
40 results
Implementation of a diagnostic stewardship intervention to improve blood-culture utilization in 2 surgical ICUs: Time for a blood-culture change
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 4 / April 2024
- Published online by Cambridge University Press:
- 11 December 2023, pp. 452-458
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Implementation of diagnostic stewardship in two surgical ICUs: Time for a blood-culture change
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s9-s10
-
- Article
-
- You have access
- Open access
- Export citation
-
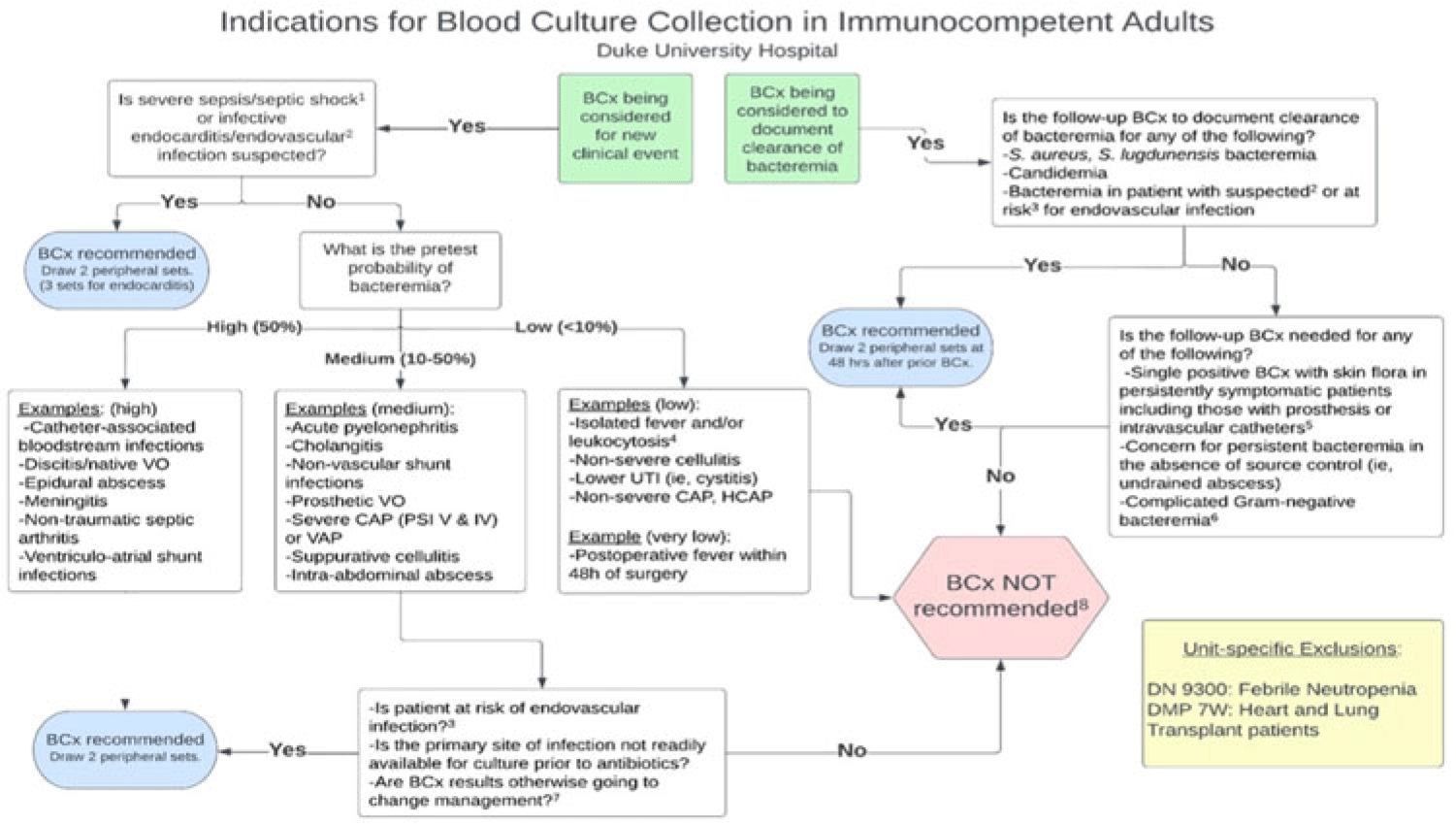
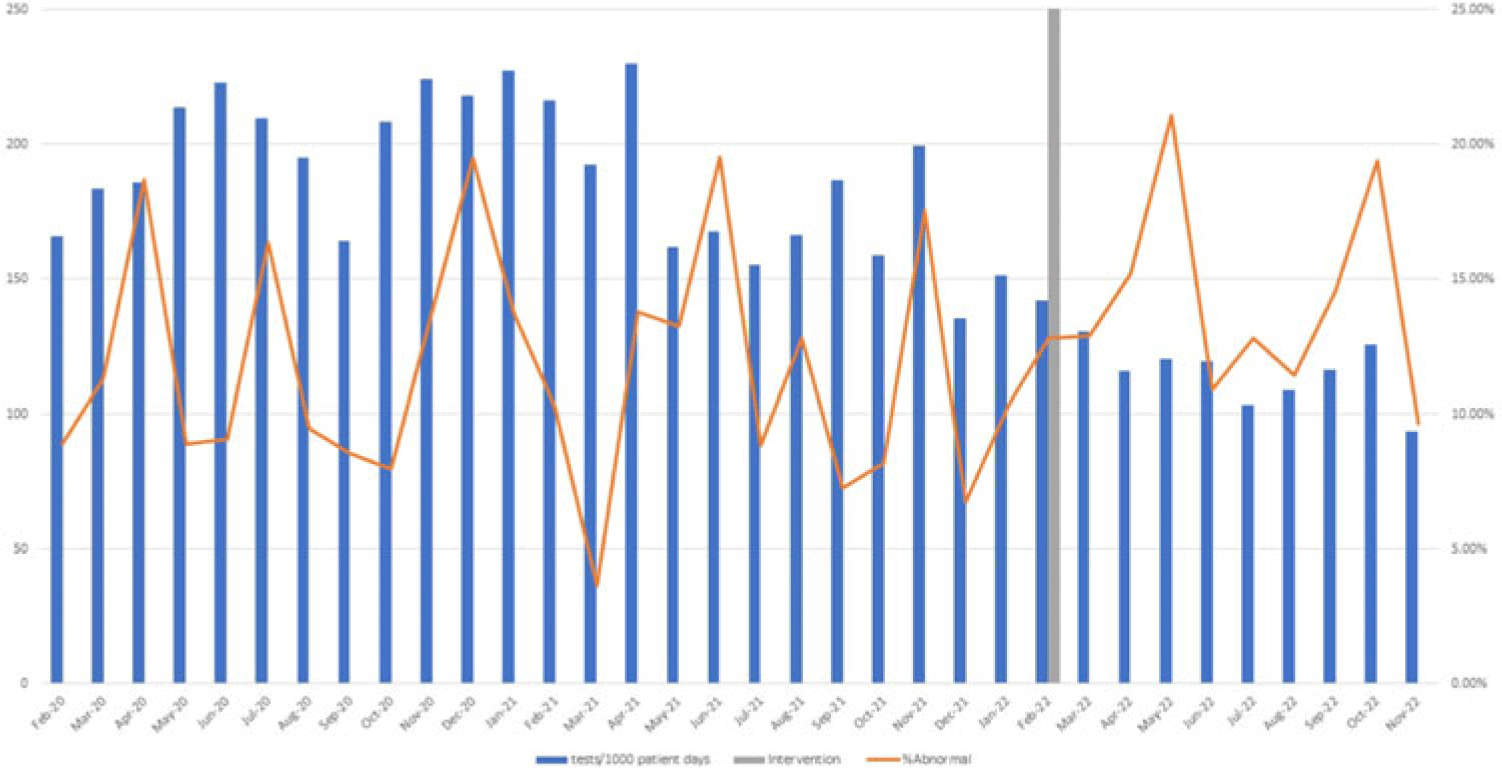
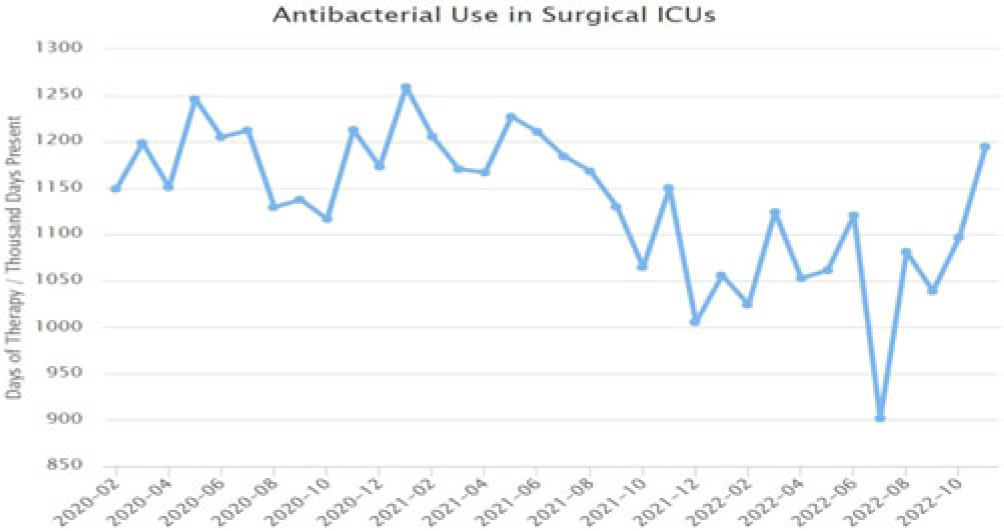
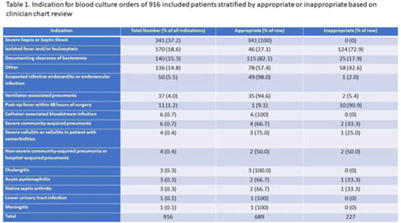
Background: Blood cultures are commonly ordered for patients with low risk of bacteremia. Liberal blood-culture ordering increases the risk of false-positive results, which can lead to increased length of stay, excess antibiotics, and unnecessary diagnostic procedures. We implemented a blood-culture indication algorithm with data feedback and assessed the impact on ordering volume and percent positivity. Methods: We performed a prospective cohort study from