



Introduction
In England, one in six adults are estimated to have a common mental disorder (CMD) (McManus, Bebbington, Jenkins, & Brugha, Reference McManus, Bebbington, Jenkins and Brugha2016) such as depression or an anxiety disorder. Improving the mental health of the nation continues to be a priority for the UK Government and the National Health Service (NHS) (NHS England, 2019). Launched in 2008, the Improving Access to Psychological Therapies (IAPT) programme offers adults in England evidence-based talking therapies for CMDs. By 2017, nearly 1 million patients were seen by services per year (Clark, Reference Clark2018). However, for such services to achieve their aim in improving the mental health of the national, equality in access across patient groups is needed. This is especially important given that the burden of CMDs disproportionally affects those from vulnerable backgrounds and lower socio-economic backgrounds, such as ethnic minority groups, disabled people, migrants, people living in deprived areas or those with low educational attainment (Fryers, Melzer, Jenkins, & Brugha, Reference Fryers, Melzer, Jenkins and Brugha2005; NHS England, 2016; Nunes et al., Reference Nunes, Pinheiro, Bessel, Brunoni, Kemp, Benseñor and Schmidt2016).
Previous research from a range of mental healthcare settings suggests there exists inequalities in access. For example, individuals for minoritised ethnicities have been found to be less likely to receive support from mental health services than those from White groups (Simpson, Krishnan, Kunik, & Ruiz, Reference Simpson, Krishnan, Kunik and Ruiz2007; Van Voorhees, Walters, Prochaska, & Quinn, Reference Van Voorhees, Walters, Prochaska and Quinn2007) and older adults have been identified as particularly disadvantaged, at least historically (Department of Health, 2001). Other factors such as language barriers (Dixon-Woods et al., Reference Dixon-Woods, Kirk, Agarwal, Annandale, Arthur, Harvey and Sutton2005), religious involvement (Harris, Edlund, & Larson, Reference Harris, Edlund and Larson2006) and level of educational qualification (Weich, Nazareth, Morgan, & King, Reference Weich, Nazareth, Morgan and King2007) have also been associated with differential access to mental health treatments. However, there has been limited research into inequalities in access to IAPT services, with existing evidence provided by a handful of services indicating that there are some local level inequalities in access. For example, individuals from minority ethnic groups are less likely to be assessed and treated in IAPT, compared to White British individuals (Ahmad, McManus, Cooper, Hatch, & Das-Munshi, Reference Ahmad, McManus, Cooper, Hatch and Das-Munshi2022; Harwood et al., Reference Harwood, Rhead, Chui, Bakolis, Connor, Gazard and Hatch2021). Recent analysis of male users from two services in London suggests ethnicity, religious affiliation and socio-economic status are associated with service use (Smyth et al., Reference Smyth, Buckman, Naqvi, Aguirre, Cardoso, Pilling and Saunders2022). However, this has not been explored at the national level. One limitation with using data from IAPT services for such analyses is that some socio-demographic characteristics, such as age, sex, disability, ethnicity, and religion, are collected at the point of registration, but the proportion of valid responses provided nationally are low for some characteristics [ethnicity; 86.5%, religion; 63.9% (NHS Digital, 2018)]. Additionally, several characteristics which may impact mental health or access to services, are not collected during the IAPT registration (e.g. individual measures of socio-economic status). Estimating rate of access to IAPT by socio-demographic characteristics is difficult because of the lack of suitable population data. Finally, to date there has been no attempt to understand how representative the IAPT population is compared to the general population with CMDs. Identifying groups with lower relative access to IAPT could help identify subgroups currently underrepresented in IAPT and support targeted outreach initiatives.
In this study, we examined the socio-demographic characteristics of individuals treated nationally in the IAPT programme and whether participants were representative of the population experiencing CMDs in England. Using a unique individual patient dataset that linked 2011 Census information of English residents to data from all patients seen by the national IAPT programme, we estimated the rate of access by a wide range of socio-demographic characteristics. Using data from a large household survey, we estimated the prevalence of probable CMDs by socio-demographic characteristics. To identify groups which had lower access to IAPT, we estimated the probability of access amongst people with CMDs by comparing the rates of access to IAPT and the estimates of prevalence of CMDs.
