



With the likely emergence of new variants and the long tail of health and economic impacts, the coronavirus disease 2019 (COVID-19) pandemic continues to prompt a broad set of responses from entities across civil society. And in the United States, responses like business closures and mask and vaccine mandates garnered significant public backlash that arguably hindered their effectiveness. 1–Reference Bonnevie, Gallegos-Jeffrey and Goldbarg8 If ongoing contention with COVID-19 and future pandemics is now a collective reality, it is important to understand how attitudes during COVID-19 could play out in future pandemics and how these views may influence pandemic preparedness activities. Attitudes related to specific pandemic experiences may require distinct intervention strategies. Furthermore, understanding COVID-19 attitudes may influence how the US designs systems and structures to respond more effectively to future shocks.
This article focuses on that next pandemic, exploring people’s attitudes in relation to 3 areas: personal COVID-19-related impacts, attitudes about institutions, and views of social change that could either pose challenges or help policy-makers leverage those attitudes to augment preparedness activities.
While a pandemic affects a broad swath of society, individual experiences during the COVID-19 pandemic varied. Those who were personally affected by the virus—being diagnosed themselves, caring for loved ones who were diagnosed, or experiencing other mental health, economic, and social impacts—represent an important stakeholder group for decision-makers to consider as they prepare for the next pandemic, as these groups are likely to continue to bear the brunt of negative impacts. Moreover, these effects were particularly pronounced in historically marginalized and underinvested communities, such as for Black, Hispanic, and low-income Americans. Reference Berkowitz, Cené and Chatterjee9
Understanding attitudes about institutions is key for future planning. COVID-19 appeared amidst a 30-y decline in trust in government institutions among the general public, Reference Lee and Schachter10 and in an environment of increasing political polarization. Reference Gollust, Nagler and Fowler11 Previous research has shown that trust in scientific experts, government officials, and other authority figures is correlated with health risk perceptions and mitigation measures, including vaccine uptake. Reference Jamison, Quinn and Freimuth12–Reference Miyachi, Takita and Senoo14 While federal agencies played a significant role in pandemic response, specific responses were carried out by different types of institutions, including state and local governments, and private and nonprofit organizations. Reference DeSalvo, Hughes and Bassett15 Although there is a small body of work on diverging levels of trust in state vs federal government in various policy domains, little research has explored differences in attitudes about pandemic response by type of institutions, including federal, state, and private institutions. Reference Leland, Chattopadhyay and Maestas16
Finally, there are attitudes that emerge from crisis and can influence more widespread policy changes. To be sure, evidence to date is mixed on the role of personal experiences with disaster on support for policy change: In general, people struggle to connect policy to their own lives, Reference Bishop17 and there is a pervasive lack of empowerment among individuals and communities to make decisions that reduce the risk and impact of disasters. Reference Cutter, Ahearn and Amadei18 In the context of COVID-19, partisan messaging has played a large role in the public response to the pandemic and mitigation measures, one that may have superseded personal experience. Reference Gadarian, Goodman and Pepinsky19 However, the pandemic has also brought about many changes to long-advocated-for health care and social policies. Reference Shah, Shankar and Schwind20 Therefore, planners expect COVID-19 to present an opportunity for positive change, but it is important to understand how public sentiment has shifted to support those changes, Reference Carman, Chandra and Miller21 and what role various personal experiences with COVID-19 might have played in those shifts.
Research Questions
Given this context, this study focused on 3 areas:
-
What were COVID-19-related experiences and how common were they for different groups over the course of the pandemic?
-
How did different COVID-19-related experiences relate to attitudes about institutions’ ability to respond to COVID-19 over the course of the pandemic? How did attitudes differ by type of institution?
-
How did different COVID-19-related experiences relate to perceptions of positive social changes as a result of the pandemic? What types of changes were prioritized related to COVID-19-related experiences?
Findings from this research can help inform preparation for the next pandemic, including repairing attitudes about institutions for those who were most impacted and targeting areas for policy change based on converging public sentiment.
