



Introduction
According to limited studies, Chinese men who have sex with men (MSM) have a high prevalence of intimate partner violence (IPV) (Dunkle et al., Reference Dunkle, Wong, Nehl, Lin, He, Huang and Zheng2013; Davis et al., Reference Davis, Best, Wei, Luo, Van Der Pol, Meyerson, Dodge, Aalsma and Tucker2015; Liu et al., Reference Liu, Zhang, Ning, Zheng, Ding, Gao, Wong and He2018; Wang et al., Reference Wang, Wang, Chu, Zhang, Mao, Geng, Jiang, Shang and Xu2018). These studies have also reported an association between IPV and high-risk sexual behaviour or human immunodeficiency virus (HIV) infection. In addition, the positive association between IPV and adverse mental health outcomes (i.e. substance abuse and depression) in the MSM population has been well documented abroad (Buller et al., Reference Buller, Devries, Howard and Bacchus2014). However, few studies have focused on the association between mental health problems and IPV among MSM in China.
There is ample evidence that MSM are disproportionately vulnerable to various psychological problems, including depression, anxiety, substance abuse and suicidality (O'Cleirigh et al., Reference O‘Cleirigh, Magidson, Skeer, Mayer and Safren2015; Batchelder et al., Reference Batchelder, Safren, Mitchell, Ivardic and O'cleirigh2017). Research abroad has revealed that the association between IPV and mental health outcomes varies with different perpetrator-victim roles (Graham et al., Reference Graham, Bernards, Flynn, Tremblay and Wells2012; Ulloa and Hammett, Reference Ulloa and Hammett2016). It has been suggested that MSM who are victims of IPV are more likely to suffer from depressive symptoms and suicidality (Devries et al., Reference Devries, Mak, Bacchus, Child, Falder, Petzold, Astbury and Watts2013; Buller et al., Reference Buller, Devries, Howard and Bacchus2014; Parker et al., Reference Parker, Lohmus, Valk, Mangine and Ruutel2015; Kazan et al., Reference Kazan, Calear and Batterham2016), and the prevalence and severity of mental health problems are higher among individuals who are both perpetrator and victim (bidirectional violence; Ulloa and Hammett, Reference Ulloa and Hammett2016). However, few studies have measured IPV perpetration and its effect on mental health in China. Even fewer studies have examined the emergence of bidirectional violence and explored its effects on mental health (Buller et al., Reference Buller, Devries, Howard and Bacchus2014). The association between different experiences of IPV (e.g. victim v. perpetrator, physical violence v. psychological violence) and mental health problems other than depression has also been rarely studied.
However, the role of emotion regulation (ER) has attracted increasing attention in IPV and mental health research. Studies have shown that men with high ER difficulties tend to show aggressive behaviour physically and sexually (Shorey et al., Reference Shorey, Mcnulty, Moore and Stuart2015; Kirwan et al., Reference Kirwan, Lanni, Warnke, Pickett and Parkhill2019). In addition, emotional disorders can lead to a risky-taking personality and risky characteristics for a multitude of personal, emotional and mental health problems (Gross, Reference Gross2002). Two main ER strategies have been widely studied: cognitive reappraisal and expressive suppression (Gross and John, Reference Gross and John1998). Cognitive reappraisal is a form of cognitive change that involves construing a potentially emotion-eliciting situation in a way that changes its emotional effect (Lazarus and Alfert, Reference Lazarus and Alfert1964), and expressive suppression is a form of response modulation that involves inhibiting ongoing emotion-expressive behaviour (Gross and John, Reference Gross and John1998). Studies have shown that the use of cognitive reappraisal is associated with healthier affect patterns (Cutuli, Reference Cutuli2014) and that the use of suppression usually leads to adverse effects (Gross and John, Reference Gross and John2003). The meta-analysis conducted by Hu et al. (Reference Hu, Zhang, Wang, Mistry, Ran and Wang2014) also revealed that cognitive reappraisal is associated with better mental health by increasing life satisfaction and positive effects, whilst expressive suppression does the opposite.
