

The publisher apologises for the two figures being incomplete in the published paper. The figures should be as below:
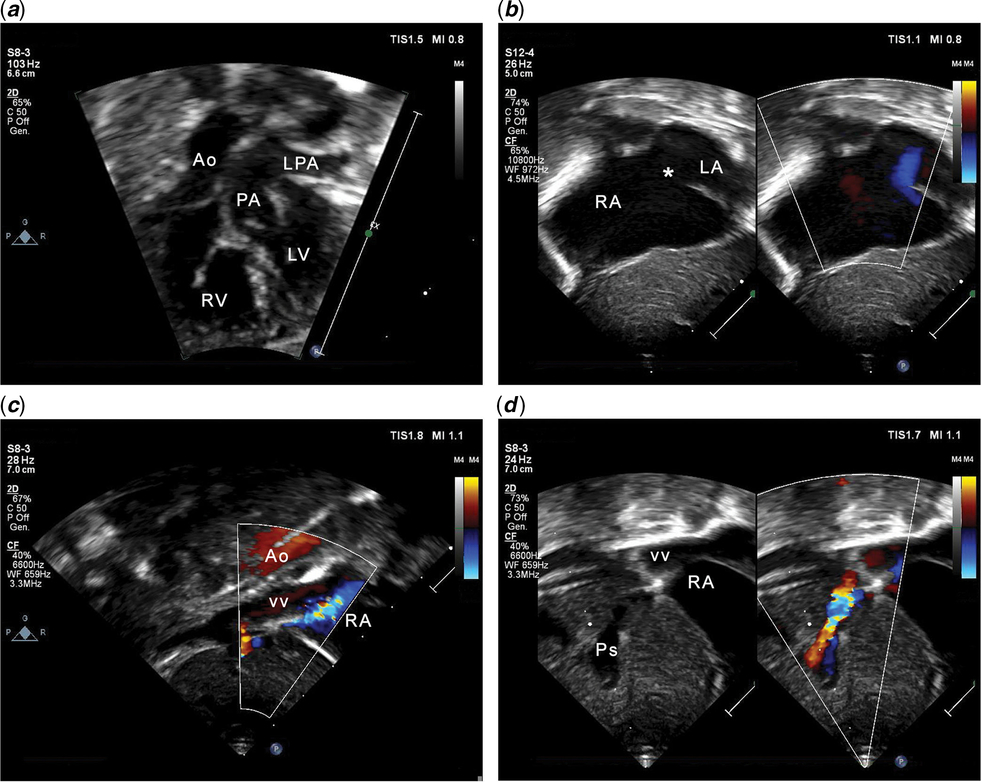
Figure 1. Echocardiographic 2D images. (a) In this subxiphoid view, D-transposition of the great arteries with intact ventricular septum is clearly demonstrated. (b) There is a large secundum atrial septal defect (asterisk) with right-to-left shunt. RA is enlarged. (c) Subxiphoid short-axis imaging with colour Doppler mapping shows a large vertical vein coursing inferiorly from behind the heart through the diaphragm; this is anterior to the aorta (Ao). Flow is towards the probe (red) in both vessels. (d) Colour aliasing indicates an obstruction of the vertical vein at the site of entry into the PS, which is dilated. Ao = aorta; LPA = left pulmonary artery; LV = left ventricle; PA = pulmonary artery; PS = portal sinus; RA = right atrium; RV = right ventricle; VV = vertical vein.
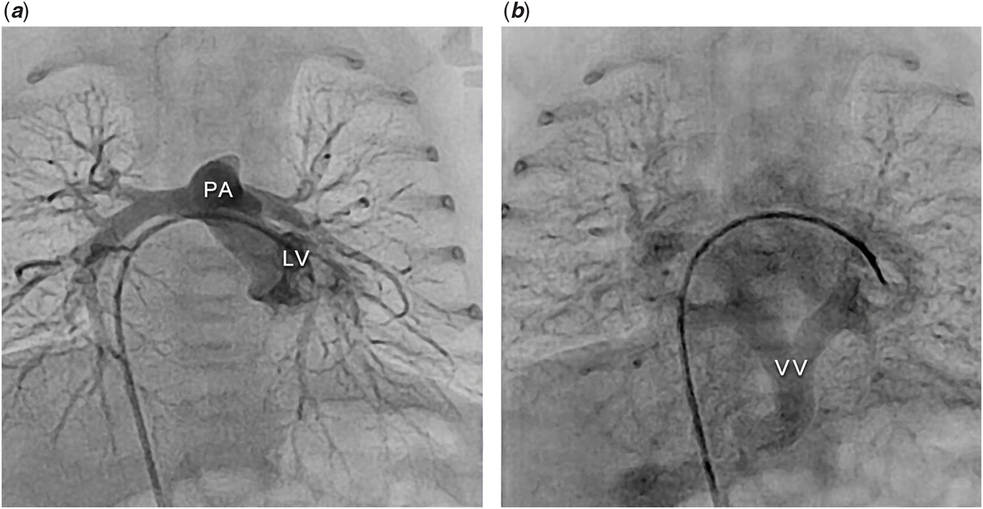
Figure 2. Cardiac catheterisation. Catheter course: femoral vein – inferior vena cava – right atrium – left atrium – left ventricle. (a) The left ventricular angiogram shows an intact ventricular septum and the PA arising from the LV, thus demonstrating the D-transposition of the great arteries. (b) Levophase of the LV angiogram showing all pulmonary veins draining into a large VV, with an inferior course through the diaphragm and a restrictive connection to the portal sinus. LV=left ventricle; PA=pulmonary artery; VV=vertical vein.



