



Healthcare-associated invasive mold infections (HA-IMIs), including invasive aspergillosis and mucormycosis, cause devastating morbidity and mortality. Reference Vonberg and Gastmeier1,Reference Novosad, Vasquez and Nambiar2 Previous HA-IMI clusters have been associated with various mold sources, including construction, water leaks, and air filtration issues. Reference Vonberg and Gastmeier1,Reference Hartnett, Jackson and Perkins3 Although considered uncommon, the incidence of HA-IMIs in the United States is unknown. Surveillance for these infections is challenging because of difficulties in ascertaining infection sources and the lack of a standardized case definition. The most widely accepted IMI case definition, developed by the European Organization for Research and Treatment of Cancer and the Mycoses Study Group (EORTC/MSG), is complex and excludes certain types of infections relevant to the healthcare setting, namely, cutaneous and wound infections. Reference Donnelly, Chen and Kauffman4 Hospitals have employed environmental air sampling techniques as a tool in HA-IMI cluster investigations and prevention efforts, but the optimal approach to analysis and interpretation of such sampling is unknown. Reference Hung, Caufield and Miller5 To gauge current practices regarding hospital HA-IMI surveillance and environmental air sampling, we surveyed members of the Society for Healthcare Epidemiology of America (SHEA) Research Network (SRN).
Methods
The SRN is a consortium of healthcare facilities collaborating on multicenter healthcare epidemiology research projects. On June 29, 2020, a cross-sectional survey was electronically distributed to eligible facilities, defined as US acute-care hospitals participating in SRN. 6 In total, 5 e-mail reminders were sent, and the survey was closed on September 3, 2020. The survey was reviewed by SRN Review and Research Committee, formatted on Survey Gizmo, and distributed by e-mail to site primary investigators. We summarized the survey responses regarding HA-IMI surveillance practices, air sampling approaches, and existing collaborations among HA-IMI prevention stakeholders. Using Fisher exact tests for proportions, we compared responses between academic and nonacademic hospitals; we considered P-values <.05 statistically significant. This activity was reviewed by the CDC and was conducted consistent with applicable federal law and CDC policy (see eg, 45 CFR part 46, 21 CFR part 56; 42 USC §241(d); 5 USC §552a; 44 USC §3501 et seq).
Results
Among 71 eligible facilities, 37 (52.1%) completed the survey. Most survey respondents were from academic medical centers (n = 25, 67.6%) and reported the presence of an intensive care unit (n = 35, 94.6%), a hematology-oncology unit (n = 30, 81.1%), and a stem cell transplant program (n = 24, 64.9%) (Supplementary Table 1 online).
Table 1. Surveillance for Healthcare-associated Invasive Mold Infections at Society for Healthcare Epidemiology of America (SHEA) Research Network Acute Care Hospitals (N = 35) a — United States, 2020

Note. EORTC/MSG, European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group.
a 2 hospitals that did not perform monitoring for healthcare-associated invasive mold infections were excluded from this table.
Overall, 35 (94.6%) of 37 hospitals performed any surveillance for HA-IMIs, either prospectively (n = 24, 68.6%) or retrospectively (n = 11, 31.4%) during a suspected IMI cluster (Table 1). Academic hospitals (n = 20, 83.3%) were more likely than were nonacademic hospitals (n = 4, 36.4%) to perform prospective monitoring for HA-IMIs (P = .02) and to have investigated an IMI cluster during 2018–2019 (n = 12 [50.0%] vs 1 [9.1%]; P = .03).
The most commonly used IMI case definition was EORTC/MSG (n = 15, 42.9%); 12 hospitals (34.3%) reported using a custom case definition developed in-house and 8 hospitals (22.9%) did not specify an IMI definition. Among facilities using a custom case definition, notable responses included a case-by-case approach based on clinical features (n = 7) and a definition based on test results (eg, culture, histopathology) (n = 2) regardless of clinical correlation. Regarding determination of whether IMIs were healthcare-associated, facilities mentioned time frames (difference between admission date to illness onset date) ranging from 2 days to >2 weeks. One hospital reported that determination of whether an IMI was hospital-associated might depend on the results of environmental samples or presence of recent construction activity.
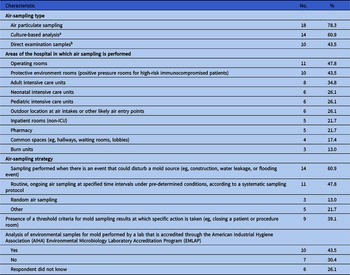
Overall, 23 (62.2%) hospitals reported performing any type of air sampling for mold (Table 2). Hospitals most commonly performed air sampling in operating rooms (n = 11, 47.8%) and protective environment rooms (n = 10, 43.5%). Approximately half (n = 11, 47.8%) of hospitals with air sampling reported performing routine, ongoing air sampling at specified time intervals under predetermined conditions using a systematic sampling protocol. Most hospitals (n = 30, 81.1%) reported access to industrial hygienist consultation and the presence of a project risk team (n = 31, 83.8%) to review proposed maintenance, renovation, and construction activities that pose an increased risk of generating or releasing microbial contamination (Supplementary Table 2 online).
Table 2. Practices Regarding Air Sampling for Mold Among Society for Healthcare Epidemiology of America (SHEA) Research Network Acute-Care Hospitals (n = 23)—United States, 2020