Methods
Survey
Sample
To explore Americans’ attitudes and COVID-19-related experiences, this study analyzed data from 3 waves of the longitudinal COVID-19 and the Experiences of Populations at Greater Risk Survey (CEPGRS), a survey that RWJF and the RAND Corporation fielded 4 times during 2020 and 2021. Reference Carman, Chandra and Bugliari22 The CEPGRS builds on the National Survey of Health Attitudes (NSHA), which has been fielded in 2015 and 2018 and captures information on how people in the United States think about, value, and prioritize issues of health, well-being, and equity. Reference Carman, Chandra and Weilant23
Identical CEPGRS instruments were fielded to 2 online panels, the RAND American Life Panel (ALP) and the KnowledgePanel (KP). Both are nationally representative Internet panels recruited by means of probability-based sampling methods and collect demographic information on respondents separately from individual survey administration. Both provide computers and Internet connections for respondents who do not already have them and offer a modest incentive for participation.
In both panels, this study oversampled respondents who are Black, Hispanic, or Asian. The KP sample was limited to individuals in households with incomes under $125,000. The ALP sample limited white individuals to those with household incomes under $125,000 but imposed no income limits on Black, Hispanic, or Asian respondents. The income limits allowed the team to focus on individuals in households that were likely eligible to receive the federal COVID-19 stimulus checks. The survey was fielded 3 times: June 29 to July 22, 2020 (wave 1: Summer 2020); October 9 to November 2, 2020 (wave 2: Fall 2020); and February 22 to March 22, 2021 (wave 3: Winter 2021). A fourth wave was conducted September 7 to October 4, 2021, but those data were not analyzed for this study. All respondents to the first wave were invited to participate in subsequent waves. More characteristics of the sample are described in Carman et al. 2021. Reference Carman, Chandra and Bugliari22
Instrument and measures
Where possible, CEPRGS questions were sourced from existing surveys. Because this survey assessed attitudes about evolving issues, many new questions were developed. Survey content was developed and reviewed by a group of researchers representing a variety of disciplines conducting surveys about COVID-19 to establish reasonable face and content validity. Reference Carman, Chandra and Bugliari22
COVID-19-related experiences. Measures of COVID-19-related experiences were based on survey questions in all 3 waves about the impact of COVID-19 on respondents’ lives (“Are you experiencing or have you experienced any of the following as a result of the coronavirus [COVID-19] pandemic or the response to the pandemic?”): COVID-19 diagnosis (1) self, (2) loved one, (3) both); (4) feeling isolated or lonely; (5) death or loss of a loved one; (6) increased use of alcohol/drugs; (7) problems affording food; (8) unable to pay rent or mortgage; (9) unable to afford bills; (10) disruption in chil-dcare/school (in wave 1, this was 2 separate questions assessing child-care challenges and disruption in school or education for self or someone in your household); (11) difficulty caring for a chronic condition. COVID-19 experiences were grouped for analysis into 5 categories: COVID-19 diagnosis (self or loved one); emotional distress; financial hardship; child-/health-care challenge; and a combined COVID-19 experiences group (respondents answering “yes” to at least 1 COVID-19 impact question.).
Attitudes about institutions’ ability to respond to the pandemic. Measures of attitudes about institutions’ ability to equitably respond (here forward “attitudes about institutions”) were based on responses to survey questions in all 3 waves about (1) trust that state government (eg, governor or state legislature) is doing enough in dealing with the impact of COVID-19 to look out for the interests of all people, regardless of a person’s race, how much money someone makes, where people live, or other factors, (2) analogous question about the federal government, (3) perceptions that businesses know more about how to protect their own employees and customers from COVID-19 than government officials. Response scales differed between these questions, with state and federal government questions assessing trust on a labeled scale of 1 to 4, where higher ratings indicate greater trust, and the business question assessing agreement on a 5-point labeled Likert scale, where lower ratings indicate more agreement. For analogous analyses, the scale of the business question was reversed and all 3 measures were dichotomized to compare perceptions of positive attitudes about institutions’ ability to respond to the pandemic. The final measures were “a great deal” or “a fair amount” vs “none” or “a little” trust that governments are doing enough and “strongly agree” or “somewhat agree” vs “neither agree nor disagree,” “somewhat disagree” or “strongly disagree” that businesses know how to protect employees and customers from COVID-19.
