


Introduction
Granulysin is a recently discovered cytolytic protein of natural killer (NK) cells and cytotoxic T lymphocytes (CTL) [Reference Krensky and Clayberger1]. Normal values of granulysin in the serum of healthy persons are 3.7 ± 3.2 ng/ml. There are also some studies which suggest the role of CD4 + T lymphocytes as secretory molecules of granulysin. Two molecular forms of granulysin, the 15 kDa precursor and 9 kDa mature form, are produced in these cells. The 15 kDa form is constitutively secreted, and its function remains poorly understood. The 9 kDa form is released by receptor-mediated granule exocytosis [Reference Hanson2]. Nine kDa granulysin is broadly cytolytic against tumours and microbes, including Gram-positive and Gram-negative bacteria, fungi and parasites. Similar to other cytolytic granule proteins, granulysin is released upon stimulation into the intercellular space between effector and target cells via a granule exocytosis pathway. Exposure to granulysin accelerated death of infected cells as assessed by apoptosis markers [Reference Okada3]. Recent experiments indicate an important role of granulysin in immunity to Mycobacterium tuberculosis and Mycobacterium leprae, so as Plasmodium falciparum and Cryptococcus neoformans [Reference Stenger4].
Chickenpox is a highly contagious viral infection which mainly affects children. Primary varicella-zoster (VZV) infection elicits immunoglobulin G, immunoglobulin M and immunoglobulin A antibodies, which bind to many classes of viral proteins [Reference Arvin5].
Studies of healthy and immunocompromised patients with primary or recurrent VZV infections demonstrate the importance of virus-specific cellular immunity for controlling viral replication [Reference Arvin6]. CD4 (helper) and CD8 (cytotoxic) T lymphocytes play a critical role in the protection against VZV primary infection and reactivation.
Methods
Subjects
This was a prospective study, approved by the Ethics Committee of the Clinical Center University of Sarajevo, with approval nr. 0207–1205. Sixty-nine patients who have been treated in the Clinical Center University of Sarajevo, Bosnia Herzegovina, in the period June 2014–January 2016 with confirmed chickenpox infection were enrolled in the study. Another 12 did not meet inclusion criteria and were rolled-out from the study. All of them were admitted in the outpatient ambulance for a first clinical examination. We took data for sex, age, possible contact with chickenpox, and according to the presented symptoms and signs of disease, patients were divided in two groups: 34 with mild and 35 with moderate, severe or life-threatening clinical presentation. Patients with mild clinical presentation had all characteristic symptoms and signs of disease but no complications, and required only symptomatic therapy, while acyclovir was prescribed to elderly patients. Patients with moderate or severe clinical presentation had at least one complication, required hospitalisation and a combination of antiviral, antibiotic and symptomatic therapy. Patients with life-threatening clinical presentation had multiple complications, which required multidisciplinary treatment with specialists for other clinical diseases. Thirty healthy volunteers served as a control group. They were employees of the Clinical Center University of Sarajevo, who met inclusive criteria: age, sex, health status. We took peripheral blood samples to detect the levels of granulysin and CD4, CD8 and NK cells from all patients and healthy controls and stored at −80°C until use. Blood samples are taken in first 3 days after beginning of the rash: in 17 patients first day, 25 second day and 27 third day. The testing was performed next week after all blood specimens have been collected (January 2016). Informed consent was obtained from all subjects.
ELISA for granulysin
For detection and quantification of granulysin in the sera, ELISA test was performed. We used LEGEND MAX™ Human Granulysin ELISA Kit from BioLegend, San Diego, CA, USA. In brief, in 96-well flat-bottomed plates, we added reconstituted dilution of human granulysin, with the highest concentration of 40 ng/ml in the first tube and 20, 10, 5, 2.5, 1.25 and 0.63 ng/ml, respectively. The plate was washed four times with wash buffer. A 50 µl of buffer was added to each well. The plate was sealed and incubated at room temperature for 2 h while shaking at 200 rpm. The content of the plate was discarded into the sink, then washed four times with wash buffer. One hundred microlitres of human granulysin detection antibody solution was added to each well, the plate was sealed and incubated at room temperature for 1 h while shaking. Then, the contents of the plate were discarded into the sink, then again washed four times with the buffer. Avidin-HRP D solution in a quantity of 100 µl was added to each well, plate was sealed and incubated at room temperature for 30 min while shaking. Again, we discarded the contents of the plate into the sink, washed the plate five times with wash buffer and soaked the wells in wash buffer for 30 s to 1 min for each wash. Finally, we added 100 µl of substrate solution F to each well and incubated for 20 min in the dark. The reaction was stopped by adding 100 µl of stop solution to each well. The absorbance was measured at 450 nm within 30 min.
