



Introduction
Most psychiatric conditions begin early in life, with lifelong consequences. The global prevalence of these conditions in young people is around 13.4% (Polanczyk et al., Reference Polanczyk, Salum, Sugaya, Caye and Rohde2015) and recent studies suggest this is increasing (Collishaw, Reference Collishaw2015; Gage and Patalay, Reference Gage and Patalay2021). Psychiatric conditions can adversely impact future social and occupational opportunities (McDaid et al., Reference McDaid, Park and Wahlbeck2019; Thompson et al., Reference Thompson, Richards, Ploubidis, Fonagy and Patalay2021). One mechanism through which psychiatric conditions may influence these long-term outcomes is by negatively impacting educational outcomes (Woessmann, Reference Woessmann2016). Educational attainment can increase employment opportunities and formal education provides a structured setting for acquiring cognitive and socioemotional skills which are important throughout life (Heckman et al., Reference Heckman, Stixrud and Urzua2006). A challenge for education professionals is to support young people to complete schooling at the appropriate age, without dropouts or grade repetition, and to help them develop reading and writing literacy in addition to socio-emotional skills. All of these outcomes can increase labour market participation later in life (OECD, 2014).
Previous research supports an association between poor mental health and adverse educational attainment (Vander Stoep et al., Reference Vander Stoep, Weiss, Kuo, Cheney and Cohen2003; Breslau et al., Reference Breslau, Lane, Sampson and Kessler2008; Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009; Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015; Veldman et al., Reference Veldman, Reijneveld, Almansa Ortiz, Verhulst and Bültmann2015; Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a; Mekonnen et al., Reference Mekonnen, Medhin, Tomlinson, Alem, Prince and Hanlon2020; Wickersham et al., Reference Wickersham, Sugg, Epstein, Stewart, Ford and Downs2021). These studies found that the population attributable risk percentage (PARP) for early high school termination due to any psychiatric condition was 10.2% in the USA (Breslau et al., Reference Breslau, Lane, Sampson and Kessler2008; Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015), whereas lower figures based on cross-sectional data were found in low- and middle-income countries (LAMICs) such as Colombia (1.3%) and Mexico (0.5%) (Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009). Gaps exist, however, in understanding the relative impact of different types of psychiatric conditions on a range of adverse educational outcomes (Breslau et al., Reference Breslau, Lane, Sampson and Kessler2008; Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009, Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015; Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a).
First, most past research has focused on educational attainment (Breslau et al., Reference Breslau, Lane, Sampson and Kessler2008; Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009; Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015). For example, Mojtabai et al. (Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015) only examined non-completion of secondary school and university, or truncation of secondary education. Similarly, Dalsgaard et al. (Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a) only assessed the proportion of students taking a final examination and respective examination grades. Other indicators such as repeating a school year (or grade repetition), age-grade distortion and deficits in literacy and socio-emotional skills (which can be learned in school) may also have long-term psychosocial and occupational consequences (Jacob and Lefgren, Reference Jacob and Lefgren2009). Moreover, attainment is affected by previous grade repetition (Ikeda and Garcia, Reference Ikeda and Garcia2013) leading to age-grade distortions (i.e. being over-age for the enrolled grade); and these outcomes can also increase the risk for school dropouts (Roderick, Reference Roderick1994). Furthermore, literacy performance and social skills impact educational attainment (Zuilkowski et al., Reference Zuilkowski, Jukes and Dubeck2016) and are an educational output in their own right.
Second, as psychiatric conditions are diverse and comprise distinct phenomena, their pathways to educational attainment may also vary. However, few studies have examined the full range of psychiatric conditions (Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a). For example, a longitudinal study in the USA by Mojtabai et al. (Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015) did not include attention deficit and hyperactivity disorder (ADHD) – one of the most common psychiatric conditions in young people. Furthermore, past studies have not robustly adjusted for confounders, such as general intelligence, background socioeconomic status or race and ethnicity (Sirin, Reference Sirin2005; Deary et al., Reference Deary, Strand, Smith and Fernandes2007). Finally, few studies considered differences in educational pathways according to sex (Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a). This could be important given that males tend to have lower educational attainment and achievement rates (Voyer and Voyer, Reference Voyer and Voyer2014; Lavoie et al., Reference Lavoie, Dupéré, Dion, Crosnoe, Lacourse and Archambault2019) and higher rates of externalising conditions compared to females (Stoet and Geary, Reference Stoet and Geary2015), whereas females have higher rates of distress-related conditions (such as major depression) and are more likely to be unemployed in early adulthood (Zahn-Waxler et al., Reference Zahn-Waxler, Shirtcliff and Marceau2008; OECD, 2014) compared to males. Furthermore, Dalsgaard et al. (Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a) found that males with fear-, distress- or externalising-related conditions were less likely to take the final 9th grade examination than females with those conditions. However, females with fear- or externalising-related conditions had lower mean grades on the examination compared to males with those conditions.