In this context, we hypothesise that ER can moderate the association between IPV and mental health, in which cognitive reappraisal acts as a buffer against the adverse effect of IPV, whilst expressive suppression is a vulnerability factor that leads to mental health problems. The objectives of this study were (1) to explore the prevalence of different perpetrator-victim roles in different types of IPV; (2) to assess the relationships between different IPV experiences, ER and mental health problems, including suicidality, general mental health and depressive symptoms; and (3) to test the hypothesis that ER can moderate the association between IPV and mental health problems.
Methods
Participants and procedure
This cross-sectional study surveyed MSM in 15 cities across China, including five in eastern China (Sanya, Fuzhou, Hangzhou, Shenzhen and Qingdao), three in central China (Taiyuan, Changsha and Hefei), three in northeast China (Changchun, Zhengzhou and Harbin) and four in western China (Lanzhou, Nanning, Urumqi and Kunming). The participants were recruited via gay-friendly non-governmental organisations in local cities between April and June 2019. They were invited to complete a self-administered online survey, which stated that participation was anonymous and voluntary, that declining to participate would have no consequences and that the data would only be used for research purposes. The inclusion criteria were (1) age of at least 18 years, (2) men self-reported anal intercourse with at least one man in the last 6 months and (3) one or more intimate partners. In this study, ‘intimate partner’ was defined as a primary male partner that a participant was dating or with whom a participant had an ongoing intimate relationship (Davis et al., Reference Davis, Kaighobadi, Stephenson, Rael and Sandfort2016). The questionnaire took about 20 min to complete, and the participants received monetary compensation of RMB15 (about US$2.5) for their time. In total, 1233 eligible participants were approached, of whom 578 completed the online survey and were included in the final study (response rate, 46.9%).
We obtained ethical approval from the Ethics Committee of Sun Yat-Sen University ([2018] 049). In this study, we asked all participants to give their informed consent before completing the online survey, which specifically informed them that the research team would contact them if their responses revealed any suicidal ideation, suicide plans or suicide attempts. For suicidality, team members in local non-governmental organisations would call the participants, inform them about crisis intervention services and help them use these services if necessary.
Measures
Demographics
Socio-demographic information was collected, including age, city of residence, ethnicity, education level, monthly income, employment status, marital status and sexual orientation.
IPV
This study used five questions to capture five types of IPV. The specific acts described in these types of IPV were derived from the intimate partner violence among gay and bisexual men (IPV-GBM) scale, specifically developed to assess the presence of IPV among MSM (Stephenson and Finneran, Reference Stephenson and Finneran2013). This scale has excellent internal reliability (Cronbach's Alpha > 0.90) and has been used in several studies (Stephenson et al., Reference Stephenson, Hall, Williams, Sato and Finneran2013; Reference Stephenson, Freeland and Finneran2016; Stephenson and Finneran, Reference Stephenson and Finneran2017; Wei et al., Reference Wei, Hou, Hao, Gu, Dev, Cao, Peng, Gilmour, Wang and Li2019). To measure different perpetrator-victim roles in IPV (i.e., non-violence, perpetrator-only, victim-only and bidirectional violence), the answers to each question were classified into four categories: (A) I did the above to my partner; (B) My partner did the above to me; (C) Both A and B; and (D) Neither A nor B. A, B, C and D thus represented perpetrator-only, victim-only, bidirectional violence and non-violence, respectively. In addition, the participants who chose A or C were considered IPV perpetrators, and those who chose B or C were recorded as IPV victims. The Cronbach's alpha value for this scale was 0.71 in this study.
Suicidality
Suicidality covers suicidal ideation, suicide plans and suicide attempts. The participants were asked to respond to three items on their suicidality. The questions were, ‘Have you had suicidal thoughts in the past 3 months?’, ‘Have you specifically planned to commit suicide in the past 3 months?’ and ‘Have you attempted suicide in the past 3 months?’ For each item, the participants answered no (0) or yes (1). Those who answered ‘yes’ to any of the three questions were recorded as positive for suicidality (Ulloa and Hammett, Reference Ulloa and Hammett2016).