Flow cytometry detection of CD4, CD8 and NK cells
Whole blood is aseptically collected by venepuncture to a sterile EDTA vacutainers tube in amount of 5 ml. White blood cell counts and differential cell count are obtained from the same specimen. Anticoagulated blood was stored at room temperature and analysed same day. The tubes were vortexed at low speed to reduce aggregation before running them on the flow cytometer. We used BD Multitest™ six-colour direct immunofluorescence TBNK reagent in a BD FACSCanto™ and BD FACSCanto™ II flow cytometer for detection and identification, or the percentage of the absolute number of T and B lymphocytes, NK cells and CD4/CD8 subpopulations.
Statistical analysis
Results are expressed as minimal, maximal and median value with standard deviation (s.d.). Frequency distribution between the groups were compared using one-way analysis of variance (ANOVA). Frequency distribution between the two groups were compared using the χ 2 test. Correlations between serum granulysin levels and other variables were analysed with Spearman's rank correlation test. All P-values were two-tailed, and the level of significance was set at P < 0.05. Multivariate logistic regression analysis with a stepwise backward selection included variables showing P < 0.05 in univariate analyses. All statistical analyses were performed using SPSS for windows version 15.0 (SPSS Inc, Chicago, Illinois, USA).
Results
The median age in the group with mild presentation was 24.57 (range 3–54 years, s.d.= 14.14), while in the other group, it was 28.47 (range 5–49 years, s.d. = 10.39). The χ 2 test found no statistical difference between the groups for age of the patients. In a group with mild presentation, women were dominant (64.7%), while in another group, men were dominant (71%). Except for respiratory symptoms and fever, there was no significant difference in clinical signs and symptoms between the two groups.
In a group of mild presentation, we found no complications of chickenpox. In another group of patients, complications were present in all patients. A number of complications vary, from one to three. Most of the complications were bacterial superinfections of skin and pneumonia, while other complications were presented in smaller number. We had 23 (28%) patients with one, 10 (17%) with two and two (4%) with three complications. Antiviral therapy (acyclovir) was given to 13 patients in a group with mild presentation, while all patients in another group received acyclovir. In a group with mild, severe or life-threatening chickenpox, 28 patients required antibiotic for treatment of secondary infections.
Mean percentage of CD4T-lymphocyte count was 28.20, with a range from 0.00 to 49.60 and an s.d. of 12.70. In the group of outpatients, mean value was 44.06, with a range from 20.30 to 80.00 and an s.d. of 11.48. In the control group, median was 44.26, with a range from 28.00 to 57.60 and an s.d. of 6.69. Using ANOVA test, we found significant differences between the groups of hospitalised patients and outpatients (P < 0.0001) as well as hospitalised patients and control group (P < 0.0001).
In a group of hospitalised patients, mean percentage of CD8T cells was 38.34, with a range from 16.50 to 84.20 and an s.d. of 15.52. In the group of outpatients, mean value was 30.15, with a range from 9.90 to 56.00 and an s.d. of 9.46. In the control group, mean value was 28.40, with a range from 14.00 to 42.10 and an s.d. of 7.34. We compared these values using ANOVA test and found significant difference between the groups of hospitalised patients and outpatients (P = 0.011) as well as hospitalised patients and control group (P = 0.02).
