



Despite Türkiye being at high risk for earthquakes, few could anticipate the destruction that the powerful 6 and 7 February 2023 earthquakes and the aftershocks would cause. As of 5 April 2023, the earthquakes have caused officially more than 50 000 deaths(1), the complete collapse of more than 139 000 buildings and many more injuries along with more than one million people being left homeless(2) in Türkiye. The numbers continued to increase after the initial earthquakes as additional tremors trapped people under the rubble(3). In Türkiye, the earthquake affected eleven provinces directly that have an estimated population of over 13·5 million(4). Earthquake zones experienced a halt to local food production, destruction of the power grid, disruption of the food supply chain and contaminated water systems, which created shortages in both potable water and water for personal hygiene(5).
Before the Türkiye–Syria earthquake (TSE), with the COVID-19 pandemic and the downturn in the Turkish economy, the population was already highly susceptible to food insecurity(6). The latest estimated national food insecurity was reported to be 16 % in 2017 according to the Türkiye Nutrition and Health Survey (TNHS)(7). However, vulnerable groups such as immigrants or low-income populations were documented to have a food insecurity prevalence of up to 60 %(7,Reference Büyüksoy, Çatıker and Özdil8) . In the FAO of the United Nations’ The State of Food Security and Nutrition in the World (SOFI) report, Türkiye with its Syrian refugees was listed among the twenty-two countries in a food crisis situation where conflict is the main driver of acute food insecurity(9). Türkiye has the highest number of asylum seekers in the world, with many subsisting on food and cash aid from different institutions(10).
While many suffer from undernutrition, chronic diseases related to overnutrition are also a concern in Türkiye. According to the National Statistical Institute of Türkiye, in 2021, 33·4 % of deaths in the country were from circulatory system diseases, 14 % from malign and benign neoplasms and 4·1 % died from endocrine system diseases(11). The country has the highest rates of obesity in Europe and increasing prevalence of CVD, diabetes and hypertension(12). The same recent economic factors that can exacerbate food insecurity for some can also exacerbate overnutrition for others; people were shown to consume unhealthy yet more affordable foods that were calorically dense(Reference Sakarya13). TNHS 2017 results showed that the consumption of vegetables and fruits was quite low since only 52·9 % of the population were found to consume vegetables every day, and for fruits, this frequency was 53·4 % of the population. These consumption levels were associated with suboptimal intake of vitamins D, B1, B2, B6 and folate along with minerals Zn, Mg and K. In addition, women were found to consume significantly less Fe compared with their daily requirements(7). TNHS 2017 was the last comprehensive and demographically representative country-wide nutrition and health survey. Since 2017, nutrition status is presumed to have worsened with the COVID-19 pandemic and the downturn in Turkish economy that followed it(Reference Kalyoncu Atasoy, Aslan and Ilgaz14). This nutritional context highlights the importance of robust emergency nutrition support in the aftermath of the TSE; many people dependent on this support had pre-existing nutritional deficiencies and needs.
In the wake of a natural disaster, emergency nutrition care is indispensable for sustaining the lives of victims and the rescue personnel(15). The two major food aid institutions in Türkiye are the Disaster and Emergency Management Presidency (AFAD), which is the main governmental disaster management agency operating under the Turkish Ministry of Interior, and the Turkish Red Crescent (KIZILAY)(Reference Ipek, Dikici and Topçu16). While AFAD is responsible for the whole rescue operation and the disaster management, KIZILAY is primarily responsible for providing emergency nutrition services and coordinating donations and other actors that could be present to provide food for the survivors of any natural or human-made disasters(Reference Doğru and Ede17,18) .
In 2017, KIZILAY prepared a comprehensive guide that detailed the optimum planning of emergency nutrition as part of disaster planning(19). The guide addresses issues observed in the nutrition response following the 1999 Izmit and 2002 Afyon earthquakes, when the biggest concerns were the availability of a limited range of food groups and lack of hygiene. Other issues observed included a lack of age-appropriate nutrition, limited availability of fruits and vegetables, inconsistent meal schedules in the tent cities, vitamin deficiencies, expired canned foods, improper storage, insufficient refrigerators, lack of hygiene in service personnel, wasted bread and dishwashing problems. In addition, baby food could not be used due to the lack of clean hot water and feeding bottles(20). According to the 2017 KIZILAY Emergency Nutrition Services Guideline, emergency nutrition should begin as soon as possible after a disaster with ready-to-eat foods that are easy to consume and ideally have a long shelf life. After the first 72 h, long-term nutrition support should begin for the disaster victims in the form of providing nutritious hot meal service along with the distribution of family kitchen sets to allow people to prepare their own food. Family kitchen sets typically include essential items such as cooking utensils, cutlery, water containers, portable cooking equipment, hygiene supplies and food storage containers. These sets should be accompanied by 20·75 kg of dry food, which was deemed sufficient for an average family for 7 d. Additionally, KIZILAY defined the daily energy requirement per person for healthy adults as 8786·4 kJ (2100 kcal) in disasters and emergencies, of which 10–12 % of the total energy should be from protein and 17 % from fats(19).
