


 Open access
Open access
Crossref Citations
This article has been cited by the following publications. This list is generated based on data provided by Crossref.
Harun, Md. Golam Dostogir
Anwar, Md Mahabub Ul
Sumon, Shariful Amin
Hassan, Md Zakiul
Haque, Tahmidul
Mah-E-Muneer, Syeda
Rahman, Aninda
Abdullah, Syed Abul Hassan Md
Islam, Md Saiful
Styczynski, Ashley R.
and
Kaydos-Daniels, S. Cornelia
2022.
Infection prevention and control in tertiary care hospitals of Bangladesh: results from WHO infection prevention and control assessment framework (IPCAF).
Antimicrobial Resistance & Infection Control,
Vol. 11,
Issue. 1,
Harun, Md. Golam Dostogir
Anwar, Md Mahabub Ul
Sumon, Shariful Amin
Abdullah-Al-Kafi, Md
Datta, Kusum
Haque, Md. Imdadul
Chowdhury, A. B. M. Alauddin
Sharmin, Sabrina
Islam, Md Saiful
and
Prins, Cindy
2022.
Pre-COVID-19 knowledge, attitude and practice among nurses towards infection prevention and control in Bangladesh: A hospital-based cross-sectional survey.
PLOS ONE,
Vol. 17,
Issue. 12,
p.
e0278413.
Anwar, Md. Mahabub Ul
Sumon, Shariful Amin
Mohona, Tahrima Mohsin
Rahman, Aninda
Md Abdullah, Syed Abul Hassan
Islam, Md. Saiful
and
Harun, Md. Golam Dostogir
2023.
Uptake of Influenza Vaccine and Factors Associated with Influenza Vaccination among Healthcare Workers in Tertiary Care Hospitals in Bangladesh: A Multicenter Cross-Sectional Study.
Vaccines,
Vol. 11,
Issue. 2,
p.
360.
Harun, M.G.D.
Anwar, M.M.U.
Sumon, S.A.
Mohona, T.M.
Hassan, M.Z.
Rahman, A.
Abdullah, S.A.H.M.
Islam, M.S.
Oakley, L.P.
Malpiedi, P.
Kaydos-Daniels, S.C.
and
Styczynski, A.R.
2023.
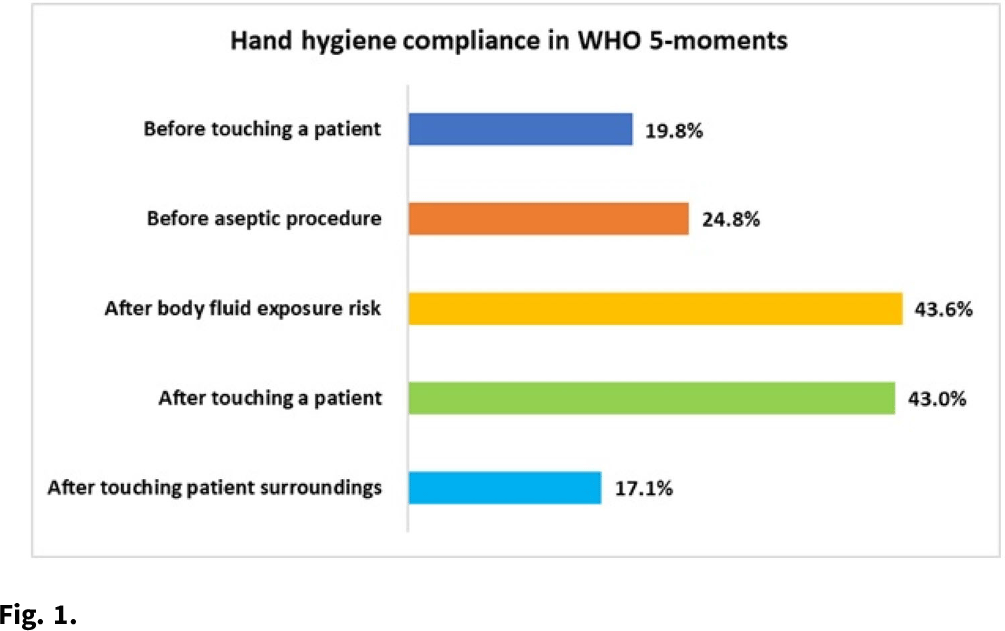
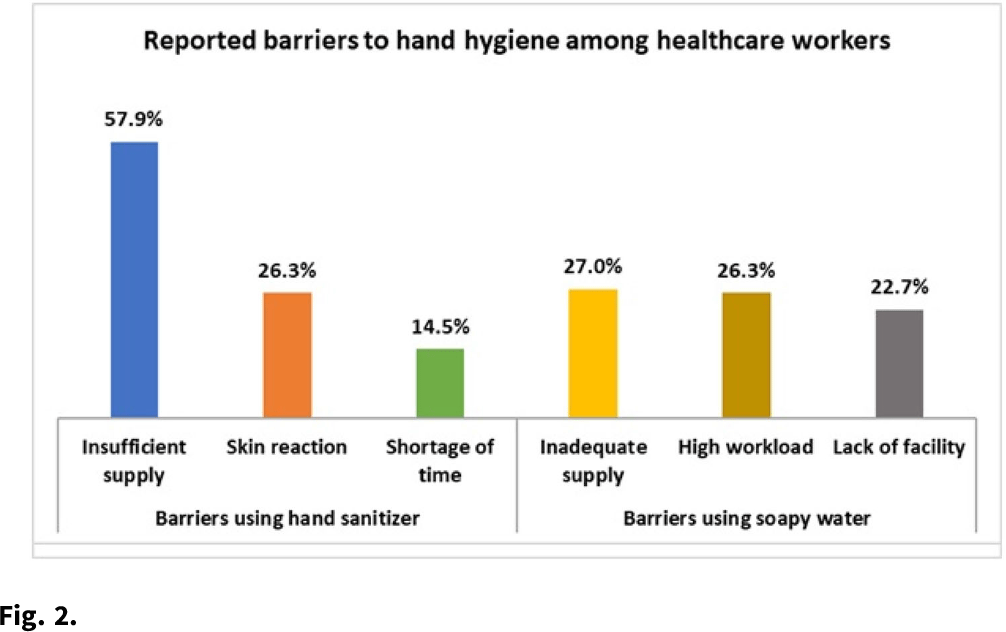
Hand hygiene compliance and associated factors among healthcare workers in selected tertiary-care hospitals in Bangladesh.
Journal of Hospital Infection,
Vol. 139,
Issue. ,
p.
220.