


CLINICIAN’S CAPSULE
What is known about the topic?
Though government statistics exist, there is an overall paucity of data evaluating dog bite injuries.
What did this study ask?
We aimed to describe the nature of dog bite injuries, their management, and their long-term complications.
What did this study find?
Of 475 dog bites, large muscular breeds were most frequently implicated. Eleven percent of bites occurred in the head and neck region, three patients were admitted to the hospital, and a 10% infection rate was identified.
Why does this study matter to clinicians?
Educational programs for dog owners, children, and health care workers may help decrease this common source of morbidity.
INTRODUCTION
Dog bites account for the vast majority of animal-related injuriesReference Touré, Angoulangouli and Méningaud1, Reference Steele, Ma, Nakase, Moran, Mower and Ong2 and represent 1% of all emergency department (ED) visits.Reference Weiss, Friedman and Coben3 In the United States alone, it is estimated that 4.5 million people are bitten annually, 30,000 of whom require intervention by a plastic surgeon.Reference Gurunluoglu, Glasgow, Arton and Bronsert4 Interestingly, the first partial facial transplant was performed to reconstruct a facial defect following a dog attack.Reference Devauchelle, Badet, Lengelé, Morelon, Testelin and Michallet5 In addition to physical injuries, dog bites can have lasting psychological ramifications.Reference Peters, Sottiaux, Appelboom and Kahn6, Reference Gilchrist, Sacks, White and Kresnow7
Estimates indicate that there are 1.2 dogs for every North American household, a figure that is expected to rise with the increasing population.8 Issues regarding dog legislation are often highlighted in the media. Recent high-profile deaths and the legislative ban on pit bull–type dogs in Montreal, Canada, have spurred heated debates from public health experts and dog owners.Reference Boisvert9 One side has argued that poor treatment and learned behaviours are the leading cause of attacks, whereas others, particularly health advocates and medical experts, have petitioned for new legislation aimed at preventing injury.
The effects of dog bites are wide ranging. They may be as minor as superficial bruising or as serious as life- and limb-threatening injuries. While government data exist on the number and nature of dog bite injuries,10 there is a lack of large, academic studies evaluating the burden of dog bites. There has also been little research describing the interventions required to manage dog bite-related injuries. Of note, prophylactic antibiotics,Reference Tabaka, Quinn, Kohn and Polevoi11 as well as primary v. secondary wound closure,Reference Paschos, Makris, Gantsos and Georgoulis12 are ongoing controversies, with scant evidence to guide treatment. It is also not known how often dog bites become infected and whether primary closure affects the rate of infection.
We undertook a retrospective analysis of all adult (≥16 years) dog bites presenting to regional adult EDs during a 30-month period. The purpose of the study was to evaluate the nature of the dog bite, reported breeds involved, the relationship between dog and patient, nature of the injury, interventions required, services involved, management, and any long-term complications. To our knowledge, this is the largest Canadian analysis of dog bites.
METHODS
We obtained approval from our institutional research ethics board before commencing this descriptive review. All patients presenting to the three EDs in our region during a 30-month period (January 2013 to June 2015) were identified using ICD-10-CA code W54. The approximate catchment area for the reviewed EDs is 400,000 people, with an approximate volume of 138,364 patients per annum.13 Patients were followed from their initial ED presentation to the date of data collection (August to September 2016). All consultation and ambulatory care notes, operative notes, and patient care documents, as well as additional emergency visits following the patient’s first ED visit, were studied to identify any evidence of infection, complication, consultation, treatment, admission, or sequelae.
The chart review was performed independently by the lead author (AM), who was not blinded to the study hypothesis. A senior author (AS) was available for assistance if needed. As double data collection was not performed, a kappa statistic for inter-rater reliability was not calculated.
For each injury, the following information was collected: patient’s age, gender, date of injury, location of injury, relationship to dog, presence of dog owner, breed, wound characteristics (muscle involvement, soft tissue defect, vascular injury, nerve injury, injury type, and Lackmann’s classification), management (dressing, simple primary closure, complex primary closure, and main operating room repair), use of prophylactic antibiotics, type of antibiotics used, antibiotic duration, rabies prophylaxis, admission to hospital, services involved, and wound complications and characteristics.
Lackmann’s classification, which was originally applied to animal bites involving the face and neck, has been adopted herein as a method of classifying the severity of all injuries.Reference Lackmann, Draf, Isselstein and Töllner14 Complex primary closures were defined as defects requiring specialized structural repairs, such as a lip laceration or eyelid laceration. In addition, any defect repaired with local flaps was classified as a complex primary closure.
