



LEARNING OBJECTIVES
After reading this article you will be able to:
• understand the history and development of multiaxial classification systems in the context of child and adolescent psychiatry
• use the ICD-10 multiaxial classification system for child and adolescent psychiatry to assist in a biopsychosocial approach to children and adolescents with mental health problems
• understand the extended use of the ICD-10 multiaxial classification system for hypothesising about differential diagnosis, planning psychotherapeutic interventions, teaching and training, analysing complex cases, and using a chronological perspective to look at symptoms and medication response.
Mental disorders are frequently complicated and often involve several potentially important factors which ‘do not in any meaningful sense, constitute alternatives’ (Taylor Reference Taylor, Rutter, Rutter, Bishop and Pine2008: p. 21). For instance, someone may have depression but also have an intellectual disability. To address the frequent issue in psychiatry of having several clinically important separate factors salient in diagnosis a variety of ‘multiaxial’ systems have been proposed over the years. These multiaxial systems have in common the distribution or clustering of suggested relevant factors into different axes to help in the overall understanding of the individual.
Although the interest in multiaxial classification stretches at least into the 1940s (Essen-Moller Reference Essen-Moller and Wohlfahrt1947), it was the World Health Organization (WHO) that bought it into prominence for child psychiatry in the 1960s, largely through the efforts of Michael Rutter and others. A paper reporting on the third WHO seminar on psychiatric disorders held in Paris in 1967 was published in 1969 regarding psychiatric disorders in childhood, with an aim ‘to make an early beginning on the task of developing a useful and scientifically sound system of classification in child psychiatry [ … ] acceptable for international application’ (Rutter Reference Rutter, Lebovici and Eisenberg1969). The diagnostic exercises carried out in the 1960s involved case histories and diagnostic video recordings. The question as to different axes of classification arose and was illustrated by the case of an 11-year-old child ‘who had an epileptic fit, whose general level of functioning was in the mentally subnormal range, and who showed a very severe disorder of behaviour, emotions and relationships. Some participants diagnosed psychosis [autism], others diagnosed mental subnormality [intellectual disability], and yet others chronic brain condition. It was generally recognised that all three diagnoses were probably correct but that each diagnosis concerned a separate and independent axis of classification’. This led to a proposed triaxial classification scheme (Supplementary Table S1, available at https://doi.org/10.1192/bja.2023.39) (Rutter Reference Rutter, Lebovici and Eisenberg1969).
Later it was suggested that the third axis, of associated or aetiological factors, be divided into two, one covering physical conditions and the other psychosocial conditions (Rutter Reference Rutter, Shaffer and Shephard1975). In 1975, in the UK, a fifth axis for specific developmental disorders was added – these disorders had previously been included with the ‘biological factors’ in the third axis (Rutter Reference Rutter, Shaffer and Shephard1975; World Health Organization 1996). Modification of Axis Five was later made to improve its reliability (van Goor-Lambo Reference van Goor-Lambo1987, Reference van Goor-Lambo, Orley and Poustka1990).
After the introduction of ICD-10 in 1993, it was suggested by Rutter that a sixth axis, ‘global assessment of psychosocial disability’, be introduced to assess disability. This was because disability was recognised by the WHO as a vital component of the assessment of psychiatric disorder (Reed Reference Reed, Spaulding and Bufka2009): ‘Its inclusion should be regarded as a first step towards the development of a systematic scheme for assessing social disability in children and adolescents with psychiatric disorder’ (WHO 1996: p. 2). Axis Six attempts to capture the individual's level of functioning, with the various aspects of functioning captured in a single global score, ranging from superior/good social functioning (scored 0) to profound and pervasive social disability (scored 8). It is the only axis that does not include codes found in ICD-10.
Axes One to Five are populated with the codes present in ICD-10, with axes One to Three drawn from the ‘F’ codes (Chapter V of ICD-10, ‘Mental and behavioural disorders’ F00–F99; WHO 2016). By previous convention, ‘Autism’ (F84) has been assigned to Axis One rather than Axis Two. Axis Four includes ‘Medical conditions from ICD-10 often associated with mental and behavioural disorders’, and Axis Five uses selected ICD-10 ‘Z’ codes (Chapter XXI, ‘Factors influencing health status and contact with health services’, Z00–Z99; WHO 2016), which are placed within ‘Associated abnormal psychosocial situations’. Expanded definitions are available for the Z codes and an atheoretical approach to timing was taken, with lifetime coding suggested but ‘with the recognition that users of the scheme will need to decide for themselves the timeframe that best suits their purposes’ (WHO 1996: p. 8).