This study addresses past limitations by first examining the impact of different psychiatric condition categories (i.e. fear-, distress- and externalising-related conditions) on a range of educational indicators beyond attainment (grade repetition, dropout, age-grade distortion, literacy performance and bullying perpetration behaviour) in young males and females separately, while implementing robust adjustment for confounders (McCaffrey et al., Reference McCaffrey, Ridgeway and Morral2004). Second, we estimate the proportion of adverse educational outcomes which can be attributed to psychiatric conditions and hence, might have been avoided if these conditions were fully prevented or treated, and translated these to national figures. We hypothesised that fear-, distress- and externalising-related conditions would negatively impact subsequent educational outcomes in comparison with subjects without a psychiatric condition. Considering available evidence, we hypothesised that males would experience greater negative educational impacts due to psychiatric conditions compared to females.
Methods
Sample
We analysed baseline (2010–2011) and 3-year follow-up (2013–2014) data from the Brazilian High-Risk Cohort Study for Psychiatric Conditions (BHRCS), a large school-based community cohort enriched for high family risk for psychiatric conditions (Salum et al., Reference Salum, Gadelha, Pan, Moriyama, Graeff-Martins, Tamanaha, Alvarenga, Valle Krieger, Fleitlich-Bilyk, Jackowski, Sato, Brietzke, Polanczyk, Brentani, de Jesus Mari, Do Rosário, Manfro, Bressan, Mercadante, Miguel and Rohde2015). The study was based on a screening stage and an assessment stage. At screening, on compulsory school registration days in 2010, all parents at state-funded schools, 22 schools in Porto Alegre and 35 in São Paulo, were invited to participate. In total, 8012 caregivers (87.3% mothers) agreed to be screened, with a modified version of the Family History Screen (FHS) by lay interviewers (Weissman et al., Reference Weissman, Wickramaratne, Adams, Wolk, Verdeli and Olfson2000). The FHS is a structured interview used to screen all family members for psychiatric conditions based on DSM-IV. We generated a family liability index that expresses the percentage of family members who screened positive for a psychiatric condition, adjusted for degree of relatedness (mother, father and sibling counts as 1.0, half sibling is 0.5). For full family liability index description, see Salum et al. (Reference Salum, Gadelha, Pan, Moriyama, Graeff-Martins, Tamanaha, Alvarenga, Valle Krieger, Fleitlich-Bilyk, Jackowski, Sato, Brietzke, Polanczyk, Brentani, de Jesus Mari, Do Rosário, Manfro, Bressan, Mercadante, Miguel and Rohde2015). We recruited two subgroups (one child per family): a high-risk sub-sample based on the family liability index (n = 1553) and a random subsample based on all eligible children (n = 958). These families (n = 2511) were selected for full household assessment by lay interviewers (parent interview) and trained psychologists (child interview) at baseline (6–14 years) and at follow-up (9–17 years, 80% retention). Participation was associated with higher maternal education, socioeconomic group (SEG), living in Porto Alegre, and anxiety-related conditions at baseline (Pan et al., Reference Pan, Sato, Salum, Rohde, Gadelha, Zugman, Mari, Jackowski, Picon, Miguel, Pine, Leibenluft, Bressan and Stringaris2017).
This study was approved by the National Research Ethics Commission (Comissão Nacional de Ética em Pesquisa), University of São Paulo and Federal University of Rio Grande do Sul ethics committees. Written informed consent was obtained from parents and participants that were able to read, write and clearly understand the written consent.
Psychiatric assessment
Current psychiatric conditions were assessed at baseline using parent-report on the Brazilian–Portuguese version of the Development and Well-being Assessment (DAWBA) (Goodman et al., Reference Goodman, Ford, Richards, Gatward and Meltzer2000; Fleitlich-Bilyk and Goodman, Reference Fleitlich-Bilyk and Goodman2004). The DAWBA is a semi-structured interview used to generate current DSM-IV diagnoses. Diagnostic probabilities were generated based on responses to lay interviewers. Verbatim responses as well as structured answers were then evaluated by nine trained psychiatrists who confirmed, refuted or altered initial computerised diagnostic probabilities to determine final diagnosis (overall agreement = 91%). Inconclusive cases were discussed with researchers and senior psychiatrists as described previously (Salum et al., Reference Salum, Gadelha, Pan, Moriyama, Graeff-Martins, Tamanaha, Alvarenga, Valle Krieger, Fleitlich-Bilyk, Jackowski, Sato, Brietzke, Polanczyk, Brentani, de Jesus Mari, Do Rosário, Manfro, Bressan, Mercadante, Miguel and Rohde2015).
Based on previous literature (Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015; Martel et al., Reference Martel, Pan, Hoffmann, Gadelha, do Rosário, Mari, Manfro, Miguel, Paus, Bressan, Rohde and Salum2017), conditions were grouped into three broad categories: fear-related conditions (including panic, separation and social anxiety disorder, specific phobia, agoraphobia and anxiety conditions not otherwise specified), distress-related conditions (including generalised anxiety disorder, major depressive disorder and depressive disorder not otherwise specified, bipolar, obsessive-compulsive, tic, eating and post-traumatic stress disorder) and externalising conditions (including ADHD, conduct and oppositional-defiant conditions). A dummy comorbidity variable was generated for individuals with diagnoses belonging to two or more broad categories (Table 1 for details regarding diagnostic overlap). Participants with baseline autism (n = 15) were excluded due to divergent literature as to which broad group they might belong.