February 2022 to November 2022 using historical controls from February 2020 to January 2022. We introduced the blood-culture algorithm (Fig. 1) in 2 adult surgical intensive care units (ICUs). Clinicians reviewed charts of eligible patients with blood cultures weekly to determine whether the blood-culture algorithm was followed. They provided feedback to the unit medical directors weekly. We defined a blood-culture event as ≥1 blood culture within 24 hours. We excluded patients aged <18 years, absolute neutrophil count <500, and heart and lung transplant recipients at the time of blood-culture review. Results: In total, 7,315 blood-culture events in the preintervention group and 2,506 blood-culture events in the postintervention group met eligibility criteria. The average monthly blood-culture rate decreased from 190 blood cultures per 1,000 patient days to 142 blood cultures per 1,000 patient days (P < .01) after the algorithm was implemented. (Fig. 2) The average monthly blood-culture positivity increased from 11.7% to 14.2% (P = .13). Average monthly days of antibiotic therapy (DOT) was lower in the postintervention period than in the preintervention period (2,200 vs 1,940; P < .01). (Fig. 3) The ICU length of stay did not change before the intervention compared to after the intervention: 10 days (IQR, 5–18) versus 10 days (IQR, 5–17; P = .63). The in-hospital mortality rate was lower during the postintervention period, but the difference was not statistically significant: 9.24% versus 8.34% (P = .17). The all-cause 30-day mortality was significantly lower during the intervention period: 11.9% versus 9.7% (P < .01). The unplanned 30-day readmission percentage was significantly lower during the intervention period (10.6% vs 7.6%; P < .01). Over the 9-month intervention, we reviewed 916 blood-culture events in 452 unique patients. Overall, 74.6% of blood cultures followed the algorithm. The most common reasons overall for ordering blood cultures were severe sepsis or septic shock (37%), isolated fever and/or leukocytosis (19%), and documenting clearance of bacteremia (15%) (Table 1). The most common indications for inappropriate blood cultures were isolated fever and/or leukocytosis (53%). Conclusions: We introduced a blood-culture algorithm with data feedback in 2 surgical ICUs and observed decreases in blood-culture volume without a negative impact on ICU LOS or mortality rate.