Following the TSE, potable water was delivered to the majority of the area after the 3rd day and the distribution of warm meals at most central locations began after the 4th day. The nutritional needs of the earthquake victims in priority groups (infants, pregnant women, elderly and those with chronic diseases) along with volunteers and search and rescue teams were addressed after the 6th day. Clean water to be used for toilet and cleaning was brought after the 7th day(21). As AFAD and KIZILAY were late in coordinating disaster management, support activities were also carried out by local charitable organisations(22). According to a comprehensive report by the Chamber of Food Engineers, these efforts were unevenly distributed across the affected region, resulting in mixed amounts of food distribution to the earthquake victims. Additionally, the same report noted that the distribution of the food took place in the food preparation areas with bare hands, which may be a heightened concern in the aftermath of a natural disaster when there are contaminated water systems and limited clean water for hand washing(21).
In addition to the importance of food availability and food safety, the survivors’ diet also needs to be healthy and nutritious. Studies have demonstrated the positive impact of nutritious food at the emergency shelters on both physiological and psychological health(Reference Webb, Boyd and de Pee23,Reference Tsuboyama-Kasaoka, Hoshi and Onodera24) . On the other hand, lower intake of vegetables and high-quality protein sources coupled with an increased intake of ultra-processed foods have been associated with impaired immune response, increased risk of common cold, gastrointestinal disorders and susceptibility for chronic diseases(Reference Maayeshi and Salehi-Abargouei25,Reference Magkos, Arvaniti and Piperkou26) .
Globally, there is a dearth of research on the emergency nutrition conditions in shelters in the immediate aftermath of natural disasters. The lack of scientific evidence could preclude efforts to better support the nutrition of survivors both short and long term in the future. Therefore, the aim of this study is to evaluate the nutrition environment and the nutritional qualities of emergency meals distributed to TSE survivors in the Malatya province of Türkiye. Using data collected during direct structured observations from thirteen locations, we assessed the emergency shelter nutrition environment and alignment of the meals and/or foods with the Türkiye Dietary Guidelines (TDG)(27) in order to highlight strengths and areas for improvement to help future emergency preparations.
Materials and methods
Research setting
The research team conducted structured observations at thirteen locations that encompassed six emergency kitchens with differing sizes, three temporary earthquake shelters (one municipal indoor shelter, two outdoor shelters located at governmental institutions) that were scheduled to dissolve within a week, two mobile trucks that were loaded with meals and food, one non-governmental organisation for celiac patients and one relatively long-term earthquake shelter that could host the survivors for at least a month (Fig. 1). These thirteen locations were analysed using an embedded case–study design with replication logic(Reference Crowe, Cresswell and Robertson28,Reference Yin29) .