Perceptions about positive changes from the pandemic. Measures of perceptions of positive changes were based on 2 survey questions in waves 2 and 3. One question assessed perceptions of whether COVID-19 presented an opportunity for positive changes in society. Responses were on a 5-point labeled Likert scale, where lower ratings indicate more agreement. In wave 2, respondents who agreed with that question were presented a second question asking them to choose the “most important” societal change they would like to see from a list of options that included “reduce income inequality,” “improve access to health care,” “prioritize science in policy decisions,” “protect our freedom,” and “reduce the role of government,” among other options. In wave 3, all respondents were asked to choose the most important positive change.
Analysis
This analysis focused on how attitudes about institutions and perceptions of positive changes that could result from the pandemic changed over time for analytic groups defined by experiences of various health, social, and economic impacts related to COVID-19 (“COVID-19-related experiences”). This study first examined the sample incidence of various COVID-19-related experiences and the demographic profile of each analytic group by computing frequencies and percentages across waves. Next, logistic regression models were used to detect differences in attitudes about institutions and perceptions of positive change between the analytic groups at each wave while controlling for differences in race/ethnicity, education, and household income level. Odds ratios were calculated with 95% confidence intervals. Analyses were performed using Stata 17.0.
Institutional review board approval
Data collection was approved by RAND’s Human Subjects Protection Committee, which acts as RAND’s Internal Review Board. RAND’s “Federalwide Assurance for the Protection of Human Subjects” (FWA00003425, effective through June 22, 2023) serves as our assurance of compliance with the regulations of 16 federal departments and agencies. ALP and KP participants receive consent materials once per year consenting to participate in surveys and are given the right to skip any survey or question.
Results
Survey participation generally decreased across survey waves, and attrition was distributed evenly across demographic groups. Across waves, roughly half of respondents were non-Hispanic white, roughly one-quarter of respondents were Hispanic, and roughly 18% were Black, with other racial/ethnic groups representing less than 10% of the sample. Other demographic characteristics are shown in Table 1.
Table 1. Demographics of survey respondents by survey wave
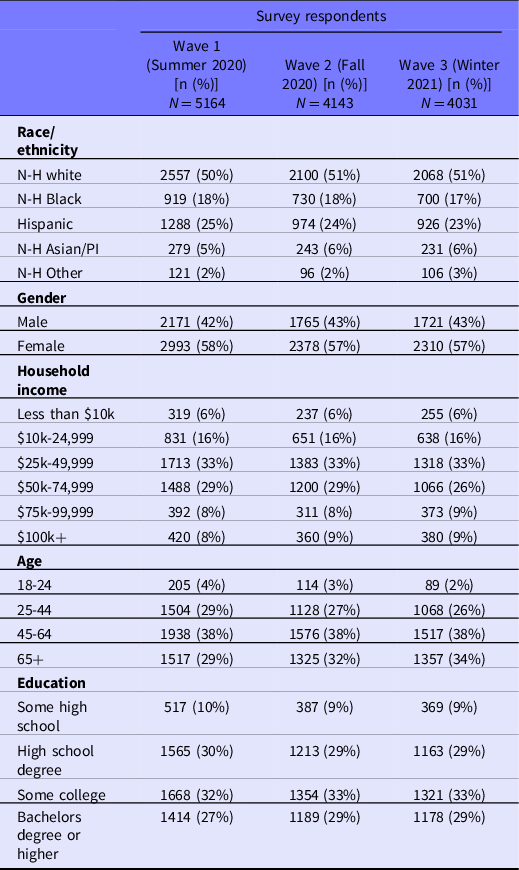
Abbreviation: N-H, Non-Hispanic; PI, Pacific Islander.
COVID-19-Related Experiences
The proportion of respondents indicating they had personally experienced at least 1 health or other impact from COVID-19 increased over time: 43% of the sample had COVID-19-related experiences in Summer 2020, 64% in Fall 2020, and 70% in Winter 2021 (Figure 1). The percent of respondents (or a loved one) diagnosed with COVID-19 also increased from roughly 9% in Summer 2020 to roughly 28% in Winter 2021.