Table 1. Psychiatric conditions at baseline (2010–2011) by each group
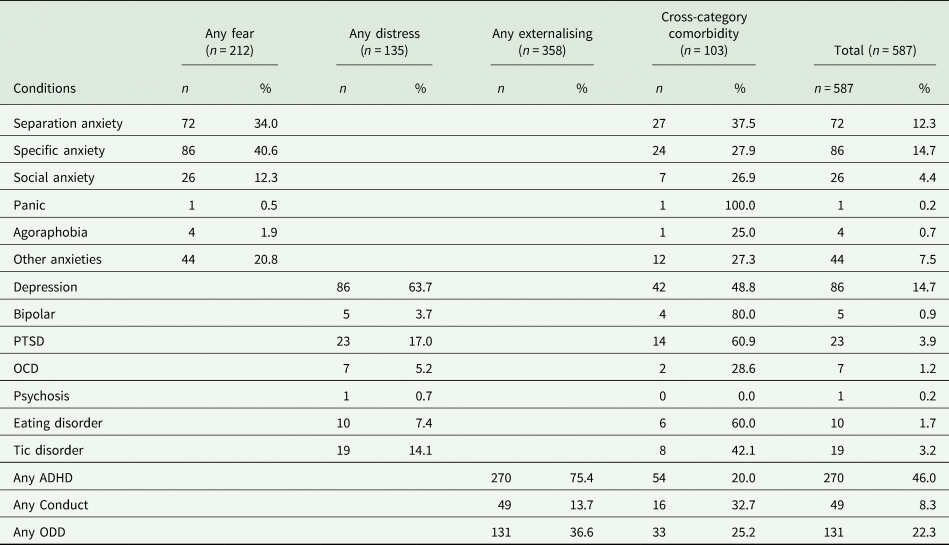
PTSD, post-traumatic stress disorder; OCD, obsessive-compulsive disorder; ADHD, attention deficit and hyperactivity disorder; ODD, oppositional-defiant disorder.
Note: Cross-category comorbidity group was defined as subjects with conditions belonging to more than one diagnostic group (comorbidity between categories). Percentages are calculated by n/total cases on condition category. Percentage in the cross-category column indicates the percentage of subjects with a cross-category comorbidity within the specific condition. Percentages may not result in 100% due to within-category comorbidity.
Educational outcomes
We considered educational outcomes reported at follow-up which had occurred since baseline. Caregivers reported on their child's grade repetition and school dropout (including expulsion). Age-grade distortion was calculated for participants reporting grade repetition, dropout or expulsion since baseline, but still enrolled in education. For these participants, age-grade distortion was measured in years and calculated by subtracting the participant's current age from the expected age range for the current school grade. For example, if a child was 12–13 years and enrolled in 5th grade (expected age 10–11 years), we estimated an age-grade distortion of 2 years. For subjects not currently enrolled in school but reporting grade repetition or dropout since baseline, to be conservative, we attributed the value of 1 year.
Reading and writing literacy was measured via the School Performance Test (‘Teste de Desempenho Escolar’ – TDE) (Salum et al., Reference Salum, Gadelha, Pan, Moriyama, Graeff-Martins, Tamanaha, Alvarenga, Valle Krieger, Fleitlich-Bilyk, Jackowski, Sato, Brietzke, Polanczyk, Brentani, de Jesus Mari, Do Rosário, Manfro, Bressan, Mercadante, Miguel and Rohde2015). We used standardised factor scores based on confirmatory factor analysis described in online Supplementary material.
We included bullying perpetration as an education-related outcome as it is an example of maladaptive peer interaction and a proxy for poor socioemotional skills (Rose et al., Reference Rose, Monda-Amaya and Espelage2011; Espelage et al., Reference Espelage, Van Ryzin and Holt2018). Bullying perpetration was assessed at follow-up in the interview with a trained psychologist using one question after the following prompt: ‘We say that a person is bullied when another person or group of people say or do unpleasant and mean things to him/her. It's also bullying when a person is repeatedly teased in a way they don't like. Examples of bullying are giving mean nicknames, humiliating, assaulting or hurting a helpless classmate, pushing, breaking and stealing belongings, chasing, isolating, ignoring, causing suffering, etc.’. After that, we asked: ‘Have you bullied another child in the past 12 months?’. Responses were ‘Yes’, ‘No’, ‘I don't know’.
Covariates
We adjusted the analyses for the following potentially confounding baseline variables on the association between psychiatric condition and educational outcomes: age; SEG; race/ethnicity, categorised as white and non-white (black, mixed, Asian and indigenous participants); intelligence (IQ); study site (due to differences in state-level legislation on retention and prevalence of psychiatric conditions) and the dummy comorbidity variable described above.
SEG was assessed using the classification from the ‘Associação Brasileira de Empresas de Pesquisa’ (Brazilian Association of Research Companies) (ABEP, 2010). Classification is made through a composite score comprising the main caregiver's educational level and household assets and conditions. A/B represent the high/comfortable class; C is considered middle class and D/E the lowest social class. SEG was considered as lower (groups C, D and E) compared against upper class (A/B) in the propensity score weighting calculation and adjusted regression analysis.
IQ was assessed by trained psychologists with the vocabulary and block design subtests of the Wechsler Intelligence Scale for Children, 3rd edition – WISC-III (Wechsler, Reference Wechsler2002), using the Tellegen and Briggs method (Tellegen and Briggs, Reference Tellegen and Briggs1967). We applied Brazilian norms (Nascimento and Figueiredo, Reference Nascimento and Figueiredo2002) and standardised the scores by age and gender.