Methods
Data and participants
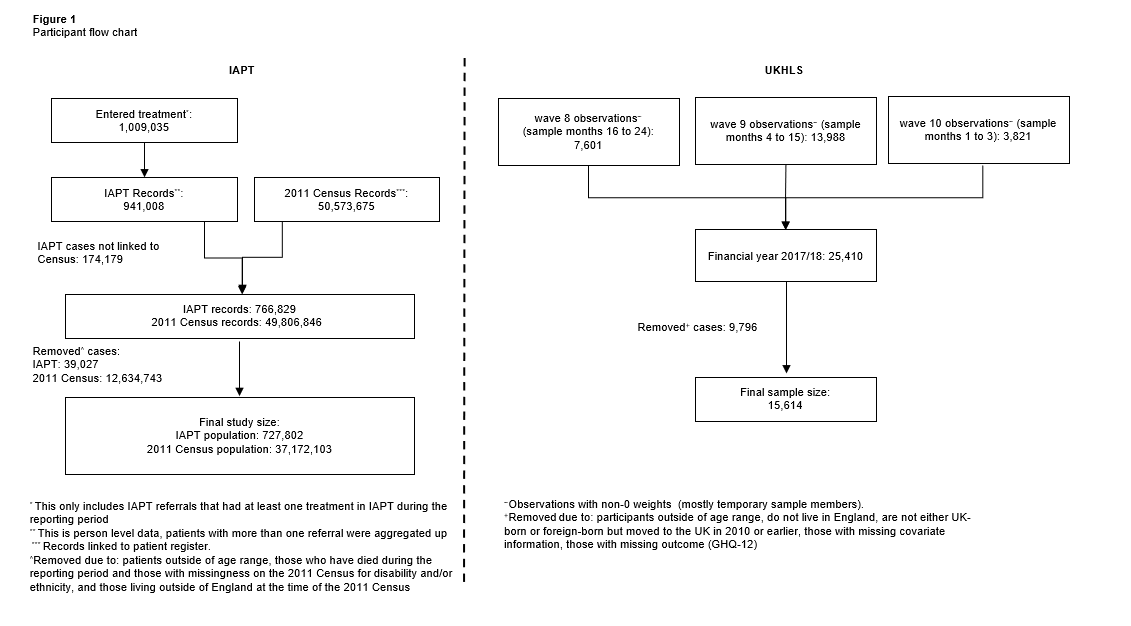
We conducted a retrospective cohort study using a unique dataset based on the 2011 Census linked to nationally collected IAPT data and comparing it to data from the UK Household Longitudinal Study (UKHLS) (University of Essex: Institute for Social and Economic Research, 2022). The census for England and Wales is a survey collected every 10 years by Office for National Statistics which provides in-depth information on all people and households in England and Wales (Office for National Statistics, 2022). All IAPT services, which operate across all regions of England, collect the same standardised minimum dataset (the IAPT MDS) and provide monthly submissions of this data to NHS Digital where it is compiled for both monthly and annual reports (John et al., Reference John, Saunders, Desai, Bell, Fearn, Buckman and Stott2022). For the current analysis the IAPT national data for the financial year 2017/18 was used, including all participants who had at least one treatment session as determined by the ‘APPTYPE’ (Appointment type) variable. For this study, we focused on the 2017/18 financial year, the most recent year for which national data were available to the research team and provided by NHS Digital (data owners) for analysis purposes via the Data Access Request Service.
The linkage of IAPT data to the 2011 Census for England and Wales was conducted using NHS number. To obtain NHS numbers for census participants, the 2011 information was linked to the 2011–2013 NHS Patient Registers. Of the 53 483 502 census records, 50 019 451 were linked deterministically to the patient register. 555 291 additional matches were obtained using probabilistic matching (overall linkage rate of Census to NHS Patient Register: 94.6%). The cohort was also linked to death registration data using NHS number, to remove participants who died during the reporting periods. Study participants are the adult population in England aged 18 (at the start of the reporting period) to 100 years, who were usual residents in England when they were enumerated in the 2011 Census. Participants living in Wales at the time of 2011 Census were excluded from the study.