The primary objective of this study was to describe the characteristics of dog bites, including patient demographics, rates, injury location, and severity. Secondary outcomes included an assessment of an infection, complications, rates of specialty consultation, need for surgery, and rates of hospital admission.
Statistical analysis
Descriptive statistics were calculated using SPSS Version 22 (IBM SPSS Statistics, Armonk, NY). A binary logistic regression model was constructed to evaluate predictors of infection. Our model accounted for the use of prophylactic antibiotics, dog breed, injury type, injury severity, season, age, and management.
RESULTS
Sixty patients were omitted as they were under 16 years of age. A total of 475 dog bites were included in the final analysis.
Demographic data
The greatest proportion of dog bites occurred in the summer months (Table 1) (140, 30%). The majority of the patients identified were female (295, 62%), with a mean age of 41 years (standard deviation [SD] 16). In most cases, the dog was the patient’s family pet (159, 43%). The breeds identified are summarized in Table 1.
Table 1. Demographic characteristics of dog bites
* Dog breeds implicated in 108 injuries (23%). Other includes: dachshund, standard poodle, golden retriever, cocker spaniel, Staffordshire terrier, chow chow, “retriever,” Bernese Mountain dog, rottweiler, Jack Russell terrier, Boston terrier, “bull dog,” shih tzu, miniature poodle, beagle, boxer, Nova Scotia duck toller retriever, Saint Bernard, springer spaniel, Doberman, corgi, Alaskan malamute, and Leonberger.
Injury characteristics
The anatomic distribution of the dog bites is summarized in Table 2. The majority of bites occurred on the hands (264), arms (111), and legs (70). Fifty-seven injuries involving the head and neck were documented. Injury classification is summarized in Table 3. The most commonly reported type of injury was puncture (47%), followed by laceration (36%), abrasion (8%), avulsion (4%), fracture (2%), and amputations (0.4%). Of the 475 injuries, there were seven nerve injuries (one median nerve, one radial nerve, and five digital nerve injuries), ranging from neuropraxia to a complete transection; six had soft tissue defects; three injuries had muscle involvement; and three had vascular involvement. One patient had both median and radial nerve injuries. A classification of injuries using Lackmann’s criteria is summarized in Table 4.
Table 2. Dog bite frequency by body region
* Some patients have more than one type of injury. Frequency calculated as a percentage of all injuries.
Table 3. Dog bite by injury type

* Some patients have more than one type of injury. Frequency calculated as a percentage of all injuries.
Table 4. Lackmann’s classification of dog bite injuries
Management
