
2041 results
Modelling habitat suitability for the Critically Endangered Manumea or Tooth-billed Pigeon Didunculus strigirostris using past and present baselines
-
- Journal:
- Bird Conservation International / Volume 34 / 2024
- Published online by Cambridge University Press:
- 18 September 2024, e20
-
- Article
- Export citation
Central bank digital currencies: an old tale with a new chapter
-
- Journal:
- Financial History Review , First View
- Published online by Cambridge University Press:
- 18 September 2024, pp. 1-29
-
- Article
- Export citation
Application of a Model Using Prior Healthcare Information to Predict Multidrug-Resistant Organism (MDRO) Carriage
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s111
-
- Article
-
- You have access
- Open access
- Export citation
-
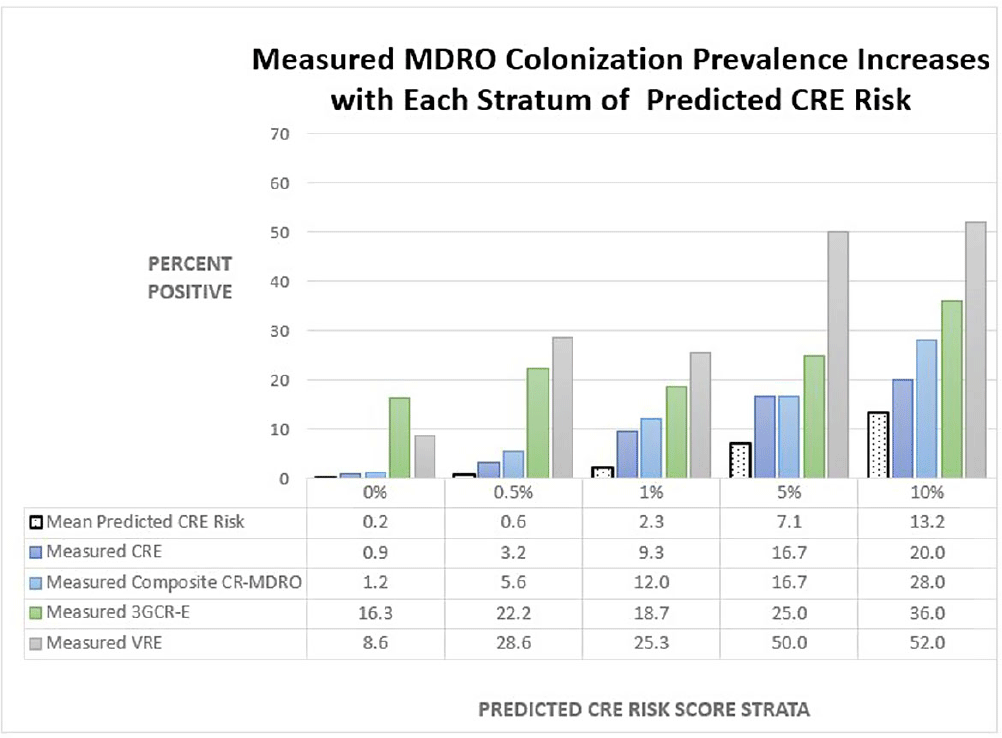
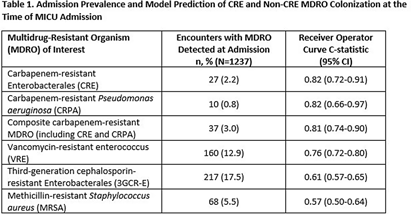
Background: Early identification of patients colonized with MDROs can help healthcare facilities improve infection control and treatment. We evaluated whether a model previously validated to predict carbapenem-resistant Enterobacterales (CRE) carriage on hospital admission (area under the curve [AUC]=0.86, Lin et al. OFID 2019) would generalize to predict a patient’s likelihood of CRE and non-CRE MDRO colonization at the time of medical intensive care unit (MICU) admission. Methods: We analyzed data collected previously in a retrospective observational cohort study of patients admitted to Rush University Medical Center’s MICU from 1/2017-1/2018 and screened within the first two days for rectal MDRO colonization. Organisms of interest included CRE, carbapenem-resistant Pseudomonas aeruginosa (CRPA), vancomycin-resistant enterococci (VRE), and third-generation cephalosporin-resistant Enterobacterales (3GCR-E). Methicillin-resistant Staphylococcus aureus (MRSA) nasal colonization at admission was determined by routine clinical screening. Each patient’s first MICU admission during the study period was linked to Illinois’ hospital discharge database and assigned a CRE colonization risk probability using the existing model. Model covariates were age, and during the prior 365 days, number of short-term acute care hospitalizations (STACH) and mean STACH length of stay, number of long-term acute care hospitalizations (LTACH) and mean LTACH length of stay, prior hospital admission with an ICD-10 diagnosis code indicating bacterial infection, and