Table 1 shows the six axes, together with the coding covered within each one. The latest iteration of ICD, ICD-11, remains as previous versions, uniaxial, but there is no reason why the multiaxial framework cannot be utilised with coding from ICD-11, even if a similar publication to that which accompanied ICD-10 is not published by the WHO (Rutter Reference Rutter, Pine, Thapar, Pine and Leckman2015).
TABLE 1 Multiaxial classification system for ICD-10

Source: adapted from World Health Organization (1996).
Other multiaxial schemes
ICD-10 has remained a uniaxial system and allows, if you like, a parallel multiaxial system to exist for child and adolescent psychiatry, which is especially helpful in complex presentations.
A multiaxial system for adult psychiatry was published by the WHO in 1997 (Janca Reference Janca1997). This system had only three axes, with all ICD-10 codes (excluding Z codes) clustered somewhat unsatisfactorily in Axis I, and Axis II attempting to capture ‘Disability’, with Axis III capturing ‘Contextual factors’ using the Z codes.
In 1980 the American Psychiatric Association published DSM-III, which differed from its predecessor by its multiaxial approach (Williams Reference Williams1985). Although there were aspects that were, to contemporaries, unsatisfactory, these very critics acknowledged it as ‘a landmark in the development of psychiatric classification’ and that ‘the introduction of a multiaxial framework is a step forward in terms of its recognition that clinical diagnosis necessarily involves several different elements which do not constitute alternatives to one another’ (Rutter Reference Rutter and Shaffer1980). The multiaxial organisation continued through DSM-III-R (Revised) and DSM-IV-TR (Text Revision) but was abandoned in DSM-5.
This difference in approach was reported by DSM-5 to be an inability to find ‘fundamental differences’ between Axes I to III, lack of ‘frequent’ usage of Axis IV categories and ‘lack of clarity’ in the usage of Axis V (American Psychiatric Association 2013: pp. 16–17). This abandonment of the multiaxial system does not seem to capture the history of the debate concerning its inclusion/exclusion in DSM-5 (Probst Reference Probst2014) and although there were deficiencies to be addressed, especially in regard to Axis IV (Kress Reference Kress, Barrio Minton and Adamson2014), it is not clear that exclusion of the multiaxial system actually led to a classification system with better clinical utility. However, the recent and substantial harmonisation of coding in the newly released DSM-5-TR (American Psychiatric Association 2022) with ICD-10 provides an opportunity for the use of the DSM with the ICD-10 multiaxial system.
The Diagnostic Classification (DC) of Mental Health and Developmental Disorders of Infancy and Early Childhood in its various iterations – DC:0–3, DC:0–3R (Revised) and DC:0–5 (Zero to Three 2016) – has also favoured a multiaxial system but with axes to cover ‘Relational context’ (Axis II) and ‘Developmental competence’ (Axis V), along with axes familiar from the ICD, including ‘Clinical disorder’ (Axis I), ‘Physical health’ (Axis III) and ‘Psychosocial stressors’ (Axis IV).
The rationale for multiaxial classification in child and adolescent psychiatry
Before exploring the practical ways in which the ICD-10 multiaxial system can assist in clinical practice it is first important to look at the reasons and rationale behind the development of such a framework. As shown above, one driver for the development of multiaxial classification was the problem of being forced to choose between non-exclusive diagnostic alternatives. A multiaxial system helps to avoid this situation as well as providing a much more holistic understanding of the child within their environment, taking into consideration medical conditions, past environmental events and stressors. The multiaxial system, by taking an atheoretical view of causation and allowing a straightforward presentation of possibly important factors, can be utilised by clinicians with differing theoretical frameworks. For instance, one is not forced into deciding whether in a particular case autism or parental separation might be the reason for some challenging behaviours – both might be contributary. Possible aetiological factors can be listed and further elucidated to reach a more thorough formulation. It is also ‘much closer to most clinicians’ preferred style of conceptualisation than is the case with a system that forces everything into the Procrustean bed of a diagnosis based only on symptoms’ (Taylor Reference Taylor, Rutter, Rutter, Bishop and Pine2008: p. 21).