Statistical analysis
We estimated the impact of baseline psychiatric conditions on educational outcomes at 3-year follow-up using unadjusted and adjusted regression models and using schools as the primary sampling units. Maternal education, any anxiety condition and study site predicted response at follow-up in the present sample (Pan et al., Reference Pan, Sato, Salum, Rohde, Gadelha, Zugman, Mari, Jackowski, Picon, Miguel, Pine, Leibenluft, Bressan and Stringaris2017). Therefore, we used these variables to compute inverse probability weights (IPWs) to address sample attrition in all regression analyses. Adjusted analyses included covariates (described above), baseline assessment of the outcome being estimated, IPWs and also propensity score weights (PSWs), to balance participants with and without psychiatric conditions for baseline characteristics (McCaffrey et al., Reference McCaffrey, Ridgeway and Morral2004), conducting, therefore, a doubly robust approach for the regression models (Kang and Schafer, Reference Kang and Schafer2007; Elze et al., Reference Elze, Gregson, Baber, Williamson, Sartori, Mehran, Nichols, Stone and Pocock2017). All regression models were estimated using the survey command in Stata 15.1 (StataCorp, College Station, TX).
PSWs were derived using generalised boosted modelling in the R twang package (Ridgeway et al., Reference Ridgeway, McCaffrey, Morral, Griffin and Burgette2017). This generates estimates of exposure probability based on covariates and fits several models using a regression tree and then merges predictions computed by each model. It also balances groups for covariate missingness. Interaction trees were set to 5000, shrinkage to 0.01 and two-way depth of interaction was used to minimise prediction errors by means of subsampling strategies (McCaffrey et al., Reference McCaffrey, Ridgeway and Morral2004). Balance in covariates between groups (e.g. belonging to a psychiatric condition category or not) was ascertained comparing standardised mean differences. PSWs were calculated separately for gender and psychiatric condition groups. Potential baseline confounders included in PSW estimation are described above; these were the same covariates used in the regression models. PSWs and IPWs were multiplied to generate final weights used in all adjusted models.
Population attributable risk percentage
We calculated PARPs for each educational outcome (grade repetition, school dropout, age-grade distortion and bullying perpetration) due to psychiatric condition category. Estimated PARPs can be interpreted as a percentage of adverse educational outcomes in the total population attributable to psychiatric conditions (and the percentage potentially preventable by successfully treating or preventing baseline psychiatric conditions). The PARP was computed using punaf command in Stata 15.0 (StataCorp, College Station, TX), based on weighted predicted probabilities from regression models. ‘Punaf’ generates estimates based on two scenarios: first, using predicted probabilities from the model and second, if all participants did not have a psychiatric condition. The ratio of predicted prevalence estimates from the two scenarios was then used to calculate PARPs. As we aimed to generalise to the Brazilian population, we included an additional sampling weight for PARP calculations. This sampling weight fully accounted for the family liability oversampling (see sample description). The methods and results can be found in the Supplemental material in Martel et al. (Reference Martel, Pan, Hoffmann, Gadelha, do Rosário, Mari, Manfro, Miguel, Paus, Bressan, Rohde and Salum2017). This allowed us to reweight our sample back to general population figures, achieved by setting a survey design in Stata.
For educational outcomes, we used data from the National Institute of Educational Studies and Research database to estimate the number of Brazilians to which PARPs would translate. Details of estimates are described in online Supplementary material.
Results
Participant characteristics
Table 2 describes sample characteristics, by gender, at baseline and follow-up. Males had a higher proportion of externalising-related conditions and grade repetition, age-grade distortion, bullying perpetration and lower literacy at baseline and follow-up. Table 1 describes the distribution of mental health condition categories at baseline. Fear-related conditions mostly comprised of specific phobia (40.6%), distress-related conditions major depression (63.7%) and externalising-related conditions ADHD (75.4%). Individuals with distress-related conditions had the highest cross-category comorbidity (50.3%).
Table 2. Sample description, by gender at baseline (2010–2011) and follow-up (2013–2014)
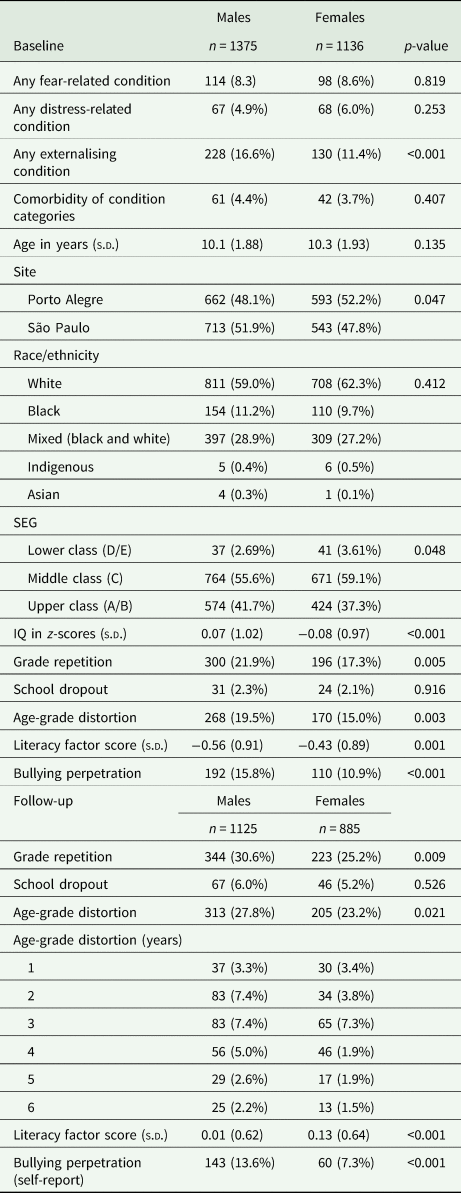
SEG, socioeconomic group measured using ABEP score; IQ, Intelligence quotient.