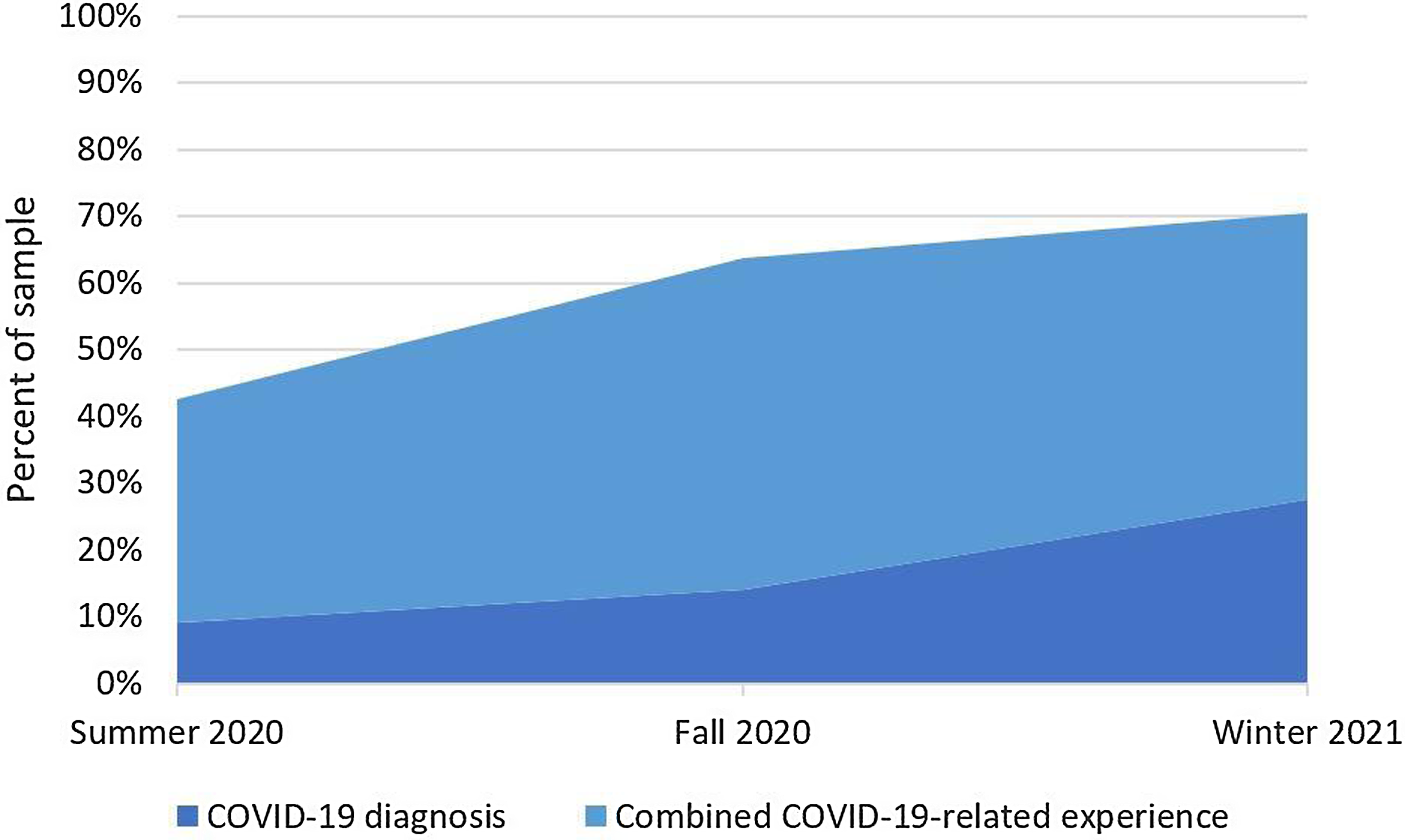
Figure 1. COVID-19 experiences over time.