Two hundred thirty-nine injuries (50%) required only a washout and dressing that included any wounds managed with antibiotic ointments (e.g., Polysporin®), a soft dressing (e.g., Mepore®), or both. One hundred five injuries (22%) required a simple primary closure, and 15 (3%) required a complex primary closure. The operating room was needed for the reconstruction of eight defects (2%). There were four (1%) tendon repairs, one (0.2%) nerve repair, and one injury that required a skin graft (0.2%). Two (0.2%) injuries required a closed reduction, and four (1%) required an open reduction with internal fixation. Only one of the seven nerve injuries required repair. The management modalities are summarized in Figure 1.
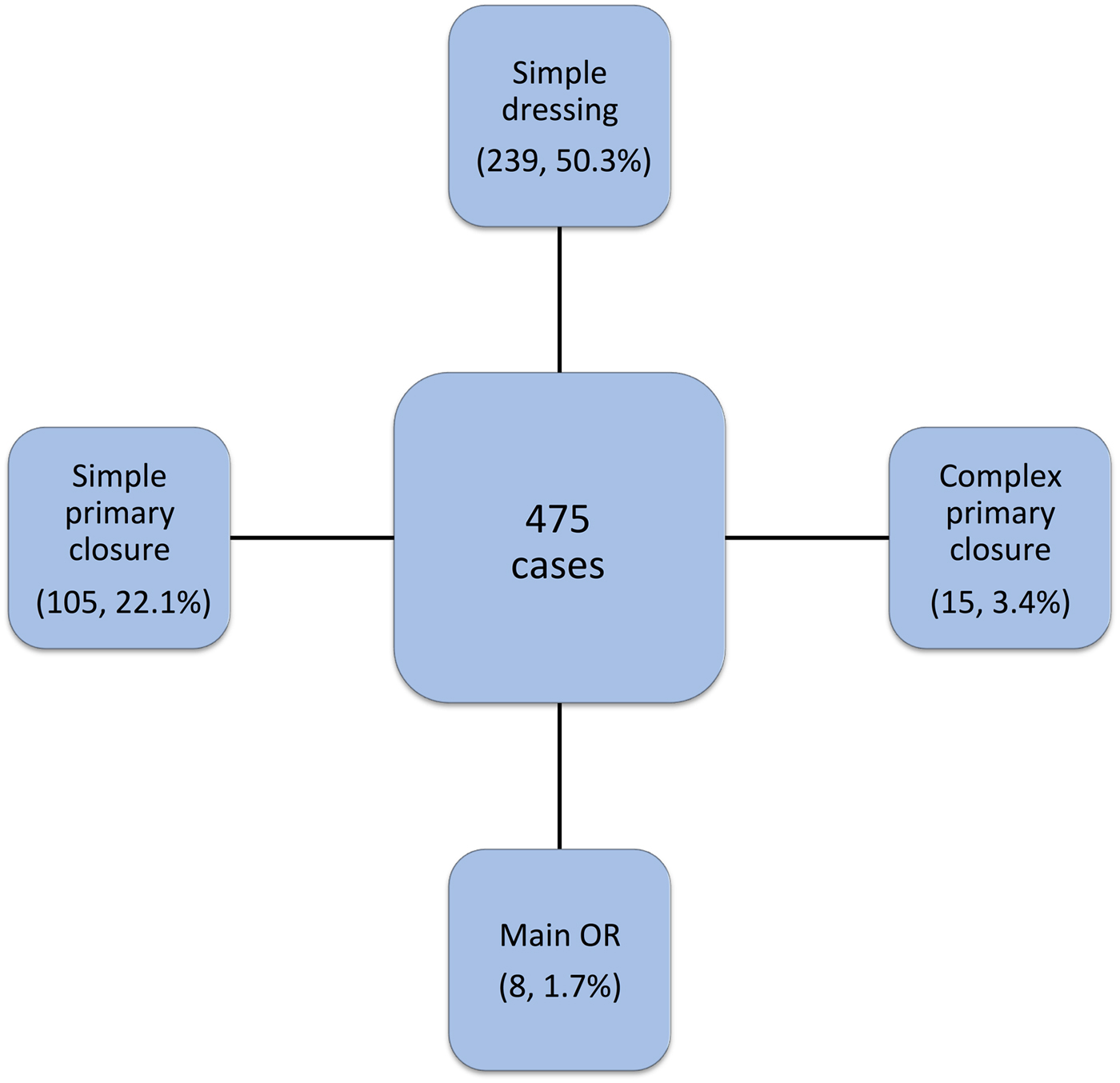
Figure 1. Treatment modalities for identified dog bites.
Prophylactic antibiotics were administered in 316 cases (67%). The most common antibiotic prescribed for dog bites was amoxicillin and clavulanate (222, 70%). Rabies prophylaxis was administered in five cases (1%). Two hundred ninety-six patients (61%) were administered a tetanus booster.
Complications
Forty-nine (10%) patients developed infections. The distribution of infection type is summarized in Table 5. Three (1%) patients were admitted to the hospital, and the average number of days spent in hospital was 3.7 (range 1–8, SD 3.8). There were no reported fatalities. There were 17 (4%) reported injury sequelae including neuropraxia, allodynia, a pin-cushioning effect of the flap following reconstruction, mallet finger, numbness, and decreased grip strength.
Table 5. Differentiation of reported infections
* Some patients had more than one infection. Frequency calculated as a percentage of all infections.
Plastic surgery was the most common specialty service involved in the care of patients with dog bites (n=53, 11%), followed by otolaryngology (n=1, 0.2%), orthopedic surgery (n=1, 0.2%), general surgery (n=1, 0.2%), and infectious diseases (n=1, 0.2%). The remainder of the patients was independently managed by emergency room physicians.
A Hosmer-Lemeshow test was not significant (χ2=0.15; p=1.00), indicating that our model was fit. No significant predictors of infection were identified (Appendix A).
DISCUSSION
This study aimed to evaluate the characteristics of dog bites affecting adults in the EDs of medium-sized Canadian cities. To our knowledge, this is the largest and most comprehensive evaluation of dog bites in Canada.
A total of 475 dog bite injuries presented to the EDs in our region over a 30-month period. Although wounds ranged in severity, the majority were fortunately minor (Lackmann Type I). Nonetheless, there were a number of more serious injuries, some requiring complex reconstructions, as well as utilization of the operating room. Specialty services were required in 12% of all cases, with the remainder of injuries independently managed by emergency physicians. The calculated infection rate for all dog bites was approximately 10%. There were three hospital admissions, ranging in duration from one to eight days. The rate of long-term functional or aesthetic disability was approximately 4%.