Potential confounders were adequately balanced (standardised mean difference <0.2) between weighted groups following application of PSWs (see online Supplementary material, Tables S1a to S3b).
Relationship between psychiatric conditions and adverse educational outcomes
Table 3 presents PSW-adjusted estimates, stratified by gender. Unadjusted results estimates are presented in online Supplementary Table S4. Full results including covariates are presented in online Supplementary Tables S5a to S7b.
Table 3. Adjusted association of baseline psychiatric condition category with subsequent educational outcomes by gender
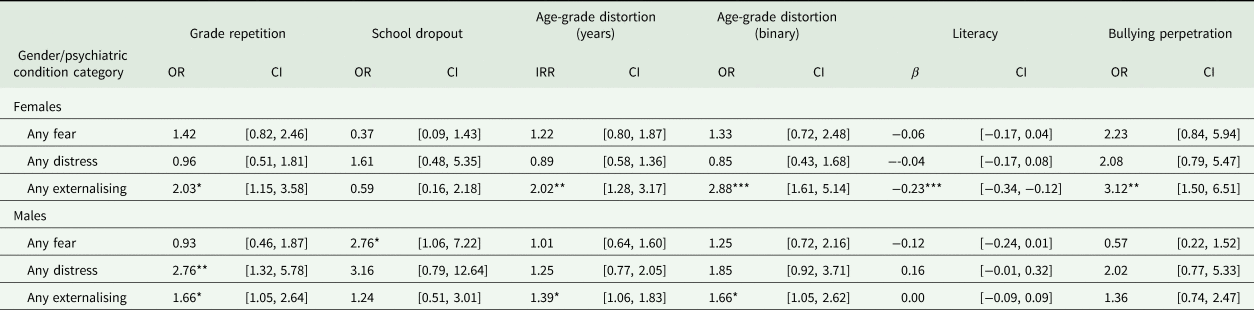
OR, odds ratio; CI, 95% confidence interval; IRR, incidence rate ratio.
Note: Models were weighted using IPWs for non-response in follow-up and propensity score weighting using condition categories as treatment variable, compared without any psychiatric condition. Covariates estimates can be found in the Supplementary material and includes baseline age, site, SEG, race/ethnicity and intelligence quotient, comorbidity with another condition category and baseline level of the specific outcome.
*p < 0.05; **p < 0.01.
Among males, fear-related conditions were associated with higher odds of school dropout, and distress-related conditions were associated with higher odds of grade repetition (Table 3). Externalising-related conditions were associated with grade repetition and age-grade distortion for males and females, and with literacy and bullying perpetration in females (Table 3).
Comorbidity between fear-, distress- and externalising-related condition categories was included as a covariate in regression models and associated estimates are presented in online Supplementary Tables S6a to S8b. Females with a comorbid condition in addition to fear-related or distress-related condition had higher odds for school dropout and age-grade distortion, respectively (online Supplementary Tables S5a and S6a). Males with fear-related or distress-related conditions who met criteria for at least one other condition category had higher odds of bullying perpetration and low literacy levels respectively (online Supplementary Tables S5b and S6b).
Population attributable risk percentage
Table 4 presents the PARP for each psychiatric condition category and estimated number of adverse educational outcomes in Brazil (reference year 2014) avoided if all conditions within categories were treated or prevented and assuming a causal relationship between psychiatric conditions and educational outcomes. When applying estimates from Table 3, weighted for high-risk sampling, we found the highest PARPs were for bullying perpetration among females with externalising diagnoses (PARP = 11.4%, 95% confidence interval (CI) = 1.5, 20.3).