General mental health
General mental health status was measured with the 12-item general health questionnaire (GHQ-12; Goldberg and Williams, Reference Goldberg and Williams1988). This study used the GHQ scoring method (0-0-1-1) rather than that of a simple Likert scale (0-1-2-3) because this method can help eliminate any bias from participants who tend to choose answers 1 and 4 or 2 and 3, respectively (Goldberg and Williams, Reference Goldberg and Williams1988). Based on the recommendations of previous studies (Goldberg et al., Reference Goldberg, Oldehinkel and Ormel1998), the mean GHQ score (3.1) of this sample was used as a rough indicator for the cut-off point, and those who with a score greater than 3 were considered to have poor general mental health. The Cronbach's alpha value for this scale was 0.78 in this study.
Depression
A 10-item version of the Centre of Epidemiological Studies Depression Scale (CES-D) was used to confirm whether the participants had significant symptoms of depression (Radloff, Reference Radloff1977). All items were added to obtain the total scores, with a higher score indicating more severe depression. A cut-off score of 10 or higher indicated the presence of significant depressive symptoms (Miller et al., Reference Miller, Anton and Townson2008; Zhang et al., Reference Zhang, O‘Brien, Forrest, Salters, Patterson, Montaner, Hogg and Lima2012). The Cronbach's alpha value for this scale was 0.89 in this study.
Emotion regulation
ER was measured by the Emotion Regulation Questionnaire (ERQ) consisting of 10 items and divided into two independent subscales (Gross and John, Reference Gross and John2003). Six items were used to measure the participants' cognitive reappraisal (i.e. the ability to control their emotions by changing the way they think about their situation) and four items were adopted to measure expressive suppression (i.e. the ability to control their emotions by not expressing them). All items were rated on a 7-point Likert scale, ranging from strongly disagree (0) to strongly agree (6), with a higher score indicating more frequent use of ER strategies. In this sample, the ERQ had a good internal consistency with Cronbach's alpha value of 0.89 and 0.78 for cognitive reappraisal and expressive suppression, respectively.
Statistical analysis
Multiple logistic regression models were fit for the three dependent variables (i.e., suicidality, poor general mental health and significant depressive symptoms), adjusted for background variables that were significant or marginally significant in univariate analysis (p < 0.1). The adjusted odds ratios (ORa) and their 95% confidence interval (CI) were obtained. In addition, Spearman's nonparametric rho correlations were used to show the inter-correlations between the two independent variables (IPV victimisation and IPV perpetration), the two moderators (cognitive reappraisal and expressive suppression) and the three mental health outcomes (suicidality, poor general mental health and significant depressive symptoms). Hierarchical logistic regression was conducted to examine the moderating effect of ER on IPV victimisation and IPV perpetration. The variables were added in four blocks: (1) background covariates; (2) IPV victimisation or IPV perpetration; (3) ER subscales (i.e., cognitive reappraisal and expressive suppression); and (4) interaction terms (i.e., IPV victimisation × cognitive reappraisal, IPV victimisation × expressive suppression, IPV perpetration × cognitive reappraisal, IPV × expressive suppression). A p value of 0.05 was set as the level of statistical significance. All analyses were conducted in SPSS version 25.
Results
Descriptive statistics
Most participants (62.8%) were younger than 30 years. More than half had completed university education (54.3%) and worked full-time (66.1%). In addition, most were homosexual (81.3%) and unmarried (51.2% were single and 36.0% had a boyfriend[s]). Details are listed in Table 1. Overall, we found no socio-demographic difference between the perpetrators and the non-perpetrators or between the victims and the non-victims (p < 0.05).