current admission to LTACH. Predictive value of the model was evaluated by receiver operating characteristic (ROC) curves. Results: We analyzed 1237 MICU admissions. MDRO admission prevalence is shown in the Table. The model performed well to predict carriage of healthcare-associated MDROs, including CRE, CRPA, composite CR-MDROs (CRE & CRPA), and VRE. However, the model performed poorly for MDROs with known community reservoirs, including 3GCR-E and MRSA (Table). In general, MDRO admission prevalence increased in parallel with predicted CRE colonization risk (Figure). The number needed to screen (NNS) to detect one healthcare-associated MDRO carrier was inversely related to the CRE colonization risk score. For example, NNS in the total cohort compared to those with CRE risk score of >0.5% was: CRE 111 vs 32 patients, CRPA 333 vs 42 patients, composite CR-MDRO 83 vs 18 patients, and VRE 12 vs 4 patients. However, higher CRE risk score cutoff was inversely related to screening sensitivity. Conclusion: A prediction model using prior healthcare exposure information successfully discriminated patients likely to harbor healthcare-associated MDROs upon MICU admission. Prediction scores generated by a public-health accessible database could be used to target screening/isolation or enact protective measures for high-risk patients.


A Comparison of Variable Input Strategies used for Risk-adjustment Models of Antimicrobial Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s30-s31
-
- Article
-
- You have access
- Open access
- Export citation
-
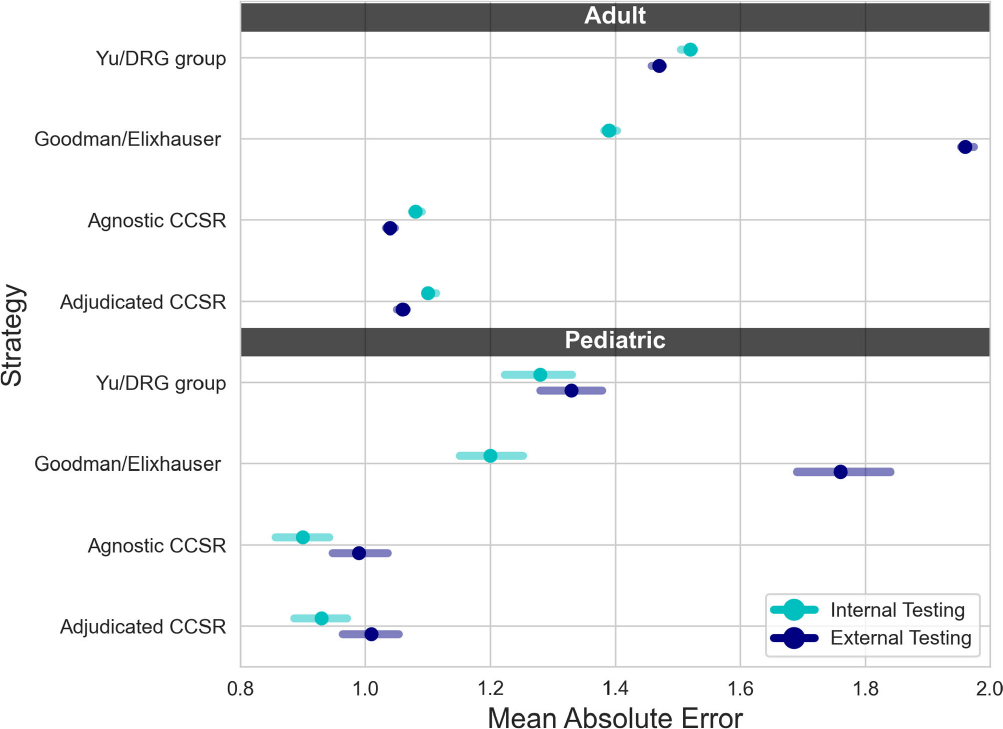
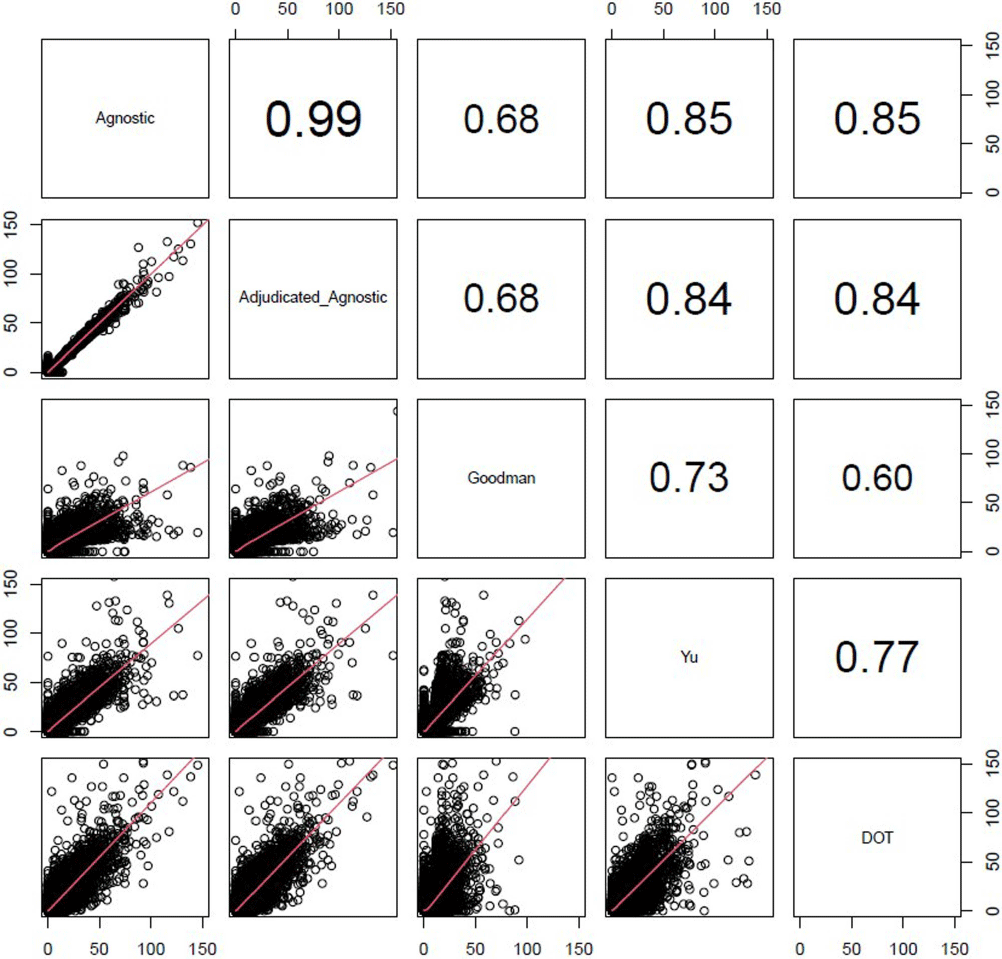
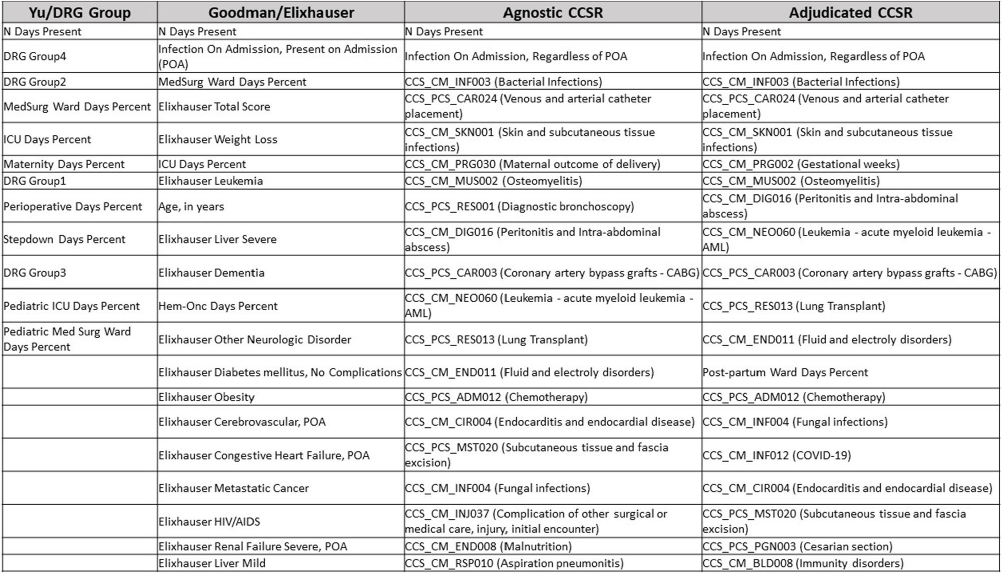
Background: External comparisons of antimicrobial use (AU) may be more informative if adjusted for encounter characteristics. Optimal methods to define input variables for encounter-level risk-adjustment models of AU are not established. Methods: This retrospective analysis of electronic health record data included 50 US hospitals in 2020-2021. We used NHSN definitions for all antibacterials days of therapy (DOT), including adult and pediatric encounters with at least 1 day present in inpatient locations. We assessed 4 methods to define input variables: 1) diagnosis-related group (DRG) categories by Yu et al., 2) adjudicated Elixhauser comorbidity categories by Goodman et al., 3) all Clinical Classification Software Refined (CCSR) diagnosis and