Disclosure: None




Multi-scale Visualization of Ferroelectric Domains in a Magnetically Frustrated TbInO3 Thin Film
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 1772-1774
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Associations between intake of calcium, magnesium and phosphorus and risk of pancreatic cancer: a population-based, case–control study in Minnesota
-
- Journal:
- British Journal of Nutrition / Volume 126 / Issue 10 / 28 November 2021
- Published online by Cambridge University Press:
- 26 January 2021, pp. 1549-1557
- Print publication:
- 28 November 2021
-
- Article
-
- You have access
- HTML
- Export citation
Staying in touch with the community: understanding self-reported health and research priorities in older Aboriginal Australians
-
- Journal:
- International Psychogeriatrics / Volume 32 / Issue 11 / November 2020
- Published online by Cambridge University Press:
- 21 November 2019, pp. 1303-1315
-
- Article
- Export citation
Johann Gottfried Wetzstein. Orientalist und preußischer Konsul im osmanischen Syrien (1849–1861). By Ingeborg Huhn. Islamkundliche Untersuchungen. Berlin: Klaus Schwarz Verlag, 2016. 396 pp. Appendixes. Notes. Bibliography. Glossary. Index. Figures. Tables. Maps. Indexes. €54.00, paper.
-
- Journal:
- Slavic Review / Volume 77 / Issue 1 / Spring 2018
- Published online by Cambridge University Press:
- 23 April 2018, pp. 222-223
- Print publication:
- Spring 2018
-
- Article
- Export citation
Late Quaternary Glacial History of the South Orkney Plateau, Antarctica
-
- Journal:
- Quaternary Research / Volume 33 / Issue 3 / May 1990
- Published online by Cambridge University Press:
- 20 January 2017, pp. 265-275
-
- Article
- Export citation
Use of Hyperspectral Remote Sensing to Evaluate Efficacy of Aquatic Plant Management
-
- Journal:
- Invasive Plant Science and Management / Volume 2 / Issue 3 / July 2009
- Published online by Cambridge University Press:
- 20 January 2017, pp. 216-229
-
- Article
- Export citation
Atatürk in the Nazi Imagination. By Stefan Ihrig. Cambridge, MA: Harvard University Press, 2014. Pp. 311. Cloth $29.95. ISBN 978-0674368378.
-
- Journal:
- Central European History / Volume 49 / Issue 1 / March 2016
- Published online by Cambridge University Press:
- 29 March 2016, pp. 138-139
- Print publication:
- March 2016
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Introduction to “A Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute Care Hospitals: 2014 Updates”
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 35 / Issue S2 / September 2014
- Published online by Cambridge University Press:
- 10 May 2016, pp. S1-S5
- Print publication:
- September 2014
-
- Article
-
- You have access
- Export citation
A Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute Care Hospitals: 2014 Updates
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 35 / Issue S2 / September 2014
- Published online by Cambridge University Press:
- 10 May 2016, pp. S21-S31
- Print publication:
- September 2014
-
- Article
-
- You have access
- Export citation
A Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute Care Hospitals: 2014 Updates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 35 / Issue 8 / August 2014
- Published online by Cambridge University Press:
- 10 May 2016, pp. 967-977
- Print publication:
- August 2014
-
- Article
- Export citation
Introduction to “A Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute Care Hospitals: 2014 Updates”
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 35 / Issue 5 / May 2014
- Published online by Cambridge University Press:
- 10 May 2016, pp. 455-459
- Print publication:
- May 2014
-
- Article
- Export citation
Contributors
-
-
- Book:
- Behavioral Emergencies for the Emergency Physician
- Published online:
- 05 April 2013
- Print publication:
- 21 March 2013, pp viii-xii
-
- Chapter
- Export citation
Notes on Contributors
-
-
- Book:
- Edith Wharton in Context
- Published online:
- 05 November 2012
- Print publication:
- 08 October 2012, pp ix-xvi
-
- Chapter
- Export citation
Notes on the contributors
-
-
- Book:
- The Future of Australian Federalism
- Published online:
- 05 April 2012
- Print publication:
- 08 March 2012, pp viii-xiii
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Christianity
- Published online:
- 05 August 2012
- Print publication:
- 20 September 2010, pp xi-xliv
-
- Chapter
- Export citation
Outcome of asymptomatic infection with rubella virus during pregnancy
-
- Journal:
- Journal of Hygiene / Volume 87 / Issue 2 / October 1981
- Published online by Cambridge University Press:
- 25 March 2010, pp. 147-154
-
- Article
-
- You have access
- Export citation
Fetal infection resulting from maternal rubella after the first trimester of pregnancy
-
- Journal:
- Journal of Hygiene / Volume 85 / Issue 3 / December 1980
- Published online by Cambridge University Press:
- 19 October 2009, pp. 381-391
-
- Article
-
- You have access
- Export citation