Table 1. Socio-demographic Characteristics of sample MSM population
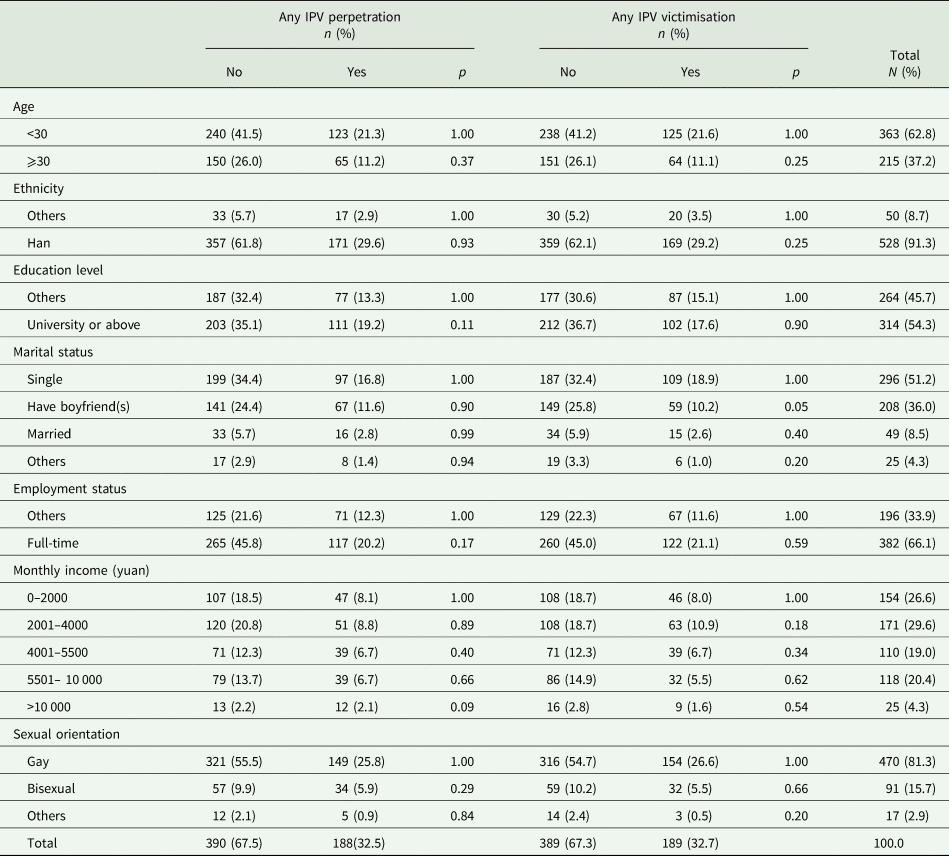
n = number of subjects, N = number of total subjects, % = proportions.
In addition, the lifetime rate of IPV victimisation was 32.7% (189/578) and the lifetime rate of IPV perpetration was 32.5% (188/578). To be more specific (Table 2), among the five types of IPV, sexual violence victimisation (6.9%, 40/578) led more frequently to victim-only experiences, followed by monitoring behaviour victimisation (5.7%, 33/578). In terms of perpetrator-only experiences, people who perpetrated monitoring behaviour (5.9%, 34/578) and emotional violence (5.4%, 31/578) ranked first and second, respectively. Similarly, bidirectional violence was most often found in cases of emotional violence (11.8%, 68/578) and monitoring behaviour (9.3%, 54/578). The rate of bidirectional violence was higher than that of perpetrator-only and victim-only violence in cases of physical, monitoring and emotional violence, and the rate of victim-only violence in cases of sexual violence was higher than that of perpetrator-only or bidirectional violence.
Table 2. Descriptive statistics of lifetime IPV experience

n = number of subjects, % = proportions.
In this study, 36.0% (208/578) of the participants had significant depressive symptoms based on the CESD-10. In addition, 42.6% (246/578) were in poor general mental health based on the GHQ-12. In the past 3 months, 13.7% (79/578) reported suicidal ideation, 3.1% (18/578) had plans to commit suicide and 2.4% (14/578) had actually attempted suicide, resulting in a rate of suicidality 14.0% (81/578).
The mean scores for cognitive reappraisal and expressive suppression were 31.4 (s.d. = 5.7) and 16.0 (s.d. = 4.6), respectively. Cognitive reappraisal showed a negative association with the three adverse mental health outcomes adjusted for background variables (ORa = 0.98–0.92), whilst expressive suppression did not show a significant association with any of the three mental health outcomes.