procedure categories, and 4) adjudicated CCSR categories where codes not appropriate for AU risk-adjustment were excluded by expert consensus, requiring review of 867 codes over 4 months to attain consensus. Data were split randomly, stratified by bed size as follows: 1) training dataset including two-thirds of encounters among two-thirds of hospitals; 2) internal testing set including one-third of encounters within training hospitals, and 3) external testing set including the remaining one-third of hospitals. We used a gradient-boosted machine (GBM) tree-based model and two-staged approach to first identify encounters with zero DOT, then estimate DOT among those with >0.5 probability of receiving antibiotics. Accuracy was assessed using mean absolute error (MAE) in testing datasets. Correlation plots compared model estimates and observed DOT among testing datasets. The top 20 most influential variables were defined using modeled variable importance. Results: Our datasets included 629,445 training, 314,971 internal testing, and 419,109 external testing encounters. Demographic data included 41% male, 59% non-Hispanic White, 25% non-Hispanic Black, 9% Hispanic, and 5% pediatric encounters. DRG was missing in 29% of encounters. MAE was lower in pediatrics as compared to adults, and lowest for models incorporating CCSR inputs (Figure 1). Performance in internal and external testing was similar, though Goodman/Elixhauser variable strategies were less accurate in external testing and underestimated long DOT outliers (Figure 2). Agnostic and adjudicated CCSR model estimates were highly correlated; their influential variables lists were similar (Figure 3). Conclusion: Larger numbers of CCSR diagnosis and procedure inputs improved risk-adjustment model accuracy compared with prior strategies. Variable importance and accuracy were similar for agnostic and adjudicated approaches. However, maintaining adjudications by experts would require significant time and potentially introduce personal bias. If findings are confirmed, the need for expert adjudication of input variables should be reconsidered.
Disclosure: Elizabeth Dodds Ashley: Advisor- HealthTrackRx. David J Weber: Consultant on vaccines: Pfizer; DSMB chair: GSK; Consultant on disinfection: BD, GAMA, PDI, Germitec



Historical and archaeogenomic identification of high-status Englishmen at Jamestown, Virginia
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Contents