In a group of hospitalised patients, mean percentage of CD16/56 cells (NK cells) was 15.27, with a range from 2.40 to 40.00 and an s.d. of 7.90. In the group of outpatients, mean value was 15.78, with a range from 1.40 to 33.10 and an s.d. of 7.24. In the control group, mean value was 15.92, with a range from 4.00 to 39.20 and an s.d. of 7.10. The ANOVA test shown no significant difference between the groups.
Serum granulysin level in a group with mild presentation was in a range from 0.00 to 5.60 ng/ml with a median value of 0.95 ng/ml and s.d. = 1.12 (Fig. 1).
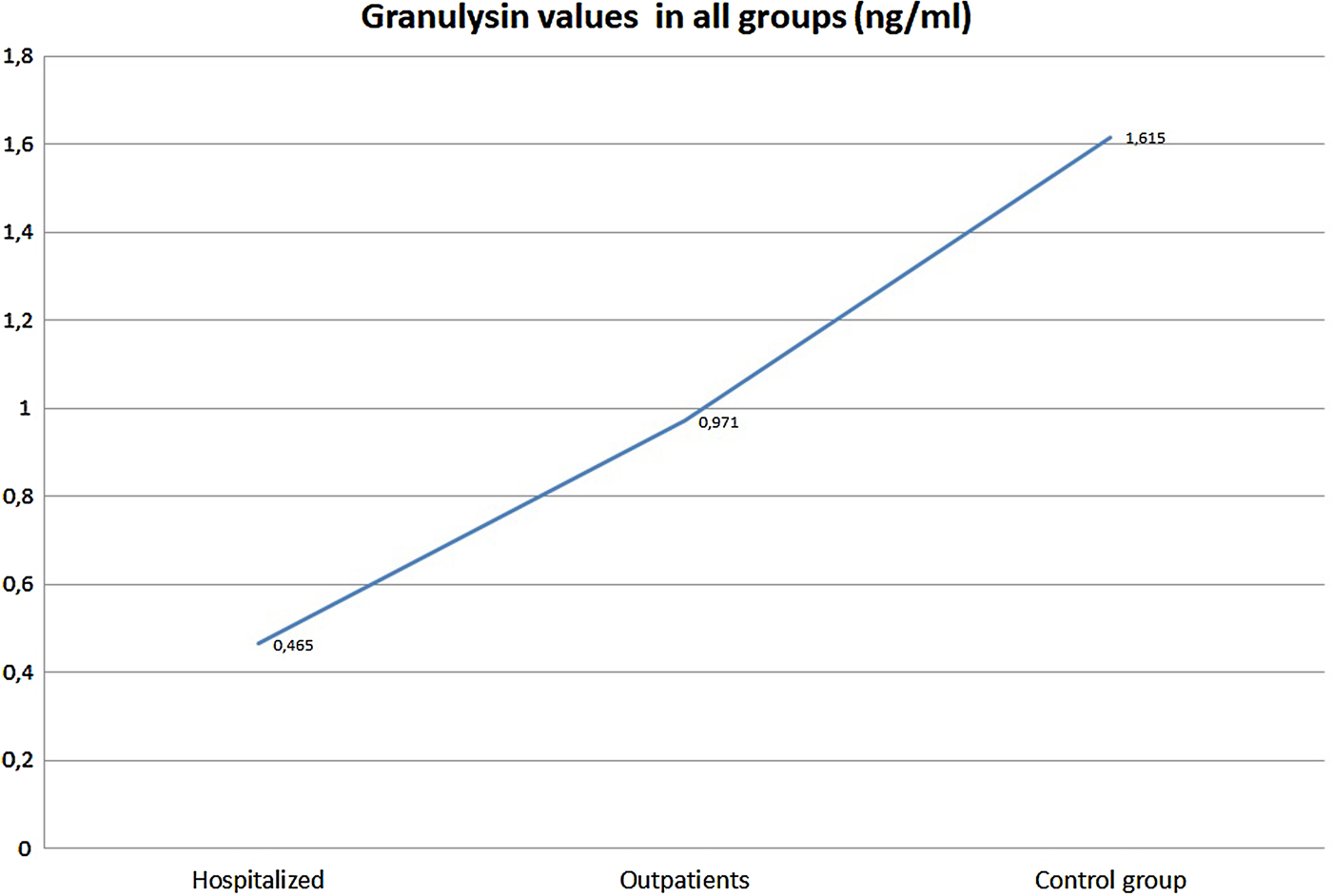
Fig. 1. Levels of granulysin by patients group.