Associated factors of suicidality
In univariate analysis, age, ethnicity and marital status showed significant or marginally significant associations with suicidality, which were included in the adjusted multivariate logistic regression as controlled variables. Victim-only experiences of physical violence (ORa = 3.22, 95% CI = 1.11–9.32), victim-only experiences of sexual violence (ORa = 2.90, 95% CI = 1.39–6.05) and IPV victimisation (ORa = 1.90, 95%CI = 1.17–3.09) showed significant associations with suicidality in multivariate analysis. Similarly, adjusted logistic regression revealed that perpetrator-only experiences of monitoring behaviour (ORa = 2.93, 95% CI = 1.30–6.60), bidirectional experiences of monitoring behaviour (ORa = 3.01, 95% CI = 1.49–6.05) and IPV perpetration (ORa = 1.71, 95% CI = 1.05–2.79) showed positive associations with suicidality (Table 3).
Table 3. Adjusted logistic regression analysis of IPV experience and mental health outcomes
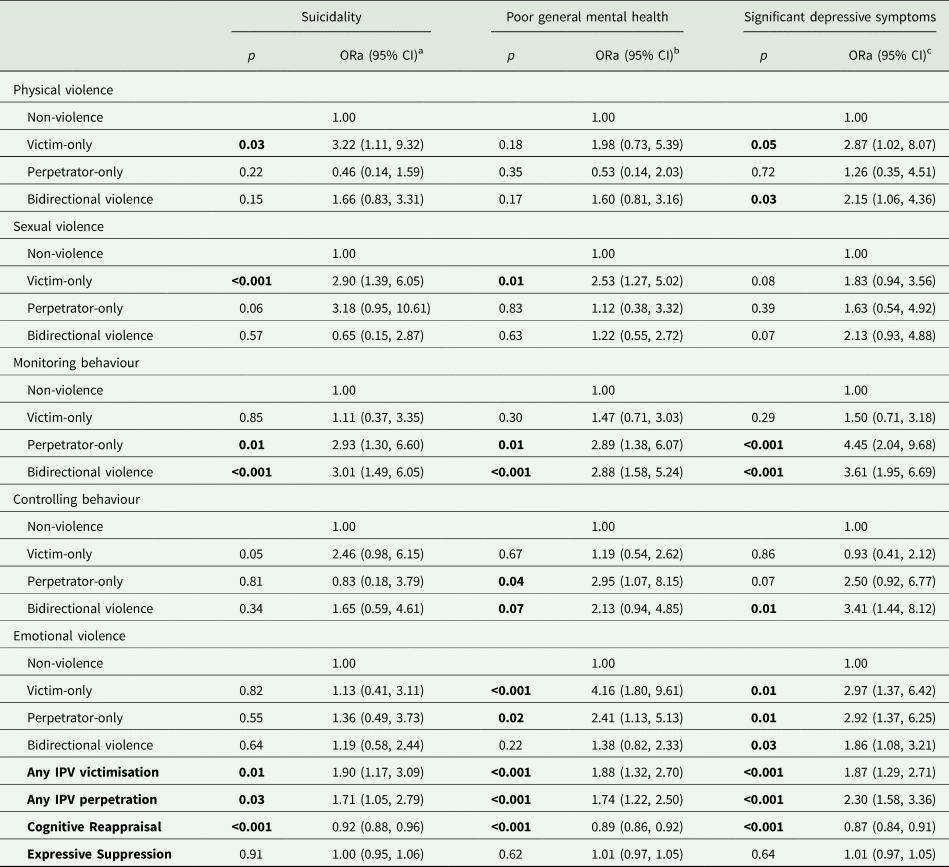
a Adjusted for Age; Ethnicity; Marital status.
b Adjusted for Marital status; Monthly income.
c Adjusted for Age; Ethnicity; Marital status; Monthly income.
ORa, adjusted odds ratio, p < 0.05 considered significant (in bold).