Out of the 1 009 035 IAPT referrals received within the 2017/18 reporting period, we identified 941 008 unique patients. Out of the 941 008 individuals, 766 829 (81.5%) were successfully linked to the 2011 Census (online Supplementary Fig. S1).
We used data from UKHLS waves 8 to 10, to measure probable CMDs within the population at an equivalent time to the IAPT data. The UKHLS data was accessed via the UK Data Archive with addition of lower super output area information requested through the special licence. Interviews for which sample months were between April 2017 and March 2018 were pooled into a financial year 2017/18 dataset equivalent to the IAPT reporting period. Survey weights were scaled to adjust for reduced likelihood to respond over time following UKLHS guidance (Kaminska & Lynn, Reference Kaminska and Lynn2019). The UKHLS includes a representative UK sample with a total sample size of between 50 994 (wave 1) and 34 318 (wave 10) participants per wave. Study participants from the UKHLS were the adult population in England (per financial year) aged 18 to 100 years who were living in the UK in 2011 who responded to the survey. Of the 19 135 respondents meeting the study criteria 3410 were removed because of missing covariate information and a further 111 because of missing outcome. Inverse probability weighting was used to adjust for selection bias due to this item missingness. Sociodemographic characteristics of UKHLS were used from the interview provided closest to March 2011 to match information from census as closely as possible.
Variables
Our exposures of interest were socio-demographic characteristics potentially related to CMDs or access to healthcare. The burden of CMDs disproportionally affects those from vulnerable backgrounds and lower socio-economic backgrounds, such as ethnic minority groups, disabled people, migrants, people living in deprived areas, those with lower educational attainment (Das-Munshi, Leavey, Stansfeld, & Prince, Reference Das-Munshi, Leavey, Stansfeld and Prince2012; Esch et al., Reference Esch, Bocquet, Pull, Couffignal, Lehnert, Graas and Ansseau2014; Fone et al., Reference Fone, White, Farewell, Kelly, John, Lloyd and Dunstan2014; Fryers et al., Reference Fryers, Melzer, Jenkins and Brugha2005; Mercer & Watt, Reference Mercer and Watt2007; Naylor et al., Reference Naylor, Parsonage, Mcdaid, Knapp, Fossey and Galea2012; NHS England, 2016; Nunes et al., Reference Nunes, Pinheiro, Bessel, Brunoni, Kemp, Benseñor and Schmidt2016). Whilst religion may offer some comfort with those with mental health problems (King, Weich, Nazroo, & Blizard, Reference King, Weich, Nazroo and Blizard2006; McCullough & Larson, Reference McCullough and Larson1999), some studies suggest religion can be a barrier affecting access to mental health services and psychological therapies (Loewenthal, Mohamed, Mukhopadhyay, Ganesh, & Thomas, Reference Loewenthal, Mohamed, Mukhopadhyay, Ganesh and Thomas2012).
All individual level socio-demographic characteristics for the access to IAPT analysis came from the 2011 Census data and include age, country of birth, disability status, English as first language, ethnicity, index of multiple deprivation (IMD), qualifications, region of England, religious affiliation, and sex (See online Supplementary Table S1). To estimate the prevalence in the general population, the socio-demographic characteristics came from the UKHLS interviews that were available closest to the 2011 Census date (±26 months) or the first adult interview for someone aged 16 years.
Outcome measures
For the analysis of access to IAPT, the main outcome was having received at least one treatment session in IAPT between April 2017 and March 2018.
For the analysis of the prevalence of CMDs using the UKHLS, the main outcome was having a General Health Questionnaire (GHQ)-12 score of 4+ using the standard scoring method to proxy probable CMD.
GHQ-12 is a validated measure that is commonly used to estimate non-psychotic psychiatric morbidity and CMDs (Brown, Harris, Srivastava, & Taylor, Reference Brown, Harris, Srivastava and Taylor2018; Endsley, Weobong, & Nadkarni, Reference Endsley, Weobong and Nadkarni2017; Stochl, Böhnke, Pickett, & Croudace, Reference Stochl, Böhnke, Pickett and Croudace2016). GHQ-12 has been validated against ICD-10 diagnoses (current depression, dysthymia, agoraphobia, panic disorder, generalised anxiety disorder, somatisation disorder, neurasthenia and hypochondriasis) that have large overlap with those covered by IAPT and which has been shown to be as effective as longer screening instruments for mental health for identifying CMDs (Goldberg et al., Reference Goldberg, Gater, Sartorius, Ustun, Piccinelli, Gureje and Rutter1997).