In a group of patients with moderate, severe and life-threatening presentation, median value of granulysin was 0.95 (range 0.00–1.67 ng/ml; s.d. = 0.52). The median value for a control group was 1.69 ng/ml (range 0.40–6.70 ng/ml, s.d. = 1.56).
Pearson's χ 2 test found no statistical difference in the levels of serum granulysin for sex between the groups, but difference was found for age (P = 0002).
We used multivariate logistic regression analysis to test the impact of serum granulysin to a clinical presentation of chickenpox. Patients with lower levels of granulysin had more severe clinical presentations (R 2 = 0.21; P = 0.04). The Pearson's correlation analysis found a negative correlation between number of complications and level of serum granulysin (R 2 = 0.29; P = 0016).
Discussion
Granulysin has been detected in cytolytic granules of CTL and NK cells aside with pore-forming proteins: perforin and granzymes [Reference Chávez-Galán7]. The importance of serum granulysin level in the immunopathogenesis of chickenpox was described in an experimental study led by Hata et al. [Reference Hata8]. In this study, granulysin was extracted from Escherichia coli, and added to a fibroblast culture infected with VZV. Granulysin enters infected cells, causing ionic misbalance, which leads to apoptosis and further stops viral replication. Higher concentration of granulysin dramatically increases the rate of infected cell death. We found significant differences in serum granulysin levels between patients with mild clinical form of disease and others who had moderate, severe or life-threatening forms. A strong negative correlation between the levels of granulysin in serum and presented complication was also confirmed. Serum granulysin can be considered as a potent prognostic biomarker of gastric carcinoma. Saigusa et al.[Reference Saigusa9] found a direct correlation between serum granulysin levels and clinical course and outcome of the disease. Low granulysin level led to a severe clinical form of disease and poor outcome, and also, they noticed an increased number of liver and peritoneal metastasis in the same patients.
The role of granulysin as a possible biomarker in NK cells neoplasms connected with the Epstein–Barr virus was conducted by Nagasawa et al.[Reference Nagasawa10]. Granulysin was found as a strong prognostic marker of malignant proliferation of NK cells. In a recent study by Pitabut et al. [Reference Pitabut11], the importance of granulysin levels has been found in patients with tuberculosis (TBC), so as in patients with TBC/HIV coinfection. Lower levels of granulysin have been found in patients with TBC, while very high levels were found in patients with TBC/HIV coinfection. This was the first study ever performed that investigated possible correlation of granulysin and TBC/HIV coinfection. In an experimental study, granulysin, together with granzyme and perforin, can cause death of intracellular parasites, like Toxoplasma gondii, Trypanosoma cruzi and Leishmania major[Reference Dotiwala12]. These findings can be a good input for further studies, since there is no relevant prognostic parameter of chickenpox in everyday clinical practice. We still do not know if NK cells and CD8 + lymphocytes are only cells that release granulysin, and the role of CD4 + lymphocytes in situations of acute VZV infections. These findings can also be helpful in other viral infections, especially in herpes viruses. Granulysin, as a therapeutic, also deserves to be a point of interests in the future. If we prove its potential to stop dissemination of human herpes viruses, possibilities to use it in some life-threatening forms of viral disease can be very valuable. Not only for VZV, as we can suppose on the basis of this study, but more importantly in cytomegalovirus infections in transplant patients or fulminant forms of herpes encephalitis.
Supplementary Material
The supplementary material for this article can be found at https://doi.org/10.1017/S0950268818000717
Acknowledgements
The authors would like to thank personnel of the Clinic for Infectious Diseases and the Department for Clinical Immunology, Clinical Center University of Sarajevo, for a great support in this work.
Declaration of interest
None.