Associated factors of poor general mental health
Adjusted for marital status and monthly income, IPV victimisation (ORa = 1.88, 95% CI = 1.32–2.70) and IPV perpetration (ORa = 1.74, 95% CI = 1.22–2.50) showed significant associations with poor general mental health. Other significant factors of poor general mental health included (Table 3): (1) victim-only experiences of sexual violence (ORa = 2.53, 95% CI = 1.27–5.02) and emotional violence (ORa = 4.16, 95% CI = 1.80–9.61); (2) perpetrator-only experiences of monitoring behaviour (ORa = 2.89, 95% CI = 1.38–6.07), controlling behaviour (ORa = 2.95, 95% CI = 1.07–8.15) and emotional violence (ORa = 2.41, 95% CI = 1.13–5.13); and 3) bidirectional experiences of monitoring behaviour (ORa = 2.88, 95% CI = 1.58–5.24) and controlling behaviour (ORa = 2.13, 95% CI = 0.94–4.85), after adjustment.
Associated factors of significant depressive symptoms
After adjusting for age, ethnicity, marital status and monthly income, the following variables showed significant associations with significant depressive symptoms (Table 3): (1) victim-only experiences of physical violence (ORa = 2.87, 95% CI = 1.02–8.07) and emotional violence (ORa = 2.97, 95% CI = 1.37–6.42); (2) perpetrator-only experiences of monitoring behaviour (ORa = 4.45, 95% CI = 2.04–9.68) and emotional violence (ORa = 2.92, 95% CI = 1.37–6.25); (3) bidirectional experiences of physical violence (ORa = 2.15, 95% CI = 1.06–4.36), monitoring behaviour (ORa = 3.61, 95% CI = 1.95–6.69), controlling behaviour (ORa = 3.41, 95% CI = 1.44–8.12) and emotional violence (ORa = 1.86, 95% CI = 1.08–3.21); and (4) IPV victimisation (ORa = 1.87, 95% CI = 1.29–2.71) and IPV perpetration (ORa = 2.30, 95% CI = 1.58–3.36).
Interaction between ER and IPV on mental health problems
As shown in Table 4, significant correlations were seen (1) between one potential moderator (i.e., cognitive reappraisal) and the dependent variables (i.e., the three mental health outcomes); (2) between one potential moderator (i.e., cognitive reappraisal) and the independent variables (i.e., IPV victimisation and IPV perpetration); and (3) between the independent variables and the dependent variables. However, only the moderating effect of cognitive reappraisal was found in the association between IPV victimisation and poor general mental health (B = 0.07, p < 0.05; Table 5). This moderating effect indicated that a higher level of cognitive reappraisal mitigated the adverse effects of IPV experiences on general mental health more among non-victims than among victims.
Table 4. Correlations of study variables
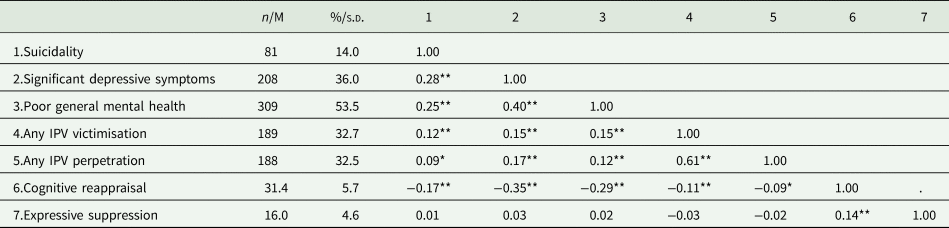
n, number of subject; M, mean; %, proportions; s.d., standard deviation.
* p < 0.05, **p <0.01.
Table 5. Final model for cognitive reappraisal and any IPV victimisation predicting poor mental health

# p < 0.1, * p < 0.05, **p < 0.01, *** p < 0.001.
Discussion
This study investigated the lifetime prevalence of IPV and examined its association with mental health problems among MSM in China. The results confirmed the high prevalence of IPV in this population reported in previous studies (18.7%–51.0%; Dunkle et al., Reference Dunkle, Wong, Nehl, Lin, He, Huang and Zheng2013; Davis et al., Reference Davis, Best, Wei, Luo, Van Der Pol, Meyerson, Dodge, Aalsma and Tucker2015; Ibragimov et al., Reference Ibragimov, Harnisch, Nehl, He, Zheng, Ding and Wong2017; Li and Zheng, Reference Li and Zheng2017; Liu et al., Reference Liu, Zhang, Ning, Zheng, Ding, Gao, Wong and He2018; Wang et al., Reference Wang, Wang, Chu, Zhang, Mao, Geng, Jiang, Shang and Xu2018). We also found that the prevalence of bidirectional violence in cases of physical violence, monitoring behaviour and emotional violence was higher than that of perpetrator-only and victim-only violence. In other words, among these three types of violence, it is more likely to find a reverse cycle between the perpetrator and the victim, which may lead to more violent conditions.