a Culture-based analysis (commonly referred to as “viable mold sampling.” Common samplers for this technique include Andersen N6, SAS Super 180, SKC BioStage and Buck BioAire).
b Direct examination samples are commonly referred to as “nonviable sampling,” “spore trapping,” or “total spore count.” These samples are usually collected using an inertial impactor with air sampling cassettes such as Air-O-Cell, Allergenco-D and Cyclex-D).
Discussion
In our survey of US SRN acute-care hospitals, most facilities performed prospective HA-IMI surveillance (69%) and most utilized air sampling for mold (62%) as part of HA-IMI prevention or investigation efforts. However, both HA-IMI case definitions and approaches to environmental sampling for mold varied substantially among facilities. The relatively high percentage of participants engaged in HA-IMI surveillance likely reflects that respondents were mostly from academic institutions caring for patient populations at high risk for IMIs (eg, patients with hematologic malignancies or receiving stem cell transplants). This finding is consistent with guidelines from the Infectious Diseases Society of America, which strongly recommend that leukemia and transplant centers surveil for cases of invasive mold infection. Reference Patterson, Thompson and Denning7
Facilities differed in both how IMIs were defined and how they were determined to be healthcare-associated, mirroring the diversity of case definitions that have been applied in previous HA-IMI cluster investigations. Reference Hartnett, Jackson and Perkins3 Ascertaining whether IMI cases are healthcare-associated is difficult because patients who develop IMIs often have complicated medical histories with multiple possible exposures and the incubation periods for some mold infections are not well established. Reference Hartnett, Jackson and Perkins3 Furthermore, certain hospitals may lack the laboratory capacity for prompt mold species identification. Despite these challenges, systematic surveillance for HA-IMIs is a necessary step in understanding disease burden, quickly identifying potential clusters, and reducing mortality from these infections; therefore, efforts to develop a feasible HA-IMI surveillance approach, including a standardized HA-IMI case definition, should be prioritized.
Hospitals varied substantially regarding whether and how they performed air sampling for mold, reflecting the controversial role of air sampling in preventing HA-IMIs. During previous HA-IMI clusters, air sampling has been helpful in identifying potential targets for remediation or supporting possible epidemiologic links between a mold sources and affected patients. Reference Hartnett, Jackson and Perkins3 For such investigations, air sampling is most useful when performed as an adjunct to a detailed environmental assessment and epidemiologic investigation using a well-designed sampling plan, optimally under the guidance of an industrial hygienist with experience participating in microbiological assessments. Reference Hartnett, Jackson and Perkins3 Air sampling may also be useful for monitoring mold counts before, during, and after major construction activities, a practice recommended by guidelines in several countries, Reference Talento, Fitzgerald, Redington, O’Sullivan, Fenelon and Rogers8,9 but it is not currently recommended by the US Healthcare Infection Control Practices Advisory Committee. Reference Sehulster and Chinn10 The utility of environmental air sampling may be limited by the lack of established threshold values or regulatory levels for mold in air and the lack of widely accepted industry qualification or practice standards for mold assessors and remediators. Reference Hung, Caufield and Miller5 Efforts to identify and close knowledge gaps regarding air sampling strategies for mold are needed; in the interim, consensus guidelines based on expert opinion and existing literature might empower acute care facilities to adopt rational approaches to air sampling for mold.
Our findings are limited by our inability to follow up with respondents and our small sample size. The HA-IMI surveillance and air sampling practices reported by the facilities surveyed might not represent practices of acute care hospitals nationwide. We suspect that facilities with interest or prior experience in HA-IMI prevention were more likely to respond to our survey and that HA-IMI surveillance and air sampling for mold may be less common in other hospitals. Nonetheless, our findings underscore the need to develop generalizable strategies for HA-IMI surveillance and for further data to guide rational approaches to air sampling for mold.
Acknowledgments
We are grateful to Valerie M. Deloney, MBA, for her contributions to survey design and assistance with survey dissemination. The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the US Department of Health and Human Services, the Public Health Service, or the Centers for Disease Control and Prevention. Use of trade names and commercial sources is for identification only and does not imply endorsement by the US Department of Health and Human Services or the US Centers for Disease Control and Prevention.
Financial support
The SHEA Research Network survey was conducted with funding provided by the Centers for Disease Control and Prevention.
Conflicts of interest
The authors have no potential conflicts of interest to disclose.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2021.285




 Open access
Open access