Over time, the evidence for the necessity of the biopsychosocial model in child and adolescent psychiatry that is encapsulated with the multiaxial approach has been fundamentally strengthened by the acceptance that mental disorders must often be viewed differently from physical disorders. Unlike many physical illnesses, for example infectious diseases, frequently in mental illness no single aetiological agent can be identified. Even where aetiological factors have been identified in mental illness, they do not act in a straightforward way, many of the ‘causal factors’ appearing to be transdiagnostic even if the underlying mechanisms are unclear (McLaughlin Reference McLaughlin, Colich and Rodman2020). The realisation that psychopathology ‘generally arises from multiple biological, behavioural, psychosocial and cultural factors, all interacting through an individual's lifetime of experience’ and that ‘mental disorders are not distinct conditions that someone “has”; rather they are complex, multidimensional phenomena with multiple causal strands’ (Clark Reference Clark, Cuthbert and Lewis-Fernández2017) is another reason for embracing a multiaxial system. That is because the use of such a system allows the capture of multiple factors beyond just a symptom cluster and categorical diagnosis. It allows a far richer understanding of the clinical presentation (Mayall Reference Mayall, McDermott and Sadhu2021) while hopefully suggesting interventions (as discussed below) that are not just targeted at a single categorical diagnosis.
Classic ICD-10 multiaxial classification and classic ICD-10 classification plus additional clinically useful information
There are several very useful ways in which the ICD-10 multiaxial classification system (WHO 1996) can be used. First, if used as intended by the WHO, it can clearly communicate the central clinical entity, along with any other factors considered helpful in understanding the case. Table 2 shows its use for a young person with a diagnosed moderate depressive episode, corresponding to ICD-10 code F32.1 (i.e. their symptoms on examination meet the ICD-10 diagnostic criteria).
TABLE 2 Classic use of the ICD-10 multiaxial classification system: young person with a moderate depressive episode with no self-harming

a Axes One–Six (World Health Organization 1996).
Additionally, if thought helpful a coding could be made as to whether a somatic syndrome is present or absent (F32.10, without somatic syndrome, or F32.11, with somatic syndrome). Thus, for the young person in Table 2, it can easily be seen that no abnormality is present in Axes Two and Three and no medical conditions (Axis Four) are thought to be relevant, and this is specifically spelled out but could also be coded with ‘XX’ (WHO 1996). That at some point a disruption of family has taken place is indicated by the appropriate Z code and a family history of some form of mental or behavioural disorders is also coded. An attempt has been made in Axis Six to identify the degree of psychosocial disability. The table as presented communicates and summarises clearly a relatively uncomplicated hypothetical case.
Table 3 shows the classic use of the multiaxial system in a hypothetical complex neurodevelopmental case in a 7-year-old boy. A range of mental and physical diagnoses are clearly identified, along with other possibly significant factors. Additional important information can be helpfully added.
TABLE 3 Classic use of the ICD-10 multiaxial classification system: complex neurodevelopmental case, male child 7 years old

Using the multiaxial framework in a variant manner to identify ages at which certain diagnoses were made can give clues as to the aetiology of certain symptoms; for instance, Table 4 shows a modified Table 3 with certain additional information that some clinicians might find extremely useful. In this case might there be a link between parental separation and the emergence of more recent challenging behaviours? The fact that only a single epileptic seizure has apparently occurred, and some time ago, possibly clarifies any possible connection between the seizures and the current escalation in behaviour; reassurance by clinical history and examination that this is accurate, and that seizure activity does not seem to be related to the more recent behavioural concerns, is important. Where there is doubt, it might lead to a review of any previous electroencephalogram (EEG) (after review of the notes it is ascertained that no EEG was carried out previously) or a request for an EEG if clinically indicated. Additionally, previous standardised testing and the results could be linked in the electronic notes to the various diagnoses. For example, the Wechsler Intelligence Scale for Children Fifth Edition (WISC-V) result showing the Full-Scale Intelligence Quotient (FSIQ) and subset scores might assist in planning school-based interventions. Again, slightly departing from the classic use of the multiaxial classification system, the result of adaptive behaviour testing, using for example the Adaptive Behaviour Assessment System Third Edition (ABAS-3), might be incorporated into Axis Three, supporting the confirmation of the diagnosis of mild intellectual disability and, if thought helpful, also in Axis Six along with the already coded ‘Global assessment of psychosocial disability’. Further information that might prove useful for understanding the case can be added (e.g. results on the Autism Diagnostic Observation Schedule Second Edition, ADOS-2). In a concise way, a much more comprehensive and useful summary has been produced by the additional information and the potential clinical utility enhanced.
TABLE 4 Extended use of the ICD-10 multiaxial classification system: complex neurodevelopmental case, male child 7 years olda

ADOS-2, Autism Diagnostic Observation Schedule Second Edition; OT, occupational therapist; WISC-V, Wechsler Intelligence Scale for Children Fifth Edition; FSIQ, Full-Scale Intelligence Quotient; ABAS-3, Adaptive Behaviour Assessment System Third Edition; EEG, electroencephalogram.
a Additional information is shown in bold and chronology is shown in italics.
b Axes One–Six (World Health Organization 1996).