The results of this study are consistent with previous reports describing the anatomical distribution of dog bites.Reference Pfortmueller, Efeoglou, Furrer and Exadaktylos15 Not surprisingly, the most common site of a dog bite injury was the hand, likely the result of the nature of interactions between dogs and people. In the case of an attack, the hands are used as a defence mechanism and may be injured secondarily. Hands are of a relatively low mortality concern but have significant functionality. The face and neck are anatomically vulnerable, cosmetically important, and frequently injured in dog attacks.Reference Ullah, Tahir, Masoodurehman and Aslam16, Reference Mcheik, Vergnes and Bondonny17 Therefore, unlike the upper extremities, attacks on the head and neck pose a greater mortality risk.Reference Tsokos, Byard and Püschel18 This is particularly true in the pediatric population, in whom injuries are often more severe.Reference Kaye, Belz and Kirschner19 In one recent assessment of dog bites presenting to a large pediatric trauma centre, nearly two-thirds of all patients required an operation, with plastic surgery being the most frequently involved specialty. In addition, 91 children required tissue transfer for reconstruction of their injuries.Reference Garvey, Twitchell, Ragar, Egan and Jamshidi20 These figures suggest that in the pediatric population, the rate of surgical intervention, length of stay, morbidity, and mortality may exceed what we observed in our adult cohort.
The discrepancy in anatomical distribution between adult and children dog bites is, simply but unfortunately, a function of height and size. Children, especially infants and toddlers, still engage with their hands and interact at eye-level with a dog, leading to more face and neck injuries. Preventive strategies, which may be employed at home, include avoiding canine interaction during meal times, and in the animal’s perceived territory, factors that have been previously correlated with dog bites.Reference Reisner, Shofer and Nance21 Parents and guardians should be mindful of these factors in regards to their children, who may be unable to identify signs of aggression.
There exists great controversy over breed identification practices, particularly in the context of breed legislation and risk factors for injury.Reference Ó Súilleabháin and Doherty22 Research has suggested that visually, dog breeds are often incorrectly identified, with DNA samples matching in only approximately 25% of cases.Reference Simpson, Simpson and VanKavage23 Furthermore, by labelling certain dog breeds as “dangerous” or “high risk,” some authors have argued that it may give the false impression that certain breeds are devoid of risks of a potentially serious injury.Reference Ó Súilleabháin and Doherty22 Despite these controversies, certain breeds continuously stand out in literature on dog bites. Among these, pit bull terriers are the most frequently implicated breed,Reference Dwyer, Douglas and van As24-Reference Wu, Beres, Tashjian and Moriarty30 consistent with the results of this study. Although it may be difficult to identify breeds upon visual inspection, the pit bull terrier falls into a larger, more muscular category of dog. Large and muscular dogs are capable of generating bite forces in excess of 1800 pounds per square inch,Reference Tsokos, Byard and Püschel18 resulting in crush wounds, devascularization, and soft tissue avulsions, regardless of genetic breed categorization.Reference Kennedy, Stoll and Lauder31 Specifically, pit bull–type dogs have been shown to cause the greatest numberReference Golinko, Arslanian and Williams32 and most severe soft tissue injuries,Reference Baack, Kucan, Demarest and Smoot33 unprovoked in nearly all cases.Reference Avner and Baker34 Although correct identification of pit bull terriers may be difficult, the evidence suggests that larger, more muscular dogs cause the majority of serious dog bites and warrant careful consideration.
The most frequently encountered complication of dog bites is infection, although cat and human bites are associated with a higher risk.Reference Esposito, Picciolli, Semino and Principi35 Infections are common in bites on the head and neck, particularly with bony or vascular involvement, and in bites on the hand.Reference Talan, Citron, Abrahamian, Moran and Goldstein36 The hands are particularly susceptible to infection because of relatively low oxygen tension.Reference Pfortmueller, Efeoglou, Furrer and Exadaktylos15 Further, infections occurring in the hand can spread rapidly because of the contiguous spaces between the hand and forearm.Reference Osterman, Draeger and Stern37 A bite wound length of more than 3 cm is a significant risk factor for infection.Reference Jaindl, Grünauer and Platzer38 Wounds repaired by primary intention were historically thought to have an increased risk of developing an infection, although one recent randomized trial found no difference in infection rate between dog bites treated using primary closure and non-closure.Reference Paschos, Makris, Gantsos and Georgoulis12 The largest and most comprehensive meta-analysis of randomized controlled trials assessing the usefulness of prophylactic antibiotics determined that they may be beneficial in bites that are at an increased risk of infection.Reference Weiss, Friedman and Coben3 Despite these findings, we did not identify any significant predictors of infection, and patients administered prophylactic antibiotics were not less likely to develop an infection. In total, we identified 316 individuals who were administered prophylactic antibiotics and an infection rate of 10%. The reason for this is likely multifactorial but includes patient-related factors, resistant bacterial strains, and variables unaccounted for by our model. Prophylactic treatment with antibiotics is, therefore, a clinical decision and may be warranted in patients with larger bite wounds of the head and neck or extremities.