In 2015, China passed its first law against domestic violence, which provides additional protection to minors, the elderly, people with disabilities, pregnant and lactating women, and seriously ill patients who suffer violence, but it ignores sexual minorities, such as MSM (Burki, Reference Burki2017). Chinese MSM largely live in a heteronormative and homophobic environment (Zhang and Chu, Reference Zhang and Chu2005; Steward et al., Reference Steward, Miège and Choi2013; Burki, Reference Burki2017) and IPV in same-sex couples is relatively more invisible than in heterosexual couples. Due to the current absence of relevant laws and regulations against discrimination and domestic-violence, homosexual victims do not have access to adequate services and legal protection. This may further increase the effects of IPV on the mental health of Chinese MSM. The high prevalence of mental health problems found in this study (14.0% for suicidality, 53.5% for poor general mental health and 36.0% for significant depressive symptoms) is consistent with that of previous studies among MSM in China (10.6%–18.3% for suicidal ideation, 49.4% for poor general health and 26.8%–37.2% for depression; Mu et al., Reference Mu, Li, Liu, Na, Yu, Bi, An, Gu, Zhou, Li, Zhang, Jiang and Pan2016; Li et al., Reference Li, Cai, Wang, Sun, Zhu, Tian, Jiang and Gan2016; Su et al., Reference Su, Zhou, Li, Shi, Huan, Yan and Wei2018; Wang et al., Reference Wang, Wang, Chu, Zhang, Mao, Geng, Jiang, Shang and Xu2018; Zhu et al., Reference Zhu, Liu, Chen, Zhang and Qu2018). In addition, this study discussed the effect of IPV, as a risk factor, and ER, as a potential moderator on the mental health of Chinese MSM.
Previous studies have focused mainly on the relationship between victims of violence and adverse psychological outcomes. Other roles, such as perpetrators of violence and bidirectional violence, and other forms of violence (e.g., emotional violence, controlling behaviour) have been less studied (Buller et al., Reference Buller, Devries, Howard and Bacchus2014; Brown et al., Reference Brown, Serovich and Kimberly2016; Ibragimov et al., Reference Ibragimov, Harnisch, Nehl, He, Zheng, Ding and Wong2017). Therefore, one of the strengths of this study is that we investigated IPV in detail based on four roles and five types of violence and their specific effects on mental health. The results suggest that the roles of perpetrator and victim may have important implications for individual mental health status. For example, victims of physical and sexual violence were more likely to report suicidality than perpetrators, whilst the perpetrators of controlling and monitoring behaviours were more likely to have mental health problems than the victims. Previous studies of heterosexual couples found that different roles in violent experiences can have different effects on mental health problems (Anderson, Reference Anderson2004; Graham et al., Reference Graham, Bernards, Flynn, Tremblay and Wells2012; Ulloa and Hammett, Reference Ulloa and Hammett2016). Overall, these studies have suggested that when designing interventions to improve the mental health status of MSM, attention should be paid to both the victims, especially victims of physical and sexual violence, and perpetrators, especially perpetrators of psychological violence (i.e. emotional violence, monitoring and controlling behaviour).