Teaching, case review and hypothesising using the ICD-10 framework
The multiaxial classification framework can be useful in both training and teaching of junior doctors as well as child and adolescent mental health service (CAMHS) clinicians. It can also be useful in practical preparation for a clinical assessment to ensure thorough exploration of factors that are suggested from the information contained in the referral letter. Fig. 1 shows a letter from a hypothetical general practitioner (GP) Dr Goodletter.

FIG 1 A hypothetical GP's letter.
Using the multiaxial framework, the various bits of information can quickly and easily be placed in the appropriate axis. For illustration, Fig. 2 shows the various factors highlighted with colours, along with a colour-coded reference to the various axes. Of course, this colour coding is not necessary in normal clinical practice and once one is familiar with content of each of the individual axes can easily be done in moments.

FIG 2 The GP's letter with colour-coded symptoms using Axes 1–6 (One to Six) of the ICD-10 multiaxial classification system (World Health Organization (1996).
Fig. 3(a) shows for illustration a colour-coded multiaxial presentation of the information taken from the GP's letter. By the side of the multiaxial framework is the coding that can be summarised from the letter (assuming accuracy of the information provided). Here one can see that Axes Four and Five can be partially coded and, to the right of the first column in the box, several hypothesised diagnoses are suggested. Later in the assessment these hypothesised diagnoses can be confirmed or discarded. For completeness of the hypothetical case referred by Dr Goodletter an additional column has been added in Fig. 3(b) showing the confirmed diagnoses further to clinical/psychometric/adaptive behaviour assessment and collateral history from other sources.

FIG 3 Using the GP's letter: (a) from letter to ICD-10 coding and hypothesised diagnoses; (b) from letter to ICD-10 coding and confirmed diagnoses (post-assessment).
In this hypothetical case it was considered that the symptoms in Axis One were best understood as primarily the result of an adjustment to a variety of factors, including parental separation, recent diagnosis of diabetes and an unaddressed intellectual disability. By further clinical enquiry, the boy's apparent self-harm has been found to be episodes of scratching his arm with his nails. It can be appreciated how helpful this process might be in thinking systematically about a clinical case even when the information is initially incomplete. It also allows a trainee or other junior clinician to at least start the process of thinking of the differential diagnoses from the outset.
A process similar to that described above (Figs 1–3) can be usefully employed when one clinician approaches another with a more complicated case for which they are seeking advice and direction. Visualising the multiaxial framework together during case consultation using a whiteboard or electronic equivalent can be useful in this regard. The symptoms and factors relevant to the case can then be placed in the appropriate axes, along with previously confirmed diagnoses. Having laid out the multiaxial framework with the information already gleaned by the clinician, a series of hypothesised diagnoses can be placed to the right of the first two columns and, to the side of these, further information needed to clarify and substantiate these hypothesised diagnoses could be suggested. A blank template for such a framework is shown in Supplementary Table S2. This approach is also very helpful when teaching about differential diagnosis and also showing clearly how the multiaxial framework allows easy identification of any gaps in the knowledge about individual clinical cases.
Planning psychotherapeutic interventions using the ICD-10 framework
Table 5 shows a variant framework for a young adolescent who has presented for assessment in the CAMHS clinic. The framework this time allows clustering of confirmed and possible diagnoses, along with the proposed interventions, a timescale and who will be overseeing these interventions. The assessment has been carried out and a primary diagnosis of moderate depressive episode made. However, some areas are identified as requiring clarification. Possible interventions can be suggested for treatment of the primary diagnosis by the treating team, while other disciplines and organisations will be required, if possible, to create a more comprehensive understanding of this young person's problems. In this hypothetical case the adolescent is already being considered for the special needs (additional needs) unit of the school, although no formal testing has taken place. The school's special needs teacher has been identified as being able to carry out a standardised reading and spelling assessment, and the educational psychologist has arranged for psychometric and adaptive behaviour assessment to be undertaken. The WISC-V will be helpful not just in excluding any formal intellectual disability but also in identifying any subtests within the WISC that might indicate the presence of cognitive problems which could be interfering with school progress, such as very low processing speed index (PSI) or working memory index (WMI). Liaison with the paediatrician managing the diabetes, especially if medication is contemplated for the depressive symptoms, will be important. Information might be sought regarding adjustment to the diabetes diagnosis, along with how well the insulin administration is managed, insulin adherence and glycaemic stability. It is further suggested to the school, in the meantime, that additional support is obtained for the child in the special needs unit. Additionally, an assessment of the degree of psychosocial disability can be carried out on a regular basis, using the Global Assessment of Psychosocial Disability (WHO 1996) or other measures, such as the Child Global Assessment Scale (CGAS) (Shaffer Reference Shaffer, Gould and Brasic1983; Schorre Reference Schorre and Vandvik2004).