The most reported COVID-19 experience at any time point was child-/health-care-related difficulties in Summer 2020. Prevalence of COVID-19 experiences differed by demographic group and changed slightly across waves (Figure 2). In Summer 2020, white respondents had the lowest proportion of combined COVID-19 impact reports compared with other racial/ethnic groups (eg, 39% of white respondents compared with 49.7% of Hispanic respondents). Over time, gaps between white respondents and other racial/ethnic groups shrank or were reversed. However, proportions of Hispanic respondents reporting any COVID-19-related experiences remained the highest of any group, at 75.6% in Winter 2021, with Hispanic respondents particularly overrepresented in the group experiencing financial hardship and health-/child-care difficulties. Across waves, reports of COVID-19-related experiences did not vary much by education level of respondents, other than financial hardship, which was disproportionately reported among those with the lowest education levels. (Data on all COVID-19-related experiences by demographics across survey waves are available in a Supplement.)
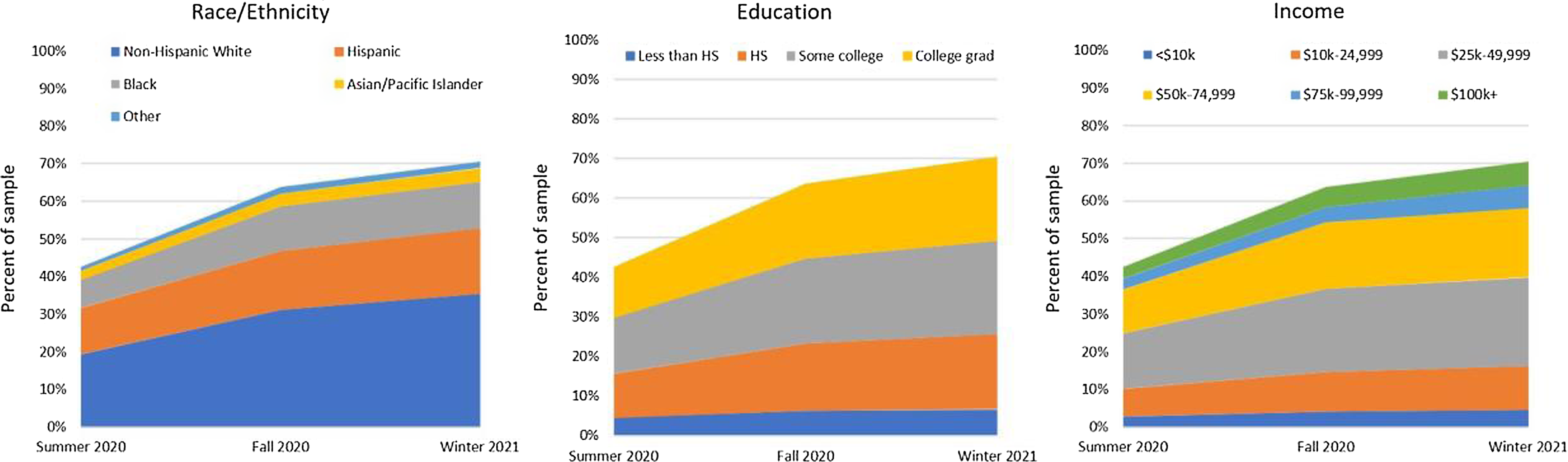
Figure 2. COVID-19 experiences by demographic.
Attitudes about institutions
Attitudes about institutions’ ability to respond to COVID-19 differed by COVID-19-related experiences and over time. In general, experiencing any COVID-19-related impact was associated with a lower likelihood of reporting positive attitudes about institutions’ ability to respond (Table 2). Early in the pandemic (Summer 2020), experiencing COVID-19-related impacts was associated with lower likelihood of reporting positive attitudes about governments (state and federal). Later in the pandemic (Winter 2021), likelihood of reporting positive attitudes about governments remained low, particularly for those experiencing financial hardship and child-/health-care difficulties. For example, those experiencing financial hardship in Winter 2021 were the analytic group least likely to report positive attitudes about state governments’ ability to respond (odds ratio [OR] = 0.55; 95% confidence interval [CI]: 0.47-0.64). Differences in attitudes about businesses’ ability to respond to the pandemic were generally non-significant, except in Winter 2021, when those reporting any COVID-19-related experience, particularly emotional distress (OR = 0.80; 95% CI: 0.71-0.91) or child-/health-care difficulties (OR = 0.84; 95% CI: 0.71-0.99), were significantly less likely to report positive attitudes about businesses. (Data on attitudes about institutions across survey waves is available in a Supplement.)