Although the concept of ER was first proposed and studied in western countries (Gross and John, Reference Gross and John1998; Gross, Reference Gross2002), it has been widely applied in eastern countries, including China, to study its effect on mental health in various populations. Hu et al.'s (Reference Hu, Zhang, Wang, Mistry, Ran and Wang2014) meta-analysis with a sample of 9454 Chinese participants and 8970 Western participants indicated that the correlation between expressive suppression and negative indicators of mental health (e.g. depression, anxiety and negative affect) was stronger in the Western cultural values category than in the Eastern cultural values category, whilst this cultural difference was not significant for cognitive reappraisal. Our results are consistent with those of previous studies. Many Eastern cultures such as China are deeply influenced by Confucianism. The Chinese collectivist culture emphasises social norms and group harmony and values individual restraint and the suppression of socially inappropriate emotions to maintain overall harmony. Therefore, expressive suppression may not have a negative effect on people who share this cultural value because it is consistent with their social value system (Hu et al., Reference Hu, Zhang, Wang, Mistry, Ran and Wang2014). In addition, in response to the heteronormative culture prevalent in China, MSM may be used to hide their emotions, such as concealing their sexual orientation for social acceptance. Thus, expressive suppression may have a limited effect on the mental health of Chinese MSM (Sun et al., Reference Sun, Pachankis, Li and Operario2020).
The cultural context discussed above explains to some extent the results of this study. However, our results differ somewhat from our hypothesis because we found no significant association between expressive suppression and mental health. The buffering effect of cognitive reappraisal was found only in the association between IPV victimisation and poor general mental health, whilst higher cognitive reappraisal was significantly associated with better general mental health. ER is a complex psychological process influenced by many factors. Therefore, follow-up studies should examine relevant influencing factors, such as the cultural background, and further explore the mechanism of different ER strategies. Although GHQ scores decreased as the cognitive reappraisal scores increased in the victim group, this trend was not as significant as in the non-victim group. This indicates that cognitive reappraisal may be insufficient to mitigate the adverse effect of IPV victimisation on mental health in this population. Therefore, programs that seek to prevent mental health problems among MSM should integrate ER and other effective measures in their curriculum for IPV victims.
Studies of the different roles in IPV experiences and their effect on mental health among Chinese MSM have been limited. Therefore, this study is one of the first to examine the moderating effect of ER on the association between IPV and mental health. Moreover, the study sample included MSM from 15 cities across China, which makes the results more representative and generalisable. Despite these strengths, this study has several limitations. First, IPV is a taboo subject globally regardless of sexual orientation, gender and culture, for both perpetrators and victims. Therefore, the results of this study may be underestimated, thus affecting the identified effect of ER on IPV and mental health. Second, the ERQ is a widely used measure of ER developed in Western culture, and suppression is explicitly defined as one of its regulation modes (Gross and John, Reference Gross and John2003). However, the suppression subscale includes only four items, which may not have enough power to differentiate participants in the Chinese context. Thus, the validity of this subscale did not allow us to explore the association of expressive suppression with IPV and ER.
Conclusions
This study explored the prevalence of different perpetrator-victim roles in different types of IPV experiences, confirmed the adverse effect of IPV on mental health and tested its potential moderators among MSM in China. The effect of IPV on mental health differs due to different perpetrator-victim roles. Therefore, this study offers new insights into the development of prevention and intervention strategies. Targeted mental health inventions for MSM with IPV experiences should be tailored to their roles. In addition, cognitive reappraisal, as a protective factor for mental health, may not play a full role in victims of violence. Therefore, integrated interventions are needed for victims. Further research is warranted to investigate the effects of different perpetrator-victim roles in IPV experiences on mental health and identify potential positive moderators.
Data
The data sets used and analysed in the study are available from the corresponding author on reasonable request.
Acknowledgements
The authors would like to thank all participants in this study and all field workers for their support during the data collection.
Author contributions
The manuscript was read and approved by all named authors and they all contributed to the development of this research.
Financial support
This work was financially supported by the National Natural Science Foundation of China (Nos. 81803334, 71774178), the Natural Science Foundation of Guangdong Province (No. 2017A030310561), a Major Infectious Disease Prevention and Control of the National Science and Technique Major Project (No. 2018ZX10715004), the Science and Technology Planning Project of Guangdong Province (No. 2017A020212006), the Science and Technology Research Project of Guangzhou (No. 201607010368), and the China Medical Board (No. 18-301).
Conflict of interest
There are no known conflicts of interest associated with this article.
Ethical standards
Ethical approval for the study was obtained from the Ethics Committee of Sun Yat-Sen University ([2018] 049).






 Open access
Open access