We then compare the two set of rates to estimate the proportion of individuals with CMD who received treatment in IAPT.
Statistical methods
Descriptive statistics for all variables were calculated in both IAPT and UKHLS cohorts. Data is presented as counts and percentages.
Adjusted rates of the respective outcome measures were derived by calculating marginal probabilities from logistic regression models. For each exposure, we fitted logistic regression models to estimate the probability of receiving treatment (IAPT) and of having a CMD (UKHLS, survey weighted). We fitted unadjusted models and models adjusted for all other exposures using our 18+ population. We restricted the population to individuals aged 25+ when estimating the effects of qualifications and National Statistics Socio-Economic Classification (NS-SEC) to minimise the influence of measurement error between the Census and IAPT time points.
In the UKHLS sample, we used analysis weights for the self-completion questionnaire to adjust for differences in selection probabilities and non-response. We deleted observations with missing data and used inverse probability weighting based on a logistic regression model to account for non-randomness of the missing data.
We used an indirect method to estimate the access to IAPT amongst people with probable CMDs. We estimated the proportion of individuals with CMD who received treatment in IAPT, by dividing the rates of people receiving treatment through IAPT services by the self-reported CMD rates. If for a particular group, the rate of access to IAPT was 3%, and the self-reported CMD rate was 15%, then the rate of access to IAPT among people with probable CMDs was 20% (0.03/0.15). To obtain 95% confidence intervals, we ran a Monte Carlo simulation with one million iterations, drawing each rate from a normal distribution with a mean equal to the estimated rate and a standard deviation equal to the standard error and calculating the ratio. The 2.5th and 97.5th percentiles of the resulting distributions were used to estimate the 95% confidence intervals (Buckland, Reference Buckland1984).
All IAPT, 2011 Census and Mortality data were analysed in R version 3.5.1. All UKHLS data was analysed in STATA version 15.1. The comparison of IAPT to UKHLS was completed in R version 4.1.3.
Results
Study populations
The general Census 2011 population for this study was 37 899 905, of which 727 802 (1.9%) received at least one treatment session through IAPT services (around 1 in 50) in 2017/18. The UKHLS cohort comprised 15 614 participants of which 18.1% had a probable CMD.
Our study population (Table 1) were predominantly female (Census: 52.3%; UKHLS: 51.7%), with a mean age 49.8 (±18.6 years) in census and 51.3 years (±18.2 years) in UKHLS, born in the UK (Census: 85.7%; UKHLS: 89.9%), had English as their first language (Census: 92.4%; UKHLS: 94.0%) and White (Census: 87.5%; UKHLS: 91.07%).
Table 1. Socio-demographic characteristics of the study population

NS-SEC, National Statistics Socio-Economic Classification; IMD, Index of Multiple Deprivation.
a Using a 25 + population.
Main findings
The proportion of people with a CMD in UKHLS; the proportion of people accessing IAPT services; and those accessing IAPT as a proportion of those with a probable CMD broken down by socio-demographic characteristic can be found in Tables 2 and 3. Findings for qualifications and NS-SEC can be found in Table 4.
Table 2. Proportion of individuals with a probable Common Mental Disorder (CMD) defined by a score of 4 and above on the GHQ-12 (A) and proportion of individuals treated in Improving Access to Psychological Therapies (IAPT) (B) broken down by socio-demographic characteristics

CI, 95% confidence interval; IMD, Indices of Multiple Deprivation.
a This is the unadjusted model.
b Fully adjusted model; adjusted for age, country of birth, English as a first language, ethnicity, sex, IMD (quintile), region, religious affiliation, and disability status.
Table 3. Estimated proportion of individuals with a probable Common Mental Disorder (CMD) that receive treatment in Improving Access to Psychological Therapies (IAPT) broken down by socio-demographic characteristics

CI, 95% confidence interval; IMD, Indices of Multiple Deprivation.
a This is the unadjusted model.
b Fully adjusted model; adjusted for age, country of birth, English as a first language, ethnicity, sex, IMD (quintile), region, religious affiliation, and disability status.
