



COVID-19 has typically been a mild or asymptomatic infection in children and adolescents [Reference Preston1]. However, restrictions to control the pandemic have had a significant impact on the lives of young people, for example, by disturbing their right to in-person education and social networking [Reference Engzell, Frey and Verhagen2]. Our aim was to evaluate the impact of closing lower secondary schools on COVID-19 incidence in 13–15-year-olds in Finland in a situation where strict restrictions and strong social distancing recommendations were implemented across the entire country and school closures were the sole supplementary infection control measure implemented in some areas.
Methods
COVID-19 case numbers were obtained from the National Infectious Disease Registry (NIDR) of the Finnish Institute for Health and Welfare, in which clinical microbiology laboratories report all positive SARS-CoV-2 tests with unique identifiers in a timely manner, usually within 1–3 days after testing, including information such as date of birth, gender and place of residence [Reference Sajanti3]. The NIDR is linked to population data registry, enabling calculation of incidences. We compared the rates and trends of incidences between the closure groups within different age groups (Fig. 1). The comparison of trends was performed by joinpoint regression [Reference Kim4]. All statistical analyses were performed using the open-source Joinpoint software (Joinpoint Regression Program, National Cancer Institute, USA, Version 4.9.0.0) and figures were created using RStudio (R version 3.6.3).

Fig. 1. Seven-day COVID-19 incidence per 100 000 inhabitants in areas with both restaurant and lower secondary school closures (solid line) and with restaurant closure only (dashed line) in Finland, March–April 2021. (a) 7–12, 13–15 (reference group) and 16–19-year-olds, and (b) 13–15 (reference group), 20–29 and 30–49-year-olds.
Results
We estimated the differences in trends between areas with both restaurant and lower secondary school closures and areas with only restaurant closures (defined as closure groups) in each age group (Table 1). The overall trend in incidences in the closure groups was parallel among 13–15-year-olds, (P-value for parallelism, 0.70) where the estimated average weekly per cent change in incidence (AWPC) in the combined trend was −16.4 (Table 1). The trend was also parallel among 20–29-year-olds and among 30–49-year-olds. However, among 7–12-year-olds, the overall trend in incidence was not parallel, and the AWCP was proportionally smaller in the areas with both restaurant and lower secondary school closures than in areas with only restaurant closures (Table 1). Among 16–19-year-olds, the overall trend was not parallel either.
Table 1. Comparison of restaurant and school closures to only restaurant closures by age group and comparison of age groups by closure group, sectioned by parallelism (if two groups are parallel, both groups are described by one combined trend; otherwise, both groups have own trends and difference between groups can be calculated)
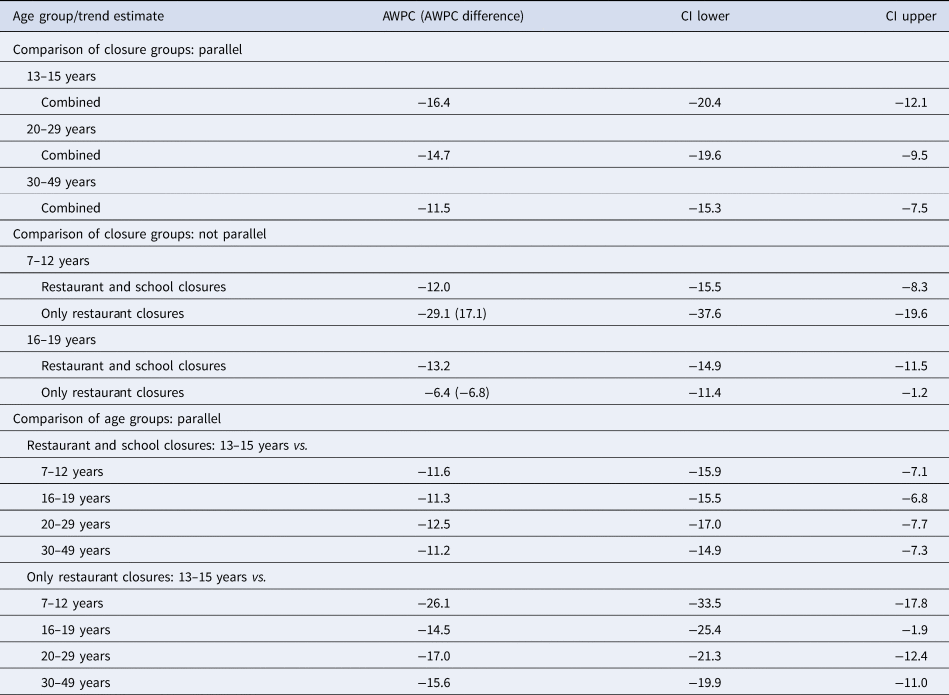
We also estimated and compared the differences in trends pairwise between age groups within the same closure group. In areas with both restaurant and lower secondary school closures, the overall trends were parallel in all cases when comparing other age groups to the 13–15-years-olds (reference group). In areas with only restaurant closures, overall trends in all age groups were also parallel, respectively.
Discussion
In the partial lockdown phase in March 2021, simultaneously with legislative restaurant closures, most areas (71.4% of total population) implemented lower secondary school closures while some kept schools open, incidentally allowing us a comparison of the impact of school closures as a separate supplementary pandemic control measure. According to our analysis, closing lower secondary schools and effectively prohibiting contacts in teenagers at schools was not associated with a larger proportional decrease in the incidence in lower secondary school aged children, nor in the incidence in any other age groups. Similar findings have been reported from Norway, where opening schools after lockdown did not lead to increased number of clusters and cases among the age group in question [5].
The number of COVID-19 cases was low in the areas with only restaurant closures meaning that even small changes in the numbers of COVID-19 cases might lead to considerable change in the AWPC value. This might explain the differences in AWCPs between the closure groups regarding 7–12-year-olds. However, the incidence of COVID-19 among children below 12 years is strongly affected by the incidence among their parents, which also may have played a role. As the areas with both restaurant and lower secondary school closures had considerably higher COVID-19 incidence, the change was likely slower in these areas in the young age groups, compared to the areas with originally lower incidence (restaurant closures only).
There are several limitations to the implementation of our results. First, the areas that did not implement school closures had, in general, lower incidence rates than the areas that did implement them. However, this was controlled by comparing proportional changes in each closure group. All other measures were similar in the study population, and the decreases in incidences can be extrapolated as the effects of general measures in place in both areas. Second, the timing for these analyses was such that it is unlikely for the cases to have been caused by the delta variant [Reference Funk6].
Our study supports earlier findings that school closures had no added effect in controlling the COVID-19 pandemic in Finland.
Acknowledgements
We are grateful to Claire Foley for proofreading the manuscript.
Financial support statement
This work was supported by the Foundation for Pediatric Research, Helsinki, Finland.
Conflict of interest
None.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author on reasonable request.



 Open access
Open access