TABLE 5 Use of the ICD-10 multiaxial classification system to plan psychotherapeutic interventions: young adolescent

CBT, cognitive–behavioural therapy; ID, intellectual disability; WISC-V, Wechsler Intelligence Scale for Children Fifth Edition; ABAS-3, Adaptive Behaviour Assessment System Third Edition.
a Axes One–Six (World Health Organization 1996).
Chronology and the ICD-10 framework
In the discussion above regarding a complex neurodevelopmental presentation (Table 4) it was shown how chronology can be added to a multiaxial framework to potentially enhance the understanding of the case. Another way of presenting the chronological data in this case is shown in Fig. 4.
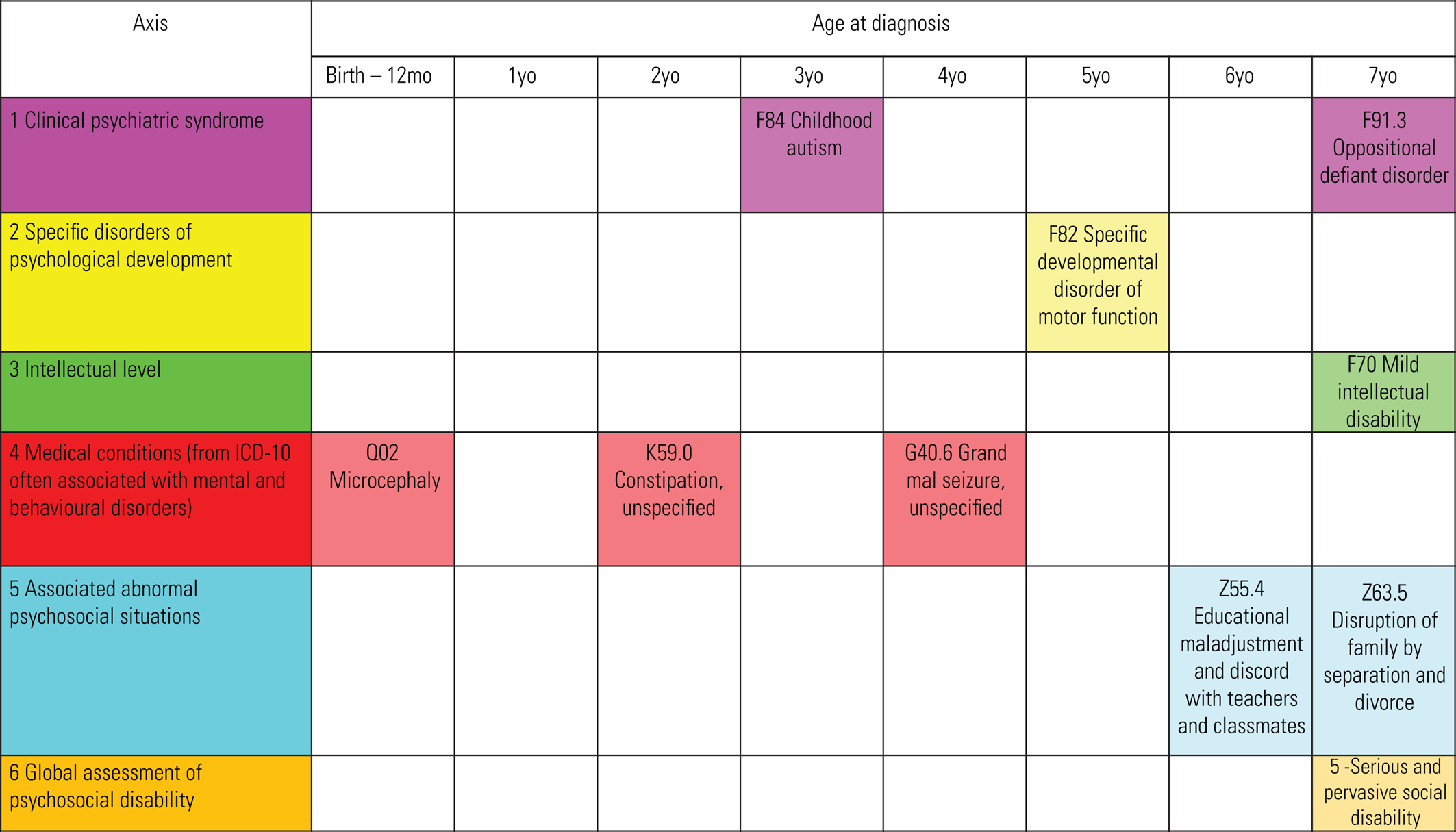
Here the simplified format shows, at a glance, the interrelationships in time. In this hypothetical case further enquiry shows parental discord occurring in the year before the parents separated and this fits at least in time with a previous deterioration at school. The increasing behavioural problems that have emerged have triggered a request by the psychiatrist for an assessment of cognitive ability. An additional diagnosis of mild intellectual disability was made after the WISC-V and an adaptive behaviour scale were completed. Axis Six could be further used to code a series of measurements across time.