Multiple preventive measures aimed at decreasing the incidence and severity of dog bites have been attempted.Reference Ozanne-Smith, Ashby and Stathakis40 These include legislated control of high-risk breedsReference Patrick and O’Rourke41 and informed breed selection.Reference Gilchrist, Sacks, White and Kresnow7, Reference Gershman, Sacks and Wright42 One study from Canadian veterinary literature recommended that young children never be left alone with a dog.Reference Bandow43 The efficacy of these programs remains unclear and controversial.Reference Ozanne-Smith, Ashby and Stathakis40 More recently, there has been an attempt in the United Kingdom toward collaborative efforts among the medical community, veterinarians, and the government on the issue of dog bite prevention and management.Reference Mannion, Shepherd and Greenberg44 Educational methods such as cognitive and behavioural interventions have also been developed in an attempt to limit dog bites and have shown a small benefit in the pediatric setting.Reference Shen, Rouse and Godbole45 In a recent qualitative analysis, it was found that most dog bite victims felt that they had the knowledge to recognize aggression, often placing blame on themselves for their condition; a leading attitude among patients was that dog bites were “just one of those things.”Reference Westgarth and Watkins46 In the development of novel strategies for dog bite prevention, barriers such as these should be addressed, as this is likely key to their successful implementation.
There is a paucity of information regarding the economic impact of dog bite injuries. American figures show an increase in insurance claims, secondary to treatment and legal ramifications, from US$324 million to US$478 million in less than a decade, a number that is likely to rise.47 Similarly, dog bite injuries pose a significant cost to Canadian health care. Even with the majority of our cases being treated with a dressing alone in the ED, this puts an added burden on a strained system. From our institutional estimates, the cost of simple dog bites over a 30-month period exceeded CDN$150,000. If patient-related costs, including permanent disability and lost income, are also considered, these figures would further increase. Likewise, in the case of complex trauma and infection requiring specialty consultation, intravenous antibiotics, multiple emergency visits, and/or operative management, these conservative estimates may be surpassed.Reference Benson, Edwards, Schiff, Williams and Visotsky48
LIMITATIONS
There were limitations to our study. First, this was a retrospective review and had inherent flaws in data collection, such as missing data. The chart review was also performed independently by the lead author, who was not blinded to the study hypothesis, potentially introducing a source of bias. Additionally, given the quantity of data collected, as well as the time and cost associated with this type of collection strategy, the data were not double collected. Future studies of this nature should address this limitation to ensure quality control and adherence to reporting standards in retrospective chart reviews. The time horizon employed may have also introduced bias as it had the potential to omit important cases and trends, which were not evident in the data collected. Only data from the main adult EDs in our region were assessed. Thus, patients presenting to their primary care physicians for follow-up, a subsequent infection, or any other further treatment was not captured and may have led to an underestimation of the figures presented.
Few pediatric patients were identified, and they were often transferred to the pediatric hospital after triage. Children are most frequently bitten,Reference Touré, Angoulangouli and Méningaud1 and the figures presented in this article underestimate the prevalence of dog bites in our region. The second phase of this study, presently underway, aims to characterize our experience with pediatric dog bites. Lastly, as described earlier in this article, there were issues with accurate breed identification; therefore, the breeds identified herein best serve as an estimate.
CONCLUSIONS
This study describes the nature of adult dog bites presenting to EDs in a medium-sized eastern Canadian region. Dog bites represent a significant source of morbidity. Dog bites most commonly occurred in the hands and upper extremities and carried an infection risk of approximately 10%. Large muscular breeds were most often implicated in bite injuries. With unclear evidence on the effectiveness of breed-specific legislation at this time, we suggest that educational programs for dog owners, children, and health care workers, particularly regarding the potentially severe injuries caused by large breeds, may decrease the number and severity of attacks.
Competing interests
The authors have no financial disclosures to declare.
SUPPLEMENTARY MATERIAL
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/cem.2018.2