Table 4. NS-SEC and Qualifications (25+ model) showing the proportions of people; with probable common mental disorder (CMD), accessing Improving Access to Psychological Therapies (IAPT) and the comparison

NS-SEC, National Statistics Socio-Economic Classification; LCI, Lower Confidence Interval; UCI, Upper Confidence Interval.
a Unadjusted model.
b Fully adjusted model; adjusted for age, country of birth, English as a first language, ethnicity, sex, Index of Multiple Deprivation (quintiles), region, religious affiliation, disability status, qualifications and NS-SEC.
Age and sex
Adults aged 25- to 34-years were most likely to have a probable CMD [23.2% (95% CI 20.1–26.3%)) and this declined with age. Similarly, among all individuals in IAPT, treatment rates decreased with age with only 0.7% (95% CI 0.6–0.7%) of adults aged 65- to 100-years old receiving treatment. Among those with probable CMDs, 18- to 24-year-olds were most likely to access IAPT [14.2% (95% CI 12.0–17.5%)] and adults 65 and over least likely to access IAPT [4.7% (95% CI 4.3–5.1%)]. Adjusting for other factors had little effect on the estimated differences in access to IAPT by age and sex.
Males were less likely to have a probable CMD [15.9% (95% CI 14.7–17.1%)] and to receive treatment through IAPT [1.4% (95% CI 1.3–1.4%)]. There is a statistically significant underrepresentation of males in IAPT with only 8.5% (95% CI 7.9–9.2%) of males with CMD entering this service compared to 10.8% (95% CI 10.3–11.4%) of females. When adjusting for other factors the difference reduced slightly but remained significant.
Ethnicity, country of birth, English as a first language and religion
The Mixed ethnic group had the highest proportion of probable CMDs [30.4% (95% CI 21.9–38.8%)] when comparing against the other ethnic groups (range 14.1 to 21.8%). They were also most likely to be receiving treatment in IAPT [2.9% (95% CI 2.8–3.1%)]. When estimating the proportion of individuals with CMD who received treatment in IAPT, 9.7% (95% CI 7.6–13.5%) of the Mixed ethnic group received treatment compared to 10.2% (95% CI 9.7–10.7%) of the White ethnic group. The Asian ethnic group [7.2% (95% CI 6.2–8.7%)] were significantly underrepresented in IAPT when compared to the White ethnic group. Adjusting for other factors reduced the differences, but the Asian ethnic group remained significantly underrepresented in IAPT compared to the White ethnic group.
Those born in the UK were (non-significantly) more likely to have a probable CMD over those born outside of the UK [19.6% (95% CI 18.7–20.6%) compared to 17.0% (95% CI 14.6–19.4%)]. However, those born outside the UK were significantly less likely to receive treatment in IAPT [1.2% (95% CI 1.2–1.3%)] compared to 2.0% (95% CI 2.0–2.0%) and consequently only 7.2% (95% CI 6.3–8.4%) of those with probable CMD received treatment in IAPT compared with 10.4% (95%CI 9.9–10.9%) of UK born patients. This difference reduced but remained significant when adjusted for other factors.
CMDs affected 19.6% (95% CI 18.7–20.5%) of people whose first language was English compared to 15.4% (95% CI 12.7–18.1%) of people for who English was not their first language. Also, there was a higher proportion of patients receiving treatment in IAPT where English was their first language [2.0% (95% CI 2.0–2.0%) compared to 1.1% (95% CI 1.0–1.1%)] where English was not their first language. When comparing there was a significant difference in representation with those where English is not the first language being underrepresented [6.9% (95% CI 5.9–8.4%)] compared to those where English was the first language [10.1% (95% CI 9.7–10.6%)]. Adjusting for other factors made this difference non-significant.