Table 4. PARP of diagnostic categories for adverse educational outcomes
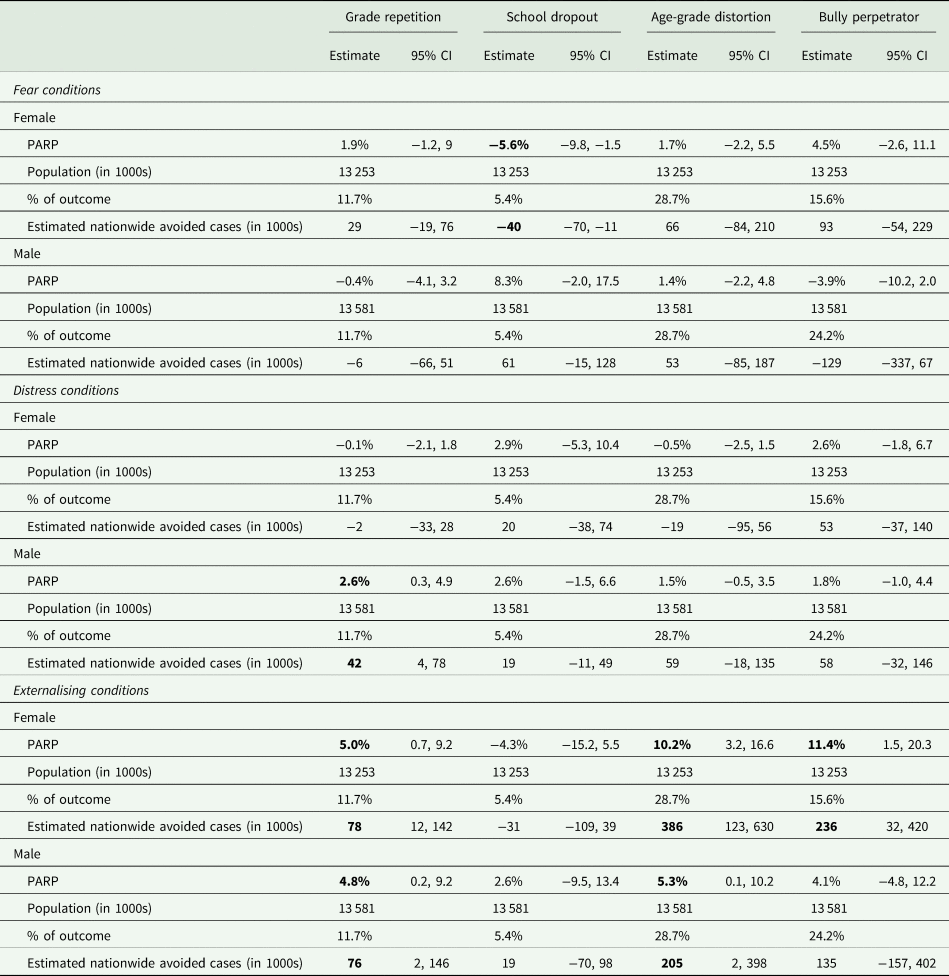
Note: Estimated avoided cases = PARP × Population in 1000s × % of outcome. PARP estimates were derived from the adjusted regression models (Table 3) and weighted for high-risk oversampling to balance for random sample. To estimate the number of people that would have benefited if mental health conditions would have been avoided, we used data from the Instituto Nacional de Estudos e Pesquisas Educacionais (INEP) to calculate the population enrolled in schools at age range for the follow-up sample, which ranged from 6 to 17 years (primary and secondary education age range) as well as the proportion of outcomes. Therefore, ‘Population’ refers to the number of males (18 661 803) and females (18 211 089) enrolled in schools multiplied by the proportion of state-funded urban students in 2014 (72.78%). The ‘% of outcomes’ were extracted from the 2014 Brazilian educational census (http://portal.inep.gov.br/web/guest/indicadores-educacionais) for grade repetition, dropout and age-grade distortion. In bold, p < 0.05.
Applying school participation estimates for 2014 in Brazil, described in online Supplementary material (p. 3), we estimate that for the Brazilian population, 154 000 cases of grade repetition (4.9% of all school repetition, 95% CI = 0.4, 9.2), 591 000 cases of age-grade distortions (7.7% of all cases, 95% CI = 1.6, 13.6) and 236 000 cases of bullying perpetration (4.4% of all cases, 95% CI = 0.6, 7.8) would have been avoided if externalising conditions were prevented or treated. As hypothesised, some differences according to gender were found, Table 4 presents estimates for males and females separately.
Discussion
Psychiatric conditions can have multiple short- and long-term impacts on individuals and society (Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015; McDaid et al., Reference McDaid, Park and Wahlbeck2019; Thompson et al., Reference Thompson, Richards, Ploubidis, Fonagy and Patalay2021). Here, we demonstrate how early psychiatric conditions can broadly impact education. Our findings highlight the independent impact of psychiatric conditions, particularly externalising conditions, on grade repetition and age-grade distortion for males and females. Moreover, we found that females experienced additional impacts associated with having an externalising condition including lower literacy ability and higher bullying perpetration. On the contrary, fear- and distress-related conditions were associated with school dropout and grade repetition in males only. Our study used PSWs to balance the condition groups for confounders, likely making our estimates more conservative; yet increases confidence of direct independent impacts. Finally, to contextualise our findings from a population perspective, we estimated that if all psychiatric conditions would have been treated or prevented, 196 000 students with grade repetition, 591 000 students with age-grade distortion and 236 000 students with bullying perpetration behaviour would have been avoided in Brazil in a 3-year period, further supporting them towards reaching future life goals. This provides evidence for the importance of effective treatment and prevention of psychiatric conditions for better educational outcomes.