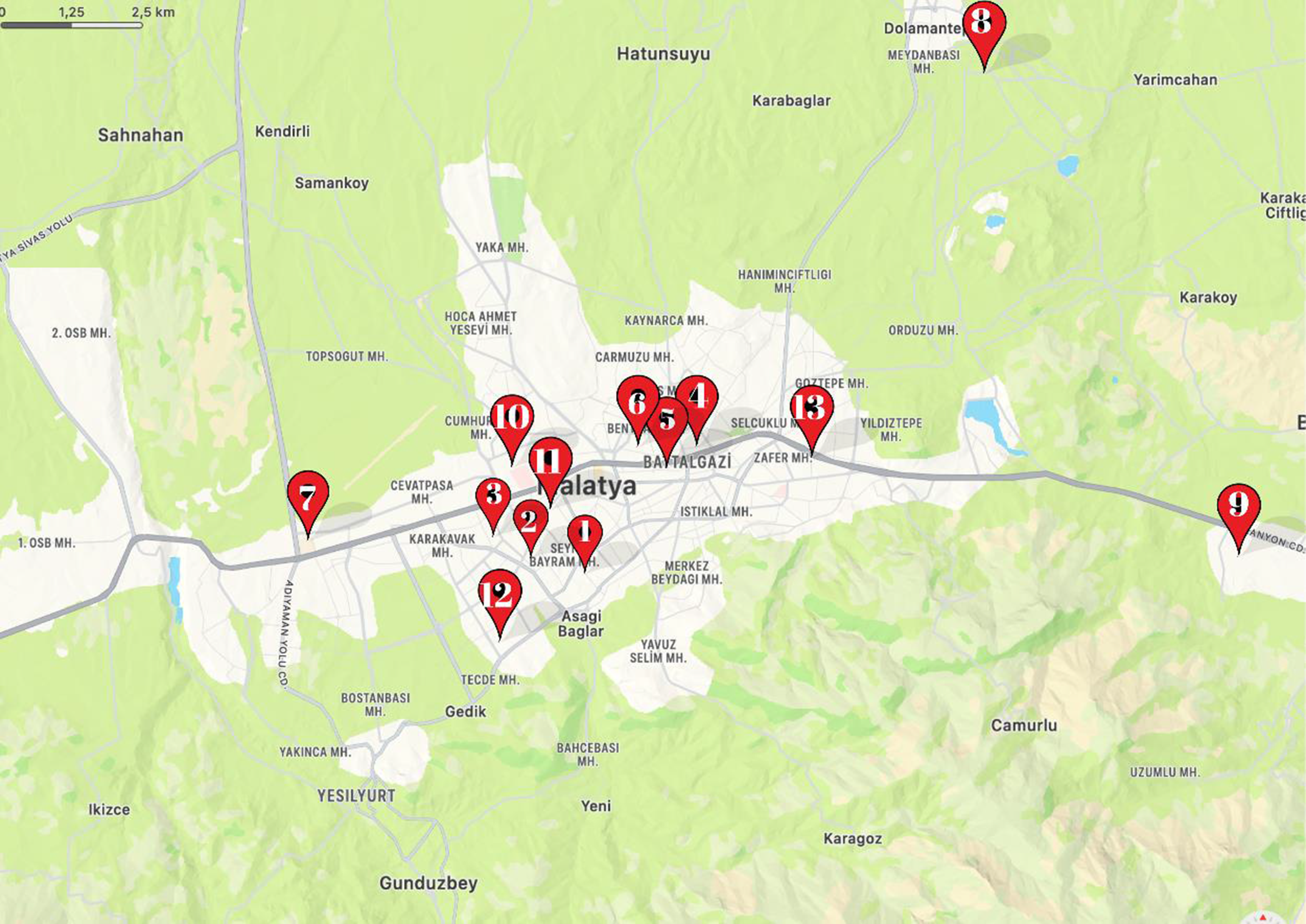
Fig. 1. Centres that were visited during the field trip in Malatya province.
Structured observation protocol
Three of the authors (ZBKA, SCK and SS) designed the structured observation protocol to document: (1) the type of foods, beverages and food preparation equipment distributed to survivors; (2) food safety at the sites including the general hygiene of the premises and the condition of kitchens; (3) presence of designated areas for breast-feeding and preparing children’s formula; (4) long-term dependability of the food supply; (5) staffing at the sites and (6) whether food waste was present. The data were collected by a trained team of nutritionists. The protocol included items on the suitability of the food for the culinary culture in terms of using familiar foods and warm meals instead of only relying on international food aid packs that might not be palatable for the local survivors. Additionally, the suitability of the food environment for chronic diseases was evaluated in terms of whether the foods and meals would be appropriate for the most common diet-related chronic diseases in Türkiye (e.g. presence of basic low salt meal alternatives for people with hypertension). Also, since more severe conditions such as cancer and chronic kidney disease require carefully planned meals, the presence of oral enteral products was also evaluated both for adults and children. The availability of healthy paediatric nutrition was assessed simply by checking the presence of baby formula and facilities to be able to prepare the formulas. Equitability of food distribution was evaluated as giving approximately the same portion to all victims. The study team documented which sites provided food packs or food boxes upon request. The study team also assessed if the number of employed or volunteering staff would be enough to distribute food based on the capacity of the kitchen and the size of the food distribution premises. The personal hygiene of the staff was evaluated by documenting the use of gloves, hair nets, clean clothing and aprons. Finally, the study team evaluated the hygiene of the toilets (Appendix: Protocol). The present study was approved by the Istanbul Aydin University Non-Interventional Clinical Research Ethics Committee (Decision Number: B.30.2.AYD.0.00.00-050.06.04/25).