This construction of a developmental multiaxial framework has many possible uses and can helpfully integrate the research evidence on developmental timings, while a knowledge of the ‘continuities and discontinuities in psychopathology’ in children and adolescents (Rutter Reference Rutter, Kim-Cohen and Maughan2006) can also be usefully brought to bear (Kessler Reference Kessler, Berglund and Demler2005; Beesdo Reference Beesdo, Knappe and Pine2009; Lijster Reference Lijster, Dierckx and Utens2017; Thapar Reference Thapar and Riglin2020). Furthermore, although the exact manner in which adverse childhood experiences (ACEs) operate in producing childhood psychopathology remains unclear, the evidence points to substantial impacts and the age at which they occur is likely to be very relevant to predicting the effects (Sonuga-Barke Reference Sonuga-Barke, Kennedy and Kumsta2017; Danese Reference Danese and Lewis2022). All in all, a system that allows the easy integration of a developmental or ‘lifespan’ approach can provide assistance in the analysis of cases, especially if complex. Symptoms over time can also be tracked and this may be valuable in any aetiological hypotheses. In more complex cases, as discussed further below, this approach has clinical utility in assessing medication response over time, as well as tracking the general level of psychosocial disability and the impact on functioning of underlying problems, diagnoses and intervention.
Figure 5 shows in a very simplified manner how other symptoms of concern can be added, along with their chronology. The mental health symptoms can be gathered in Axis One and then the age at which the symptoms were first identified or recorded added to the table. From the further history elucidated in this case a symptom of anxiety was found to have been present from at least the time of the initial diagnosis of autism. Subsequently, low mood, aggression and oppositionality have emerged as symptoms and more recently the young child has engaged in self-biting.

FIG 5 Chronological data – diagnoses and symptoms using Axes 1–6 (One to Six) of the ICD-10 multiaxial classification system (World Health Organization (1996).
Use of the ICD-10 framework in analysing complex cases, symptom chronology and medication response
Presented above in the hypothetical case of a young boy it has been portrayed how symptoms can be added to a simple presentation. Sometimes, however, complex cases arise that require an even more thorough clinical analysis. Often this occurs when the patient has been in the service for some time without a satisfactory outcome, or when significant deterioration of symptoms has occurred. A similar approach to that of Figs 4 and 5 could assist in the process and in this case a spreadsheet could be utilised to help with it. Let us assume another hypothetical case in which a consultant paediatric colleague has contacted you in your capacity as the child psychiatry consultation liaison consultant. The case in question is of a 12-year-old girl with Prader–Willi syndrome as the only current diagnosis, and although the eating behaviour has been well managed (with weight within the average range) other significant challenging behaviours have emerged and medication tried. Complicating the case have been frequent moves geographically, such that the young person has been in and out of different paediatric services. The family has presented to the current service in the past few months. There are many notes available, and the psychiatry and paediatric registrars are available to assist. To use the ICD-10 multiaxial framework in this case may very well provide a helpful analysis of a complicated clinical case. First, from the notes is extracted the information to populate the multiaxial schema and, as in the example above of the GP letter, some coding could initially take place, particularly regarding any Z codes. However, it is not necessary to be extremely formal at this stage, especially as in Axis One symptoms, not diagnoses, can be initially gathered and their place in time subsequentially indicated. Chart analysis of this type can be initially complicated and ‘messy’, but the simplified example in Fig. 6 shows the general idea.

FIG 6 Symptom and medication chronology using Axes 1–6 (One to Six) of the ICD-10 multiaxial classification system (World Health Organization (1996). ADOS, Autism Diagnostic Observation Schedule; MDT, multidisciplinary team; ASD, autism spectrum disorder; Yr, year; WISC-V, Wechsler Intelligence Scale for Children Fifth Edition; FSIQ, Full-Scale Intelligence Quotient.
