
348 results
SHEA position statement on pandemic preparedness for policymakers: emerging infectious threats
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 19 July 2024, pp. 1-3
-
- Article
- Export citation
SHEA position statement on pandemic preparedness for policymakers: the role of healthcare epidemiologists in communicating during infectious diseases outbreaks
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-5
-
- Article
- Export citation
Society for Healthcare Epidemiology of America position statement on pandemic preparedness for policymakers: mitigating supply shortages
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-5
-
- Article
- Export citation
SHEA position statement on pandemic preparedness for policymakers: building a strong and resilient healthcare workforce
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-4
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
SHEA position statement on pandemic preparedness for policymakers: introduction and overview
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
SHEA position statement on pandemic preparedness for policymakers: pandemic data collection, maintenance, and release
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-5
-
- Article
- Export citation
Testing residual chloramine levels in tap water across sink locations in a US academic hospital setting
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 20 March 2024, pp. 1-2
-
- Article
- Export citation
The impact of minimally invasive surgical approaches on surgical-site infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 03 January 2024, pp. 557-561
- Print publication:
- May 2024
-
- Article
- Export citation
Strategies to maintain an N95 respirator supply during a pandemic supply-chain shortage
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 13 December 2023, pp. 688-689
- Print publication:
- May 2024
-
- Article
-
- You have access
- HTML
- Export citation
The impact of environmental cleaning protocol featuring PX-UV in reducing the incidence of multidrug-resistant gram-negative healthcare-associated infection and colonization in intensive care units in Thailand
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 13 December 2023, pp. 684-687
- Print publication:
- May 2024
-
- Article
- Export citation
Bacille Calmette-Guérin preparation and intravesical administration to patients with bladder cancer: Risks to healthcare personnel and patients, and mitigation strategies
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 4 / April 2024
- Published online by Cambridge University Press:
- 11 December 2023, pp. 520-525
- Print publication:
- April 2024
-
- Article
- Export citation
Effects of a hard stop for C. difficile testing: Provider uptake and patient outcomes
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s44
-
- Article
-
- You have access
- Open access
- Export citation
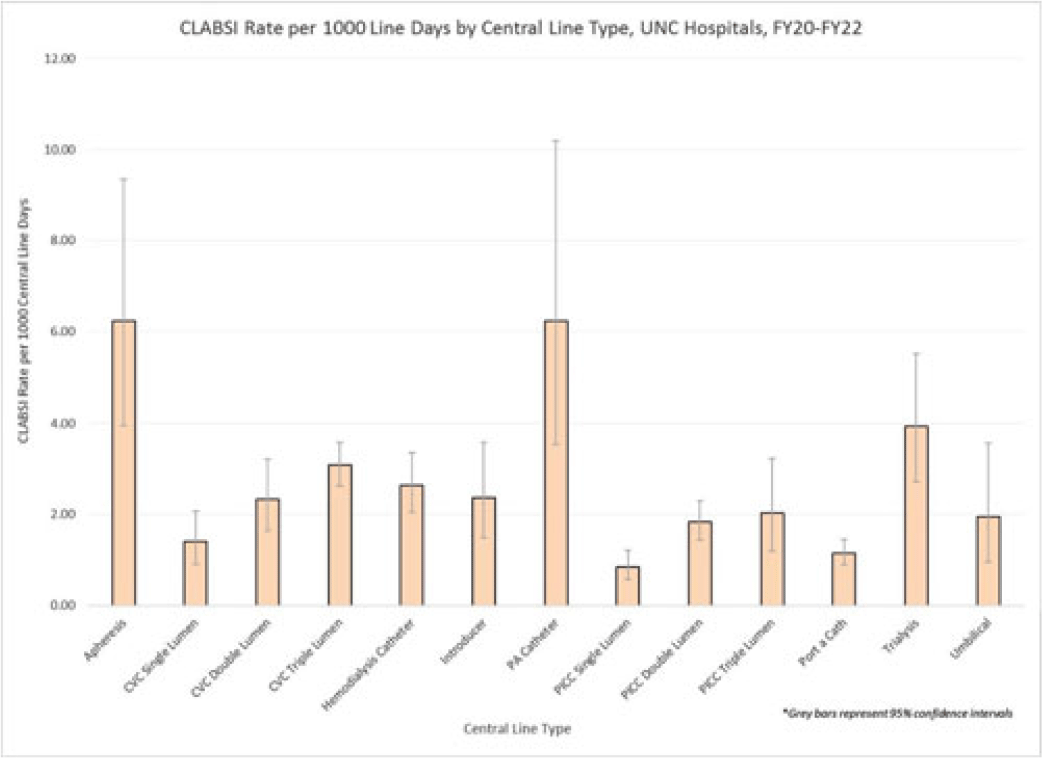
Examining CLABSI rates by central-line type
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s48-s49
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Central-line–associated bloodstream infections (CLABSIs) are linked to increased morbidity and mortality, longer hospital stays, and significantly higher healthcare costs. Infection prevention guidelines recommend line placement in specific insertion locations over others because of the relative risk of infection. The purpose of this study was to assess CLABSI rates by line type to determine whether some central lines had a lower risk of infection and should be recommended over others given similar clinical indications. Methods: At UNC Hospitals, data were obtained on central lines across a 3-year period (FY20–FY22) from the EMR (Epic