Description of the fieldwork
Structured observations took place between 17 and 19 February 2023. Since there were unforeseeable power outages in the area, printed protocols were brought to be filled in by the researchers. Photographs of meals and distributed foods were taken and notes were written on the protocol for each visited location. Permission to take photos was given by an authorised staff member from each site and these administrative personnel also escorted the research team into the food preparation and storage areas. Information regarding meals distributed in the absence of the research team was also obtained from these authorised staff members. The meals and foods provided daily were recorded for each location with the confirmation of each official. A minimum two visits were conducted to each food distribution location to capture photos of different meals and the whole food distribution process. In the locations where emergency kitchens were present, the whole site was visited including the areas for receiving, preparing, cooking and distributing meals. The Turkish Dietetic Association’s Malatya representative also helped to coordinate and attended the field visits.
Quantitative data analysis
Energy and nutrient content were calculated for food and beverages provided daily at the thirteen locations observed. The macro and micro nutrient values were analysed using the Nutrition Information System (BEBIS) and the updated TDG 2022(27).
The sufficiency of the daily meals in meeting the daily total energy, carbohydrate, protein, fat, fibre, added sugar, saturated fat, total cholesterol, vitamin C, Na, Ca and Fe requirements or limits was evaluated for different sexes and age groups (10–13 years, 14–18 years, 19–70 years and individuals over 70 years old). In order to determine the portion amount in packaged products, the portion amount recommended by the manufacturer has been taken into account, if available. Otherwise, a package of food offered for personal consumption was evaluated as one portion, as it is assumed that people ate the entire package.
For the distributed warm meals, nutrient information was determined by using standardised recipes in BEBIS that are currently in use for Türkiye. Each food and beverage ingredient was evaluated under the categories of TDG 2022 food groups as: (1) milk and dairy products; (2) meat and meat products, eggs, legumes and nuts/seeds; (3) fresh vegetables and fruits; (4) bread and cereals; (5) fats; (6) sugars or (7) water and beverages. The study team calculated the percentage of total foods offered each day from each of these categories. If a single food was offered multiple times in a day, it was counted that number of times for the percentage calculations.
In addition, IBM SPSS 20.0 for Windows was used to descriptively evaluate the protocol items that are used in the field by using frequencies and percentages.
Qualitative data analysis
The photographs and the field notes used as the qualitative data sources were analysed using NVivo 1.7.1. The photographs taken at each distribution point were coded separately by two researchers, and then the codes were compared and combined to create themes and categories through thematic content analysis. The computer-aided visual analysis findings were interpreted together with the quantitative results.
Results
A total of 304 photos were included in the qualitative analysis in addition to the field notes. As a result of the thematic analysis, three themes were developed: (1) foods and beverages offered; (2) cooking/food preparation and food safety and (3) dining areas and other facilities. The results are reported according to these themes.
Foods and beverages offered
Eight observation points provided warm meals only, four provided warm meals and other food (i.e. individual packaged foods, food packs and boxes) and only one of the thirteen sites provided gluten-free food (Table 1). This last site prioritised gluten-free products for celiac patients and their relatives by registering names and addresses. Staff gave more gluten-free food to those who had travelled a far distance to the site. All other sites distributed food and meals to anyone present without registering names. Around 53·8 % of food distribution was carried out indoors with the remaining food aid provided in temporary tent cities, outside the temporary shelters, or in assembly areas.