Table 2. Attitudes about institutions’ ability to respond to the pandemic by COVID-19-related experience in Winter 2021
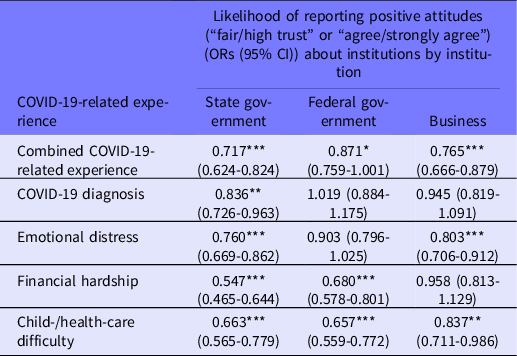
***P < 0.01, **P < 0.05, *P < 0.1
Note: Logistic regression models controlled for differences in race/ethnicity, education, and household income level.
Abbreviations: CI, confidence interval; COVID-19, coronavirus disease 2019; OR, odds ratio.
Perceptions about positive changes from the pandemic
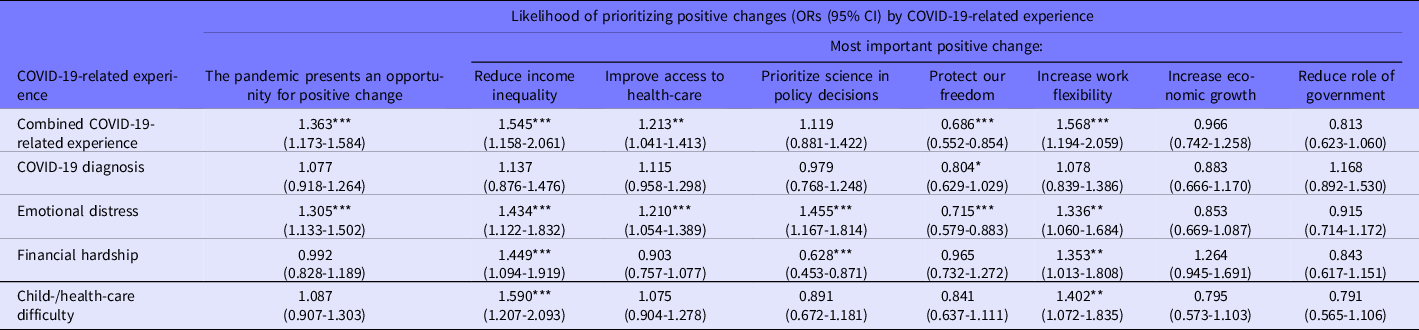
Respondents generally perceived that COVID-19 presented an opportunity for positive change in society. Respondents in the COVID-19-related experiences group were more likely to agree there is opportunity for positive change compared with respondents who did not have COVID-19-related experiences, though adjusted regression models with demographic characteristics as predictors showed that the perception that the pandemic presented an opportunity for positive change differed by type of COVID-19-related experience (Table 3). For example, those who reported emotional distress (OR = 1.31; 95% CI: 1.13-1.50) or who were part of the combined “COVID-19-related experience” group (OR = 1.36; 95% CI: 1.17-1.58) were significantly more likely to perceive that the pandemic presents an opportunity for positive change. Differences in perceptions of positive change were not significant for those respondents reporting any other specific COVID-19-related experiences.
Table 3. Perceptions of positive changes by COVID-19-related experience in Winter 2021
***P < 0.01, **P < 0.05, *P < 0.1
Note: Logistic regression models controlled for differences in race/ethnicity, education, and household income level.
Abbreviations: CI, confidence interval; COVID-19, coronavirus disease 2019; OR, odds ratio.