Axis Four can now serve to identify the medications trialled, doses and symptomatic control achieved (or not), by virtue of comparison with symptom resolution on Axis One. This process can often also identify medication groups that have not been tried and suggest avenues for future medication trials if thought clinically appropriate. Regarding the symptoms and potential diagnoses, these can be correlated with knowledge of the disorder in question, in this case Prader–Willi syndrome. So, if it is found, for instance, that there are suggestions of peer relationship problems and established issues in social communication, a formal diagnosis of autism spectrum disorder (ASD) could be formally considered, as from the literature, ASD has a significant co-occurrence with Prader–Willi syndrome (Dykens Reference Dykens, Lee and Roof2011). Likewise, intellectual disability can be a feature of Prader–Willi syndrome and if this is an area of concern then checking for previous testing might help to exclude this diagnosis. If testing has never taken place, as in this case, then it becomes one of the recommendations. In Axis Five an eye would be kept out for any significant psychosocial factors and in Axis Six it would be useful to try to gauge as far as possible the severity of any psychosocial disability related to the condition.
Figure 6 shows the final multiaxial scheme (in spreadsheet format) and how it might appear. At the top of the chart is the age and timeline. The chart has been populated from the information gathered. In this case it seems that generally, symptoms had deteriorated up until the referral to the current treating paediatric team, except for a brief period where the mother had instituted strict boundaries (age 8). The first vertical green column shows suggested intervention after a multiaxial analysis (the chart to the left of the first green column shows the historical information recorded). The three subsequent out-patient appointments after the multiaxial analysis are shown to the right, and the final vertical green column at the extreme right shows the outcomes of the suggested interventions. The outcomes include established diagnoses of ASD, with the standardised testing for speech and language and scholastic skills, in keeping with the diagnosis of intellectual disability (supported by the WISC-V and ABAS scores). The increase in risperidone was suggested during the appointment in November 2019 because since its introduction in February 2019 there appeared to be a response with less aggression. The introduction of the selective serotonin reuptake inhibitor (SSRI) was suggested to manage the anxiety symptoms and given the evidence base for its use (like risperidone) in Prader–Willi syndrome (Bonnot Reference Bonnot, Cohen and Thuilleaux2016). The N-acetylcysteine (NAC) had been started prior to the move to the new home and was continued for the skin picking, but the SSRI appeared to have a greater effect. In Axis Five suggestions were made for entry into a local special school, with increased one-to-one support recommended as well as funding for overnight respite. A global assessment of psychosocial disability score has been attempted in Axis Six for the period prior to entry into the current paediatric service and within the current episode of care, as has a CGAS.
Suggestions for including positive, resilience and cultural factors
The ICD-10 multiaxial framework in both its classic usage and its variant uses as described above is very useful for collecting data relevant to understanding and making diagnoses in clinical cases. There is an argument, however, that although it is understandably focused on collecting the information on clinical pathology and potential negative environmental exposure it does not collect any direct positive, resilience or compensatory factors. In Fig. 6 the ABAS report was placed in Axis Three, where along with the FSIQ it allowed a diagnosis of mild intellectual disability. However, if the ABAS had hypothetically identified some significant strengths in functioning (perhaps showing better adaptive skills than might be predicted from the FSIQ), this potentially important information might be lost among the intellectual disability diagnosis. Might Axis Six be used to accumulate such positive functional descriptors and other strengths in psychosocial functioning? Also, although it is clear that there are negative impacts on a child of environmental adverse childhood experiences (ACEs) and these ACEs can be collected in Axis Five, might there also be an argument for the expanded use of the multiaxial framework for including information on protective, resilience and compensatory factors, as these have been shown to have significant modulating effects (Rutter Reference Rutter2012; Crandall Reference Crandall, Miller and Cheung2019)? Also, Axis Five might serve as a repository for the key issues in any cultural formulation of the child and family as per DSM-5.
Conclusions
Classification in psychiatry in general, and in child psychiatry in particular, remains a highly complex and continuously developing area (Cantwell Reference Cantwell1996; Scott Reference Scott2002; Taylor Reference Taylor, Rutter, Rutter, Bishop and Pine2008; Rutter Reference Rutter2011; Uher Reference Uher and Rutter2012; Surís Reference Surís, Holliday and North2016; Clark Reference Clark, Cuthbert and Lewis-Fernández2017; Gaebel Reference Gaebel, Stricker and Kerst2020).