There was no difference in the proportion of people with a probable CMD by religious affiliation [no religion: 19.6% (95% CI 18.4–20.9%); any religion affiliation: 19.1% (95% CI 18.0–20.3%)]. People with no religion were significantly more likely to be treated in IAPT [2.4% (95% CI 2.4–2.5%) compared to 1.7% (95% CI 1.7–1.8%)]. Those with a religious affiliation and probable CMD were significantly underrepresented in IAPT [9.1% (95% CI 8.6–9.7%) compared with 12.4% (95% CI 11.6–13.3%)]. Adjusting for other factors reduced the difference, but having a religious affiliation remained significantly associated with being underrepresented in IAPT.
Disability status
Disabled people had higher levels of probable CMD [31.6% (95% CI 29.5–33.8%)] compared to those who were not disabled [16.4% (95%CI 15.5–17.3%)] and there was a higher proportion of disabled people receiving treatment in IAPT [2.2% (95% CI 2.1–2.2%) compared to 1.9% (95% CI 1.9–1.9%)]. However, only 6.8% (95% CI 6.4–7.3%) of disabled people with a probable CMD are being treated in IAPT compared with 11.5% (95%CI 10.8–12.1%) of non-disabled people, indicating disabled people are significantly underrepresented in IAPT. After adjustment, these differences were attenuated but remained significant, suggesting having a disability is negatively associated with access to IAPT.
Highest qualification (sample age 25+)
Having no academic or professional qualifications was associated with a higher level of probable CMDs [20.1% (95% CI 17.0–23.3%)] compared to below a degree qualification [19.1% (95% CI 17.8–20.4%)] and degree level and above [16.9% (95%CI 15.5–18.2%)] (Table 4). Despite this, the no qualifications group were least likely to be treated in IAPT [1.3% (95% CI 1.2–1.3%)] and this was significantly different to those with any other qualifications [below a degree level; 2.0% (95% CI 2.0–2.0%), degree level and above; 1.7% (95% CI 1.7–1.8%)]. They were also significantly underrepresented in IAPT as a proportion of those with probable CMD [6.3% (95% CI 5.4–7.4%)] compared to 10.3% (95% CI 9.7–11.1%) for those with a below a degree level qualification and 10.3% (95% CI 9.5–11.2%) of those with a degree level and above. After adjustment, this difference reduced but remained significant.
Additional analyses
Further analyses on local area deprivation, region and NS-SEC can be found in Tables 2, 3 and 4. There was little difference in IAPT treatment rates among those with a probable CMD by IMD (range 9.7–10.2%) with those in IMD category 2 (1 being most deprived) most represented in IAPT [IMD 2: 10.2% (95% CI 9.3–11.4)]. The biggest difference between regions was between the West Midlands [8.4% (95% CI 7.4–9.6)] and the North East [11.6% (95% CI 9.6–14.6)].
Discussion
This study found that older adults, males, people born outside of the UK, people with a religious affiliation, people from Asian ethnic backgrounds, people with a disability and those without any academic or professional qualifications appear underrepresented in IAPT as a proportion of those with a probable CMD.
Research acknowledges that older adults are underrepresented in mental health treatment (Department of Health, 2001), including IAPT (Clark, Reference Clark2018) despite evidence that they may have better outcomes in IAPT than working age adults (NHS Digital, 2022; Saunders et al., Reference Saunders, Buckman, Stott, Leibowitz, Aguirre, John and Pilling2021), and this is supported by the results of this study. Having a disability was also associated with reduced access to IAPT. The prevalence of CMDs is higher in those with a disability and this supports previous research demonstrating that people with disabilities are at a higher risk of experiencing poor mental health (NHS England, 2016), although it is important to note that for many individuals' mental ill-health itself can be classified as a disability. The IAPT programme has expanded to offer integrated services which provide treatment for CMDs in individuals with long term physical health conditions, which go some way to addressing the treatment gap for those with disabilities (Clark, Reference Clark2018).Targeted programmes within IAPT which help those with long term conditions have been effective at reducing depression and anxiety (Toffolutti et al., Reference Toffolutti, Stuckler, McKee, Wolsey, Chapman, J Pimm and M Clark2021).
Men are less likely to seek support than women for their mental health (Bogdanova, Cooper, Ahmad, McManus, & Shoham, Reference Bogdanova, Cooper, Ahmad, McManus and Shoham2022) despite evidence that men are much more likely to take their own life (Office for National Statistics, 2021; Vogel, Wade, & Haake, Reference Vogel, Wade and Haake2006). The differences in access in IAPT are consistent with this existing research. Increasing engagement with men may help to reduce poorer outcomes. This outreach should be targeted to ensure there are greater numbers of referrals for men, and barriers need to be broken down to encourage men to seek this support when needed.