Impact of externalising conditions on educational outcomes
Our findings suggest that externalising conditions had the most robust negative impacts across educational outcomes for both genders but especially for females. Individuals with externalising conditions experienced more grade repetition and age-grade distortion compared to those without these conditions. This is supported by previous literature from high-income countries showing externalising conditions are associated with a lower probability of educational completion and literacy difficulties in primary and secondary education (Carroll et al., Reference Carroll, Maughan, Goodman and Meltzer2005; Breslau et al., Reference Breslau, Lane, Sampson and Kessler2008; Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009; Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2015; Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a). Our findings demonstrate this in one of the largest LAMICs, using longitudinal data, which were not previously reported (Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009), where welfare safety nets are rare and gainful employment resulting from educational attainment can mitigate severe poverty and exclusion (Patel et al., Reference Patel, Saxena, Lund, Thornicroft, Baingana, Bolton, Chisholm, Collins, Cooper, Eaton, Herrman, Herzallah, Huang, Jordans, Kleinman, Medina-Mora, Morgan, Niaz, Omigbodun, Prince, Rahman, Saraceno, Sarkar, Silva, Singh, Stein, Sunkel and Jü2018).
Nonetheless, the impacts of externalising conditions on promoting lower literacy and higher bullying perpetration were found in females only. Previous research suggests externalising conditions are more likely to be under-detected in females compared to males (Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020b) thus, females with these conditions may also be perceived as less impaired and encouraged to take the exams, ultimately leading to lower performance in literacy and math (Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a). This may not be the case in the current study because all participants were assessed for psychopathology and literacy skills. Therefore, this could be explained in at least three alternative ways. First, this may be due to a floor effect among males who already had lower literacy and were more prone to bullying compared to females at baseline. Second, externalising conditions may develop earlier in males than in females (Hill et al., Reference Hill, Degnan, Calkins and Keane2006) and their literacy and socioemotional skills could be affected earlier on by these conditions (Carroll et al., Reference Carroll, Maughan, Goodman and Meltzer2005). A third possibility is that externalising behaviours such as impulsivity, aggression and oppositionality may be less socially acceptable in Brazilian females compared to males (Burity, Reference Burity2020). Thus, the association between externalising conditions with lower literacy and bullying perpetration may be driven by stigma and social non-acceptance, which, if addressed, could minimise these impacts. Whatever the mechanism, female students with externalising conditions may need special support to prevent, detect and treat externalising conditions early on to avoid lower literacy and higher rates of bullying behaviour.
Impact of fear- and distress-related conditions on educational outcomes
We also found gender differences among those with fear- and distress-related conditions whereby males (but not females) were more likely to experience school dropout and grade repetition, respectively. This further increases the gender disparity already experienced by males who have lower educational attainment than females (OECD, 2014; Voyer and Voyer, Reference Voyer and Voyer2014). Previous evidence suggests that young males are particularly impacted by fear- and distress-related conditions. They have greater psychological impairment and lower levels of academic attainment compared to females with the same conditions (Dunn and Goodyer, Reference Dunn and Goodyer2006; Riglin et al., Reference Riglin, Frederickson, Shelton and Rice2013; Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a). Compared with females, fear- and distress-related conditions are less likely to be detected and treated in males and consequently, they may be less likely to receive support and understanding from teachers and parents, who may perceive their poor performance as evidence of being lazy or deliberately unruly (Lavoie et al., Reference Lavoie, Dupéré, Dion, Crosnoe, Lacourse and Archambault2019; Dalsgaard et al., Reference Dalsgaard, McGrath, Østergaard, Wray, Pedersen, Mortensen and Petersen2020a). Furthermore, it is possible that males with fear- and distress-related conditions (e.g. specific phobias, depression, etc.) could be stigmatised because in many societies, Brazil included, these symptoms would not be expected or tolerated in young males. The mediation role of stigma and social norms in psychiatric conditions and educational outcomes deserves further scrutiny.
Population health and policy implications
To contextualise the population impact of psychiatric conditions, we calculated PARPs for each educational indicator. Previous research has estimated that up to 10.2% of early school termination could be attributed to psychiatric conditions (Vander Stoep et al., Reference Vander Stoep, Weiss, Kuo, Cheney and Cohen2003; Breslau et al., Reference Breslau, Lane, Sampson and Kessler2008), including a cross-sectional study using data from seven LAMICs (0–5.4%) (Lee et al., Reference Lee, Tsang, Breslau, Aguilar-Gaxiola, Angermeyer, Borges, Bromet, Bruffaerts, de Girolamo, Fayyad, Gureje, Haro, Kawakami, Levinson, Oakley Browne, Ormel, Posada-Villa, Williams and Kessler2009). Our study provided estimates linking psychiatric conditions to prior educational indicators that lead to early school termination. Moreover, after correcting for the high-risk sampling, we found that 5.6% (95% CI = 1.5, 9.8) of school dropouts were avoided in females with fear-related conditions. This might be explained by the fact that females with these conditions tend to be more frequently detected and potentially treated (Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020b).
As a practical application of our estimates, we consider the case of ADHD in Brazil. Among those with ADHD, it is estimated that only 20% receive medication treatment (Mattos et al., Reference Mattos, Rohde and Polanczyk2012). If treatment coverage increased to 30% and assuming treatment efficacy of 70% (Mattos et al., Reference Mattos, Rohde and Polanczyk2012) and considering the proportion of individuals with a diagnosis of ADHD in the externalising condition group (75.4%), according to our PARP estimates, we can estimate that 8128 (95% CI = 739, 15 253) children and adolescents would not have repeated the school year from 2013 to 2014 in state-funded urban schools (78 000 female + 76 000 male repetitions due to externalising conditions × 10 percent-point increase in ADHD coverage × 70% treatment efficacy × 75.4% of ADHD cases in the externalising group). In this example, this represents a group of young people that would have completed education on time, with their peers, with less dropout risk and a greater chance of completing higher education, ultimately leading to better employment, earnings and future life opportunities (Jacob and Lefgren, Reference Jacob and Lefgren2009; OECD, 2014; Veldman et al., Reference Veldman, Reijneveld, Almansa Ortiz, Verhulst and Bültmann2015). These findings could guide educational policy, particularly, integration of education and health sectors.