Systems). Central lines were categorized as apheresis catheters, CVC lines (single, double, or triple lumen), hemodialysis catheters, introducer lines, pulmonary artery (PA) catheters, PICC lines (single, double, or triple lumen), port-a-catheters, trialysis catheters, or umbilical lines. The line type(s) associated with each CLABSI during the same period were recorded, and CLABSI rates by line type per 1,000 central-line days were calculated using SAS software. If an infection had >1 central-line device type associated, the infection was counted twice when calculating the CLABSI rate by line type. We calculated 95% CIs for each point estimate to assess for statistically significant differences in rates by line type. Results: During FY20–FY22, there were 264,425 central-line days and 458 CLABSIs, for an overall CLABSI rate of 1.73 CLABSIs per 1,000 central-line days. Also, 16% of patients with a CLABSI had >1 type of central line in place. Stratified data on CLABSI rates by each central-line type is presented in the Figure. CLABSI rates were highest in patients with apheresis lines (6.22; 95% CI, 3.96–9.35) and PA catheters (6.22; 95% CI, 3.54–10.20), and the lowest CLABSI rates occurred in patients with PICC lines (1.44; 95% CI, 1.19–1.73) and port-a-catheters (1.14; 95% CI, 0.89, 1.45). For both CVC and PICC lines, as the number of lumens increased from single to triple, CLABSI rates increased, from 0.91 to 2.63 and from 0.57 to 1.20, respectively. Conclusions: At our hospital, different types of central lines were associated with statistically higher CLABSI rates. Additionally, a higher number of lumens (triple vs single) in CVC and PICC lines were also associated with statistically higher CLABSI rates. These findings reinforce the importance of considering central-line type and number of lumens to minimize risk of CLABSI while ensuring that patients have the best line type based on their clinical needs.
Disclosures: None

Approaching coronavirus disease 2019 (COVID-19) vaccine hesitancy among healthcare personnel: The importance of cultural competency
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 18 July 2023, pp. 1371-1372
- Print publication:
- September 2023
-
- Article
- Export citation
The role of environmental and healthcare-associated infections in Asia: Lessons learned from the coronavirus disease 2019 (COVID-19) pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 15 June 2023, e100
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Impact of Chemical, Biological, Radiological, Nuclear and Explosive Events on Emergency Departments: An Integrative Review
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, p. s3
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
Diagnostic stewardship for Clostridioides difficile testing in an acute care hospital: A quality improvement intervention
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 05 April 2023, e67
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Strategies to prevent Clostridioides difficile infections in acute-care hospitals: 2022 Update
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 12 April 2023, pp. 527-549
- Print publication:
- April 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Reasons for cooperation and defection in real-world social dilemmas – ERRATUM
-
- Journal:
- Judgment and Decision Making / Volume 18 / 2023
- Published online by Cambridge University Press:
- 31 March 2023, e11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Implementation should be a standard component of practice guidelines and guidance documents
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 02 March 2023, pp. 1365-1368
- Print publication:
- September 2023
-
- Article
- Export citation