Research reports that marginalised groups are at higher risk of poorer mental health (Nyashanu, Ganga, & Chenneville, Reference Nyashanu, Ganga and Chenneville2022) as they are more likely to experience downward social mobility due to racism, discrimination, language barriers or lack of cultural knowledge (Das-Munshi et al., Reference Das-Munshi, Leavey, Stansfeld and Prince2012). Studies also report that mental health services continue to be inaccessible for these groups (Das-Munshi et al., Reference Das-Munshi, Leavey, Stansfeld and Prince2012). Research has found that individuals from ethnic minority backgrounds are less likely to consult GPs for CMDs and when they do, they are less likely to be diagnosed (Bogdanova et al., Reference Bogdanova, Cooper, Ahmad, McManus and Shoham2022; Cooper et al., Reference Cooper, Spiers, Livingston, Jenkins, Meltzer, Brugha and Bebbington2013). Evidence suggests that minority groups are more likely to be referred to IAPT via secondary care routes and are less likely to self-refer to the service, showing differences in health seeking behaviours (Harwood et al., Reference Harwood, Rhead, Chui, Bakolis, Connor, Gazard and Hatch2021). Recent research using the 2007 and 2014 APMS data also shows treatment inequalities are widening over time by ethnic group (Ahmad et al., Reference Ahmad, McManus, Cooper, Hatch and Das-Munshi2022).
There was a significant underrepresentation of those born outside of the UK compared to those born in the UK in IAPT, confirming previous research suggesting that migrants are likely to be disadvantaged regarding access to support for mental health issues (Bhavsar et al., Reference Bhavsar, Jannesari, McGuire, MacCabe, Das-Munshi, Bhugra and Hatch2021; Das-Munshi et al., Reference Das-Munshi, Leavey, Stansfeld and Prince2012). Despite this, not having English as a first language was not identified as a significant barrier to accessing IAPT services. Given research has indicated language barriers can impact access to mental health treatment (Scheppers, van Dongen, Dekker, Geertzen, & Dekker, Reference Scheppers, van Dongen, Dekker, Geertzen and Dekker2006), this finding may highlight some positive actions taken by IAPT services to increase accessibility. For example, the IAPT manual has several initiatives such as bilingual clinicians and producing leaflets and information in community languages (Harwood et al., Reference Harwood, Rhead, Chui, Bakolis, Connor, Gazard and Hatch2021) which may partly explain this finding. For ethnic minority groups, migrants and those where English is not their first language further research is needed to understand the barriers to treatment that these groups face, which might inform policies to improve access for these groups.
Religion can be an important factor affecting attitudes to accessing support for mental health (Loewenthal et al., Reference Loewenthal, Mohamed, Mukhopadhyay, Ganesh and Thomas2012). Religious people often feel that the significance of their beliefs are not understood by mental health professionals (McCullough & Larson, Reference McCullough and Larson1999), despite evidence that religious and faith-based adaptions to psychological therapy might improve outcomes (Arundell, Barnett, Buckman, Saunders, & Pilling, Reference Arundell, Barnett, Buckman, Saunders and Pilling2021). Some groups and communities still stigmatise mental illness, seeing it as a punishment and fearing discrimination from their community, meaning they may opt for spiritual treatments (Yu, Yang, Yu, & Liu, Reference Yu, Yang, Yu and Liu2022). Despite research suggesting that religious involvement could provide a sense of belonging and spirituality and consequently benefits to mental health (King et al., Reference King, Weich, Nazroo and Blizard2006; McCullough & Larson, Reference McCullough and Larson1999), in this study, there was no difference in the proportion of people with CMDs between those with and without religious affiliation.
Previous research has identified complex relationships between school experiences, educational qualifications and mental health problems (Esch et al., Reference Esch, Bocquet, Pull, Couffignal, Lehnert, Graas and Ansseau2014; Fergusson, McLeod, & Horwood, Reference Fergusson, McLeod and Horwood2015).This is reflected in the proportion of CMDs experienced by those without any academic and professional qualifications, yet this group were also less represented in IAPT treatment. There is little research into the potential barriers in access for individuals with lower educational attainment but efforts to better understand such factors might help services improve access for these individuals.