Those that contributed to the development of the ICD-10 multiaxial classification system with their foresight and empirical testing have gifted a practical and usable framework which, decades on, continues to provide enormous clinical utility. In terms of limitations it should be remembered, however, that over the years there have been many multiaxial systems proposed with different designated axes/number of axes and that the choice of axes is often based on ‘looking for a group of quasi-independent clinical aspects representing a reasonable combination of parsimony and richness of information’ (Mezzich Reference Mezzich1979). It is therefore important that no classification system become reified, as there may be further improvements that can still emerge and multiaxial classification, like psychiatric classification in general, has itself a complex history. It is also the case that there are added complexities in inter-axis relationships, that is although the axes may be separated for the purpose of providing clinical utility, they often have significant relationships to each other (Mezzich Reference Mezzich1979).
The multiaxial system developed for child and adolescent psychiatry by the ICD has stood the test of time for many reasons, including its eminently atheoretical approach and very practical nature. This is because clinicians can see that it reflects, far more comprehensively, the clinical picture of a child within their environment. This article suggests some additional usages of the multiaxial system beyond the standard classic use already developed for ICD-10 (WHO 1996). In many ways the multiaxial biopsychosocial framework is best seen as a logical extension of the comprehensive assessment already entirely familiar to the child and adolescent psychiatrist, once the rationale for dividing up the information among the six axes is fully appreciated. Beyond this it has potential to provide a common framework across the multidisciplinary child mental health space, as well as being helpful as a shared clinical tool in communicating with paediatric colleagues (Mayall Reference Mayall, Teoh and McDermott2022).
Future directions
Although the ICD multiaxial system for children and adolescents has had its ‘field tests’ and improvements in the past, which have shown its acceptability and usefulness, with potential to enhance diagnostic reliability (Rutter Reference Rutter, Lebovici and Eisenberg1969, Reference Rutter, Shaffer and Shephard1975; Skovgaard Reference Skovgaard, Isager and Jorgensen1988; van Goor-Lambo Reference van Goor-Lambo, Orley and Poustka1990; Shaffer Reference Shaffer, Gould and Rutter1991), there remain questions as to its current frequency of clinical usage and its utility in practical clinical terms for contemporary clinicians. Do clinicians find it useful and do they use it in their clinical practice? If so, which parts of the classic/extended format outlined above might be most useful? We hope to address these questions in an assessment of a teaching module for junior psychiatrists, paediatricians and other mental health professionals in the near future for which ethics approval has already been sought and granted (the corresponding author, M.M., can be contacted regarding any details). There are clearly training and resource issues, as well as the need to address time constraints in busy clinical areas, and all these might affect the use and usefulness of the multiaxial system. Might it be helpful in ongoing clinical communication, especially in clinics where there are complex cases and a frequent turnover of medical staff? How far can the multiaxial system support a robust mental health formulation? Might it be of value in clinical discussions with children/ adolescents and their families to show both the complexity of a presenting problem and how different areas require different solutions? These questions and many others remain.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bja.2023.39.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Author contributions
M.M.: conceptualisation, original draft preparation and rewriting, final editing. B.M., R.S., Y.T., M.B. and S.N.: writing, review, editing.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
MCQs
Select the single best option for each question stem
1 How many axes does the current ICD-10 multiaxial classification system for child and adolescent psychiatry have?
a five
b three
c four
d six
e none.
2 Which of the following diagnostic systems allowed/allows multiaxial classification in some form?
a DSM-III
b DC0–5
c DSM-IV
d ICD-10
e all of the above.
3 Which of the following is not a recognisable rationale/characteristic of the ICD-10 multiaxial classification for child and adolescent psychiatry?
a it stops clinicians being forced to choose between non-exclusive diagnoses
b it has an atheoretical approach
c it allows a biopsychosocial approach
d it creates definitive aetiology for each diagnosis
e it has an axis for psychosocial disability.
4 In the ICD-10 multiaxial classification for child and adolescent psychiatry which axis covers physical or medical conditions?
a Axis Three
b Axis Four
c Axis Two
d Axis Five
e Axis One.
5 In the extended use of the ICD-10 multiaxial system of classification outlined in this article, what additional uses are suggested?
a planning of psychotherapeutic interventions
b analysis of complex cases, including medication response
c hypothesising about differential diagnosis
d reviewing symptom chronology
e all of the above.
MCQ answers
1 d 2 e 3 d 4 b 5 e














 Open access
Open access
eLetters
No eLetters have been published for this article.