

No CrossRef data available.
Article contents
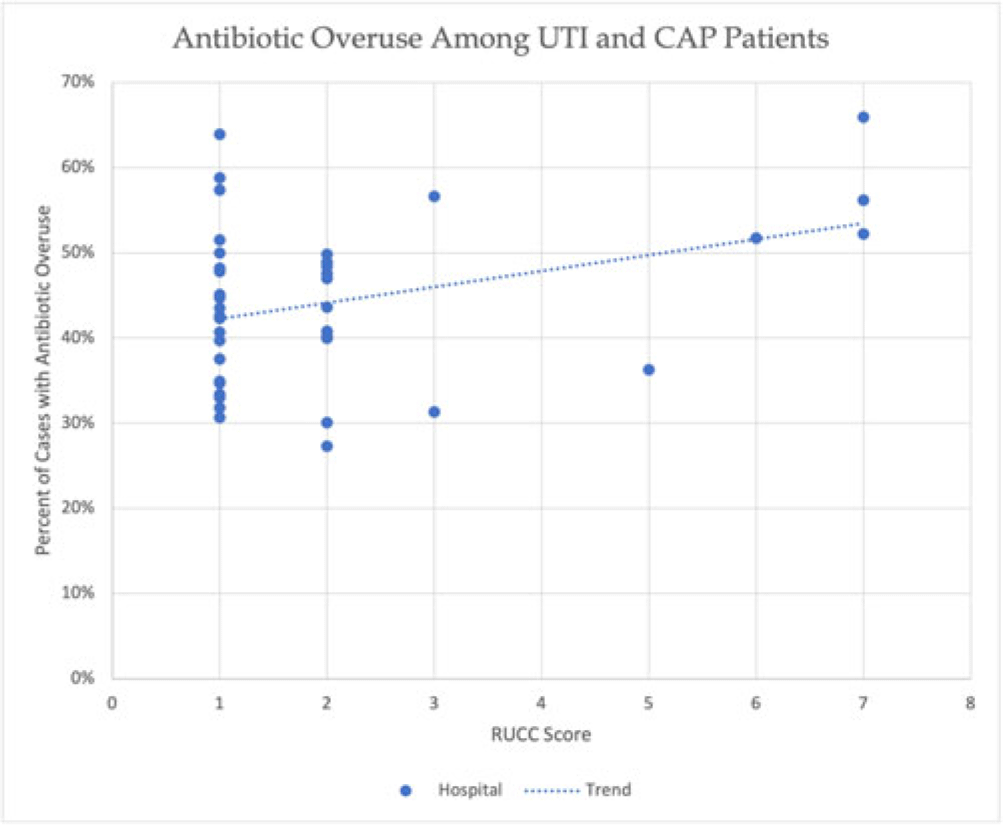
Identifying the relationship between hospital rurality and antibiotic overuse
Published online by Cambridge University Press: 29 September 2023
Abstract
Core share and HTML view are not available for this content. However, as you have access to this content, a full PDF is available via the ‘Save PDF’ action button.
Background: Antibiotic overuse and the resulting patient outcomes span all hospitals. However, although antibiotic stewardship can improve antibiotic use, effective stewardship programs require expertise and an infrastructure that are not present in all hospitals. Rural hospitals have less access to resources, infectious disease expertise, and participation in academic research. Thus, we compared antibiotic overuse at discharge between rural and nonrural hospitals for patients diagnosed with community-associated pneumonia (CAP) or urinary tract infection (UTI)—the 2 most common hospital infections. Methods: To determine whether antibiotic overuse at discharge was higher among rural versus nonrural hospitals, we analyzed data from a 41-hospital prospective cohort of patients treated for CAP or UTI between July 1, 2017, and July 30, 2019, in Michigan. Antibiotic overuse was defined as treatment that was unnecessary (ie, patient did not have an infection), excessive (ie, duration >4 days for CAP), or included suboptimal fluoroquinolone use (ie, safer alternative available). Overuse was determined based on patient risk factors, symptoms, allergies, diagnostic results, and time to stability. Hospital rurality was defined using the Rural–Urban Continuum Codes (RUCC) score. We defined rural as a score ≥4 and very rural as a score of 7–9. We used t tests to compare the mean percentage of patients with antibiotic overuse at discharge between nonrural and rural (and very rural) hospitals. Results: Across 41 hospitals, we included 23,449 patients with CAP or UTI. There were 5 rural (and 3 very rural) hospitals with 2,039 (and 1,082) patients. Antibiotic overuse at discharge was present in 43.1% of patient cases in nonrural hospitals, 52.5% in rural hospitals (P = .04 vs nonrural) and 58.1% in very rural hospitals (P = .007 vs nonrural). Compared to nonrural hospitals, the mean percentage of cases with antibiotic overuse at discharge in rural hospitals was 9.4% higher (15.1% higher in very rural hospitals). Results were similar in a subgroup analysis of only patients with UTI (47.0% in rural vs 37.5% in nonrural, mean difference, 9.5%; P = .03) but were not statistically significant in patients with CAP (53.8% vs 48.0%, respectively; mean difference, 5.8%; P = 0.23). Conclusions: In this retrospective study, rural hospitals—especially very rural hospitals, had higher rates of antibiotic overuse at discharge than nonrural hospitals. Our findings suggest that antibiotic stewardship interventions tailored toward the unique differences in infrastructure, resources, and needs of rural hospitals are essential to community health.
Disclosures: None
- Type
- Antibiotic Stewardship
- Information
- Antimicrobial Stewardship & Healthcare Epidemiology , Volume 3 , Issue S2: SHEA Spring 2023 Abstracts , June 2023 , pp. s34 - s35
- Creative Commons

 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.- Copyright
- © The Author(s), 2023. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
 You have
Access
You have
Access
 Open access
Open access