The most commonly selected prioritized positive change across the sample was “improve access to health care.” “Reduce income inequality” was more likely to be selected as a prioritized positive change among those with COVID-19-related experiences, regardless of the specific experience, and there were differences in likelihood of prioritizing different positive changes by COVID-19-related experiences (Table 3). In particular, those reporting child-/health-care difficulties in Winter 2021 were significantly more likely to select “reducing income inequality” (OR = 1.59; 95% CI: 1.21-2.09) as the most important positive change coming out of the pandemic than those not experiencing child-/health-care difficulties. (Those experiencing emotional distress and financial hardship were also more likely to prioritize “reducing income inequality,” although the magnitude of the association was slightly lower [OR = 1.43; 95% CI: 1.12-1.83 and OR = 1.45; 95% CI: 1.09-1.92, respectively].) On the other hand, those reporting experiencing financial hardship in Winter 2021 were significantly less likely to select “prioritize science in policy decisions” (OR = 0.63; 95% CI: 0.45-0.87) as the most important positive change coming out of the pandemic than those not experiencing financial hardship. Those with COVID-19-related experiences were also less likely to prioritize “protect our freedom,” particularly those who reported experiencing emotional distress (OR = 0.69; 95% CI: 0.55-0.85).
Discussion
This study describes views associated with COVID-19-related experiences and the implications of these perceptions for future pandemic preparation. We sought to understand differences in (1) attitudes about different institutions’ ability to respond to COVID-19 and (2) perceptions of positive societal changes stemming from the pandemic related to different COVID-19-related experiences. The CEPGRS is a longitudinal study, enabling researchers to examine how changes in COVID-19-related experiences and attitudes toward institutions and prioritized positive changes evolved over the course of the first year of the pandemic, between June 2020 and March 2021. Even as the COVID-19 pandemic continues to impact daily life for many Americans, planning now for future pandemics, as experiences are evolving and attitudes are continually being shaped, could prove beneficial.
This analysis reveals insights for pandemic planners going forward, particularly in our primary areas of interest related to personal COVID-19-related experiences, attitudes about institutions, and expectations for social change. Examining how these 3 domains were related provides a path forward for public messaging and future engagement of the American public in pandemic preparedness.
COVID-19-related experiences appear to be related to attitudes about institutions. Those who experienced any COVID-19-related impacts were less likely to report positive attitudes about institutions’ ability to respond to the pandemic and were less likely to report trust in state governments in particular as the pandemic wore on. Given the visible role of state governments in imposing public health policies, such as mask mandates, and making decisions about school and business reopening, it may demonstrate the immediacy of blame that might exist for those with COVID-19-related experiences. Depending on the community, private businesses were charged with COVID-19 mitigation and response with regulatory oversight and guidance from state governments varying by state. 24 Pandemic fatigue may be understandably more pronounced for those who were personally impacted, thus approaches to address that fatigue must consider how people view institutions and the faith they may place in communication and expectations coming from those institutions. For instance, local governments and businesses may need to evolve their messaging to account for the growing impact of a pandemic and have specific narratives ready to meet each stage of an evolving but chronic situation.
On the other side, those with COVID-19-related experiences also may be a ready group of ambassadors for leveraging the terrible experience into positive social change. Our findings show that those with personal experiences saw this as an opportunity for changes, such as reducing income inequality. Other recent data have shown that over 60% of Americans agree that the country faces an income inequality problem, but fewer than half say addressing it is a top priority. Reference Horowitz, Igielnik and Kochhar25 This suggests there is a window of opportunity to reform the system, but that more is needed to motivate prioritization nationwide. Those invested in improving public health emergency preparedness, including addressing the social drivers of health, could capitalize on that interest among those with COVID-19-related experiences, training members of this group to be champions and policy influencers going forward. At the same time, planners must be mindful of those without COVID-19-related experiences, who were more likely to select other priorities such as protecting freedoms. Additionally, certain COVID-19-related experiences such as experiencing financial hardship were associated with lower likelihood of prioritizing science in policy decisions. Our findings align with previous research on Americans’ reticence to support public policy that requires behavior changes and limitations on personal choices without a clear personal benefit, particularly in situations of scientific uncertainty, like an evolving pandemic. Reference Diepeveen, Ling and Suhrcke26,Reference Kreps and Kriner27 Messaging about emergency preparedness and pandemic preparations for that group will need to include an approach that does not appear to impose on individual behavior change, but rather considers how notions of freedom and evidence-based pandemic preparedness can be knitted together.