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp v-v
-
- Chapter
- Export citation
Bibliography
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 183-207
-
- Chapter
- Export citation
Acknowledgements
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp vi-viii
-
- Chapter
- Export citation
4 - The War of Position
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 108-143
-
- Chapter
- Export citation
Index
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 208-211
-
- Chapter
- Export citation
2 - The Gramscian Right, or Turning Gramsci on His Head
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 34-66
-
- Chapter
- Export citation
Copyright page
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp iv-iv
-
- Chapter
- Export citation
1 - A Diverse and Global Right
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 1-33
-
- Chapter
- Export citation
5 - The Right World
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 144-182
-
- Chapter
- Export citation
3 - Deconstructing the Global Administrative State
-
- Book:
- World of the Right
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024, pp 67-107
-
- Chapter
- Export citation
World of the Right
- Radical Conservatism and Global Order
-
- Published online:
- 13 June 2024
- Print publication:
- 27 June 2024
Trust, Guilds, and Kinship in London, 1330–1680
-
- Journal:
- The Historical Journal , First View
- Published online by Cambridge University Press:
- 30 May 2024, pp. 1-24
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Líĺwat Climbers Could See the Ocean from the Peak of Qẃelqẃelústen: Evaluating Oral Traditions with Viewshed Analyses from the Mount Meager Volcanic Complex Prior to Its 2360 BP Eruption
-
- Journal:
- American Antiquity , First View
- Published online by Cambridge University Press:
- 23 May 2024, pp. 1-21
-
- Article
- Export citation
Electrophysiological correlates of inhibitory control in children: Relations with prenatal maternal risk factors and child psychopathology
-
- Journal:
- Development and Psychopathology , First View
- Published online by Cambridge University Press:
- 24 April 2024, pp. 1-14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
76 Lessons learned during implementation of OMOP common data model across multiple health systems
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 20
-
- Article
-
- You have access
- Open access
- Export citation