Lastly, although the self-referral model has been designed to improve the overall access to IAPT, studies have found that the self-referral process can be overwhelming and act as a barrier in access for certain socio-demographics (Thomas et al., Reference Thomas, Hansford, Ford, Wyatt, McCabe and Byng2020). Individuals who are aware of mental health services in England, have access to internet-enabled devices and are confident in using these devices could be more likely to self-refer than others. Therefore, it could be argued the self-referral option could lead to increased inequalities in access between groups.
Strengths and limitations
This study benefitted from a unique dataset linking the 2011 Census to national IAPT data. Unlike studies solely based on sample frames, we generated high-quality population-based information with large sample size and high data coverage. Data collected by UKHLS provided large representative sample of the English population with a probable CMD which increased validity of the findings. This study used a validated and reliable measure to identify probable CMDs.
The 2017/18 IAPT dataset was used for the analysis, and therefore findings may not reflect the current representation in IAPT which showed relative increases in referrals that started treatment across all socio-demographic groups (NHS Digital, 2022). Similarly, some 2011 Census variables particularly qualifications may have changed in between the census and IAPT access. Future research should look at later years of data to compare changes in IAPT access over time.
Despite GHQ-12 being a reliable and commonly used measure, previous studies have questioned validity of GHQ-12 for identifying CMDs (Donath, Reference Donath2001). We used GHQ-12 as a proxy of CMDs, but not all individuals scoring 4+ are likely to require support for a CMD. It is also possible that people with serious mental illness, who should be referred to secondary mental health services rather than IAPT, might score 4+ on GHQ-12. Conversely, GHQ-12 might not capture well some conditions, such as obsessive-compulsive disorder and post-traumatic stress disorder, that are covered by IAPT. We also do not account for other services or potential treatments for CMDs like private care or medication which may reduce the need for IAPT. For that reason, we can only assess the uptake from IAPT, it is not possible to say if groups underrepresented in IAPT are more likely to receive other types of treatment instead. Further research combining different data sources to assess different treatments for CMDs combined would be desirable. Additionally, the anticipated access rates for the IAPT programme are typically based on results from the Adult Psychiatric Morbidity Survey (APMS) which uses the Clinical Interview Schedule Revised (CIS-R) to determine CMD prevalence rates in England which could result in discrepancies with the UKHLS.
Lastly, we only included individuals seen at least once in IAPT, meaning we evaluated the initial access to mental health services as an unmet need. This does not consider the quality and efficacy of the care they receive. Retention of patients, treatment length and outcomes should be evaluated to fully understand socio-demographic differences in access to mental health services. Due to data availability, we could not include or control for clinical severity scores, so future iterations of this study should incorporate these to provide a more accurate representation of people with probable CMD in IAPT.
Conclusions
This study aimed to identify the representativeness of the IAPT population amongst people with probable CMDs. The study found underrepresentation of several key groups including older adults, males, ethnic minority groups, those born outside of the UK and those with no academic or professional qualifications. Whilst these results are not necessarily unique to IAPT in the context of mental healthcare, they should inform future expansion of IAPT services targeting these groups to ensure they get equal treatment of their CMD. Future research should consider repeating the study with later years of IAPT and 2021 Census data, and consider to further explore the measure for probable CMD prevalence by comparing GHQ-12 to the more detailed CIS-R based on the next APMS survey. To address knowledge gaps, future research should also incorporate analysis looking at differences in treatment length, dropout rates and outcomes of patients who completed minimal treatment in IAPT. This will provide more accurate representation of people with CMDs in IAPT and greater understanding of the unmet need. Research should also incorporate patients' perspective of barriers to access to mental health services.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291723001010
Financial support
This project was funded by the Office for National Statistics.
Conflict of interest
The authors have consulted NHS England teams (IAPT data owners and IAPT programme leads) on key methodologies during the initial planning of the project. Besides this, there are no other conflicts of interest for all authors.







 Open access
Open access