Limitations
Strengths of this study include its nationally representative sample, with a particular focus on those individuals earning less than $125,000 per year, a group that was expected to receive federal support and more likely had to make difficult choices during the pandemic. However, survey data and analytic methods present certain limitations that may constrain the generalizability of these results. First, survey respondents were members of existing online panels. Although the panels are demographically diverse, certain groups may be underrepresented. Response bias was mitigated by sending reminders to potential respondents. Second, the ways in which this study defined analytic groups and constructs could have constrained interpretations of differences in attitudes. Similar pandemic-related experiences were grouped for simplicity, but the effects of each experience (eg, feeling isolated or lonely vs experiencing death or loss of a loved one) were not analyzed separately. Third, because selection of the most important positive societal change as a response to the pandemic was only available to a subset of Fall 2020 respondents, the comparability of that measure between waves may be limited. Additionally, opinions about the presidential election in 2020 and transition in 2021 may have particularly impacted individuals’ trust in the federal government, beyond the role of their experience of COVID-19-related impacts at each time point. Detailed examination of the effects of the election was beyond the scope of this analysis. While regressions controlled for some demographic factors, this study also did not analyze attitudes based on characteristics shown in the literature to impact beliefs about health or trust in institutions, including information sources, Reference Gollust, Vogel and Rothman28 prevailing social norms, Reference Streefland, Chowdhury and Ramos-Jimenez29 political party, or partisanship, Reference Gadarian, Goodman and Pepinsky19 because our analytic framing was intentionally based on the shared experience of being impacted by COVID-19. (The role of partisanship could have been particularly relevant in influencing attitudes about state government responses to the pandemic. Reference Wichowsky and Condon30 ) Attitudes about institutions including institutional trust was also defined slightly differently than in prior research to focus specifically on trust related to equitable COVID-19 response vs general trust in institutions. Thus, our results may not be directly comparable to existing evidence about trust in institutions, broadly.
Conclusions
Central to preparing for any future pandemic is learning the appropriate lessons from the past—in this case, the COVID-19 pandemic. As Kaiser Family Foundation’s chief executive, Drew Altman, put it: “When a theoretical threat becomes a clear and present danger, people are more likely to act to protect themselves and their loved ones.” Reference Hoffman31 Beyond changing their own behaviors, people’s pandemic experiences also influence their views on and support for institutional pandemic responses. In our sample, the composition of this group did not appear to change much over time, but attitudes did change. These variations in views suggest several implications for policy-makers planning for future pandemic response.
First, lack of information at the outset of the COVID-19 pandemic hampered responses that could have blunted disease spread and its impact on vulnerable populations. There is a need for increased foresight and capacity that can support anticipation of potential backlash or other public views that could affect the effectiveness of pandemic responses (eg, mask mandates). Future pandemic response would benefit from improved anticipation capabilities, both by investing in public health surveillance monitoring and by better understanding how public views may affect planned actions. Reference Parker, Edelman and Carman32 The urgency to anticipate public views on pandemic response is underscored by the fact that there is possibly a brief window of opportunity, as prior research has shown that public support for policy change tends to flag quickly after a disrupting event. Reference Bishop17
Second, strengthening public institutions will be crucial to ensuring their effectiveness during a pandemic. Bolstering capacities of public institutions also helps build trust in them. Improving logistics and governance (including the role of federal, state, local governments, and communities) not only helps disaster response operations, but can be employed in service of trust-building and public confidence.
Finally, pandemic planning could exploit opportunities to take policy actions where views seem to converge among people with otherwise-divergent views. In our results, the most widely agreed upon item for future change was support for increased access to health care (regardless of COVID-19 experiences), with prioritization of reducing income inequality concentrated among those with COVID-19-related experiences. This suggests that people might support steps that improve general societal equity, in addition to steps that focus on pandemic response (eg, disease surveillance). It also emphasizes the enduring importance of addressing fundamental health concerns and drivers, such as and increasing access to health care and reducing inequality.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2023.38.
Acknowledgments
The authors thank Carolyn Miller for reviewing this study and providing valuable feedback. The manuscript was written by the RAND study team.
Funding
This research was funded by the Robert Wood Johnson Foundation (award no. 74430). The funding body offered input on the study design and interpretation of data, but ultimately the RAND study team had final determination of all research design, analysis, and interpretation choices.







 Open access
Open access