Limitations
This study has some limitations. First, cohort participants came from two large urban areas and thus findings are more generalisable to urban areas, where more than 80% of the Brazilian population lives (OECD, 2014). Therefore, we only considered students who matched sample characteristics when applying our estimates to the Brazilian population (i.e. similar age group attending state-funded urban schools). As 72.8% of the Brazilian population attended state-funded urban schools in 2014, the number of negative educational outcomes avoided might be greater if we included individuals in private schools as well as those living in rural areas. Second, due to limitations of population data, the proportion of grade repetition, dropout and age-grade distortion were assumed equal between males and females, which might underestimate male and overestimate female rates. Third, given the mean sample age of 13.5 at follow-up, we are likely not capturing the peak rate of dropout (usually 15–17 years). This could explain why psychiatric conditions were more highly associated with repetition, which happens earlier and is a risk for later dropout. Fourth, we assumed psychiatric conditions have a causal impact on educational outcomes. We used a series of adjustments to improve causal inference including applying PSWs to minimise effects of potential confounders and adjusted for autoregressive effects. Nonetheless, unmeasured confounders, such as parental values and relationship of parents with children, family environment and social support could also explain these relationships. Fifth, bullying perpetration was assessed with one self-reported question, which may raise concern on its validity. The use of a prompt to explain and exemplify what is bullying may minimise inaccuracy. Moreover, single-item assessment of bullying has been demonstrated previously as being informative of health and service use outcomes over five decades (Takizawa et al., Reference Takizawa, Maughan and Arseneault2014; Evans-Lacko et al., Reference Evans-Lacko, Takizawa, Brimblecombe, King, Knapp, Maughan and Arseneault2017).
In conclusion, the current study estimated the impact of psychiatric conditions on educational outcomes, including examining different condition categories with several widely used educational indicators. The United Nation Sustainable Development Goals recognise education as ‘one of the most powerful vehicles for sustainable development’. Our findings provide support that treatment and prevention of psychiatric conditions could prevent around 4.9% of grade repetition and 7.7% of age-grade distortion in males and females, and 11.4% of bullying perpetration behaviour and low literacy performance in females with prior externalising-related conditions. Thus, policies which encourage early intervention and collaboration between education and health sectors to support the mental health of schoolchildren can have profound consequences for lifetime opportunities and socioeconomic well-being.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796021000561.
Availability of data and materials
The data that support the findings of this study are available upon request in the Open Science Framework public repository (https://osf.io/ktz5h/) and syntax to process raw variables used in this study can also be found in gitlab (https://gitlab.com/bhrc/bhrc). Dr Hoffmann has full access to all the data used in the study, as well as analysis code (R and Stata), and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Financial Support
This work is supported by the National Institute of Developmental Psychiatry for Children and Adolescents, a science and technology institute funded by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; National Council for Scientific and Technological Development; grant numbers 573974/2008-0 and 465550/2014-2) and Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP; Research Support Foundation of the State of São Paulo; grant number 2008/57896-8 and 2014/50917-0). This work was also funded by the European Research Council under the European Union's Seventh Framework Programme (FP7/2007-2013)/ERC grant agreement no 337673, The Medical Research Council-UK, Fundação de Amparo à Pesquisa do Estado de Alagoas and Fundação de Apoio ao Desenvolvimento do Ensino, Ciência e Tecnologia do Estado de Mato Grosso do Sul. Dr. Hoffmann was supported by the Newton International Fellowship (Ref: NIF\R1\181942), awarded by the Academy of Medical Sciences through the UK Government's Newton Fund Programme. Dr. Salum is supported by the US National Institute of Mental Health (grant number R01MH120482).
Conflict of Interest
Luis Augusto Rohde: Novartis/Sandoz and Shire/Takeda in the last three years. The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by Dr Rohde have received unrestricted educational and research support from the following pharmaceutical companies in the last three years: Novartis/Sandoz and Shire/Takeda. Dr Rohde has received authorship royalties from Oxford Press and ArtMed and travel grants from Shire to take part in the 2018 APA annual meeting. Ary Gadelha: Janssen, Aché, Daiichi-Sankyo, Cristália and Torrent in the last three years. Rodrigo Affonseca Bressan: Pfizer, Torrent and Sanofi-Aventis.
The other authors declare no conflict of interest.
Ethical Standards
The authors assert that all procedures contributing to this study comply with the ethical standards and approved by the National Research Ethics Commission (Comissão Nacional de Ética em Pesquisa), the University of São Paulo and the Federal University of Rio Grande do Sul ethics committees. The authors assert that all procedures contributing to this study also comply with the Helsinki Declaration of 1975, as revised in 2008.







 Open access
Open access