Table 1. Characteristics of the foods and beverages offered at thirteen emergency food sites in Malatya
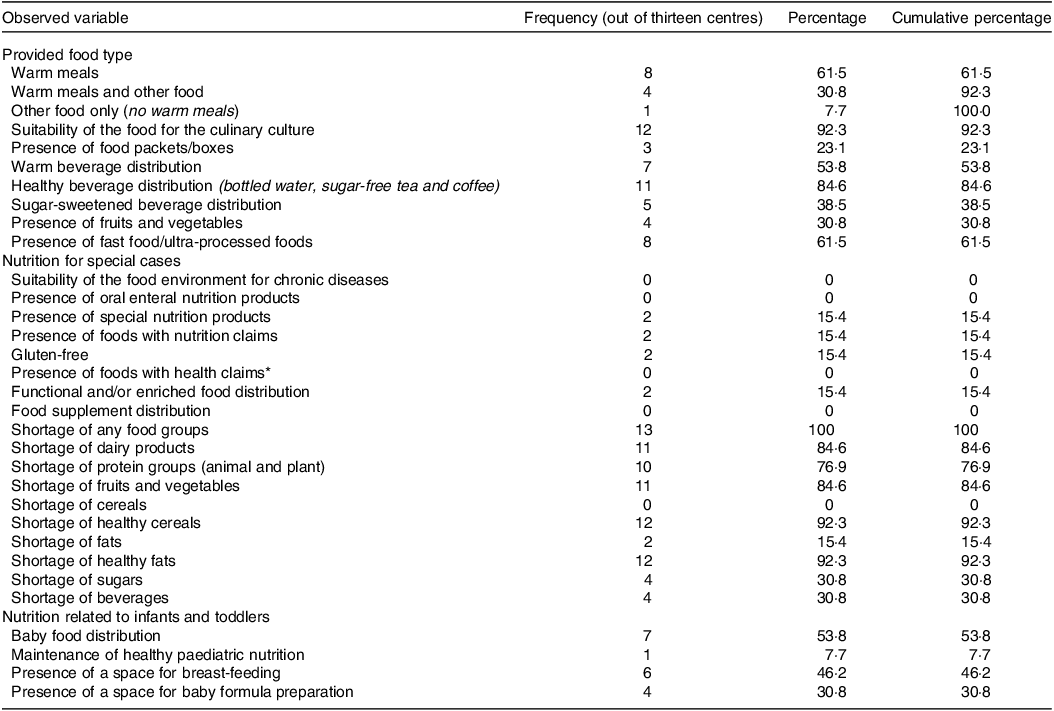
* Health claims in Türkiye refer to the voluntary information that indicates, suggests or implies the relationship of any food group, food or the elements in the composition of the food with health. An example of a health claim would be ‘This food contains low sodium. Low sodium helps reduce the risk of high blood pressure and protect cardiovascular health (56) .’
While few sites distributed functional and/or enriched food or food supplements, fast food/ultra-processed foods were distributed at eight locations (61·5 %). Some centres reserved snacks like biscuits, chocolate and confectionery for children, but these foods were no longer being distributed during the observations conducted for this study. No sites distributed fruits and vegetables together; at four locations, either a meal was made using canned vegetables or a single fruit was given to survivors. No family kitchen set, either in the form of food or essential food preparation appliances, was distributed to survivors at any point visited in the field and the interviewed officials also stated that they did not have any information in this regard.
The nutritional values of the meals were significantly below the TDG recommendations. All food groups were lacking except for the ‘bread and cereals’ group; only white bread was encountered in the field. Fig. 2 summarises the types of foods offered each day at the centres. Red lentils, green lentils and bulgur were served repeatedly and judging by the food supplies in the storage areas, red lentils and bulgur will continue to be served frequently in the time after the observation period. In the TDG, although the daily energy and protein requirements of individuals vary according to age, sex, body structure, physical activity, climate and seasonal conditions, 8368 kJ (2000 kcal)/person per day is considered an average estimate and nutrient levels are calculated based on that amount for food package labels in Türkiye(27). However, in disasters, 8786·4 kJ (2100 kcal) daily energy is recommended for individuals by KIZILAY. In addition, energy needs increase by 418·4 kJ (100 kcal)/d per each 5°C decrease in disaster areas where the air temperature is below 20°C(Reference Güden and Borlu30). Table 2 shows the total energy provided per person per day at each site along with the percentage coverage of these amounts for 8368 kJ (2000 kcal) and 8786·4 kJ (2100 kcal). Even at the 8368 kJ (2000 kcal) standard, only three of the centres provided close to three quarters of the daily energy requirements. The energy provided by the meals given at the four points evaluated in the field study was below 50 % of the daily requirement. Despite the low energy levels of the daily meals, the protein and fat percentages of most sites were in line with the KIZILAY recommendations (Table 2). However, total protein and fat fell below TDG standards. Just as total energy was lacking, levels of important nutrients did not meet the TDG standards for different sex and age groups. The nutrient analysis for 19–70 years is shown in Table 3, and the same analysis is also shown for 10–13 years, 14–18 years and individuals over 70 years old in the supplementary material. Meals served to earthquake victims and volunteers were insufficient in terms of quantities of protein, fat, fibre, vitamin C, Ca and Fe, but Na levels were higher than the maximum threshold in many of the centres.
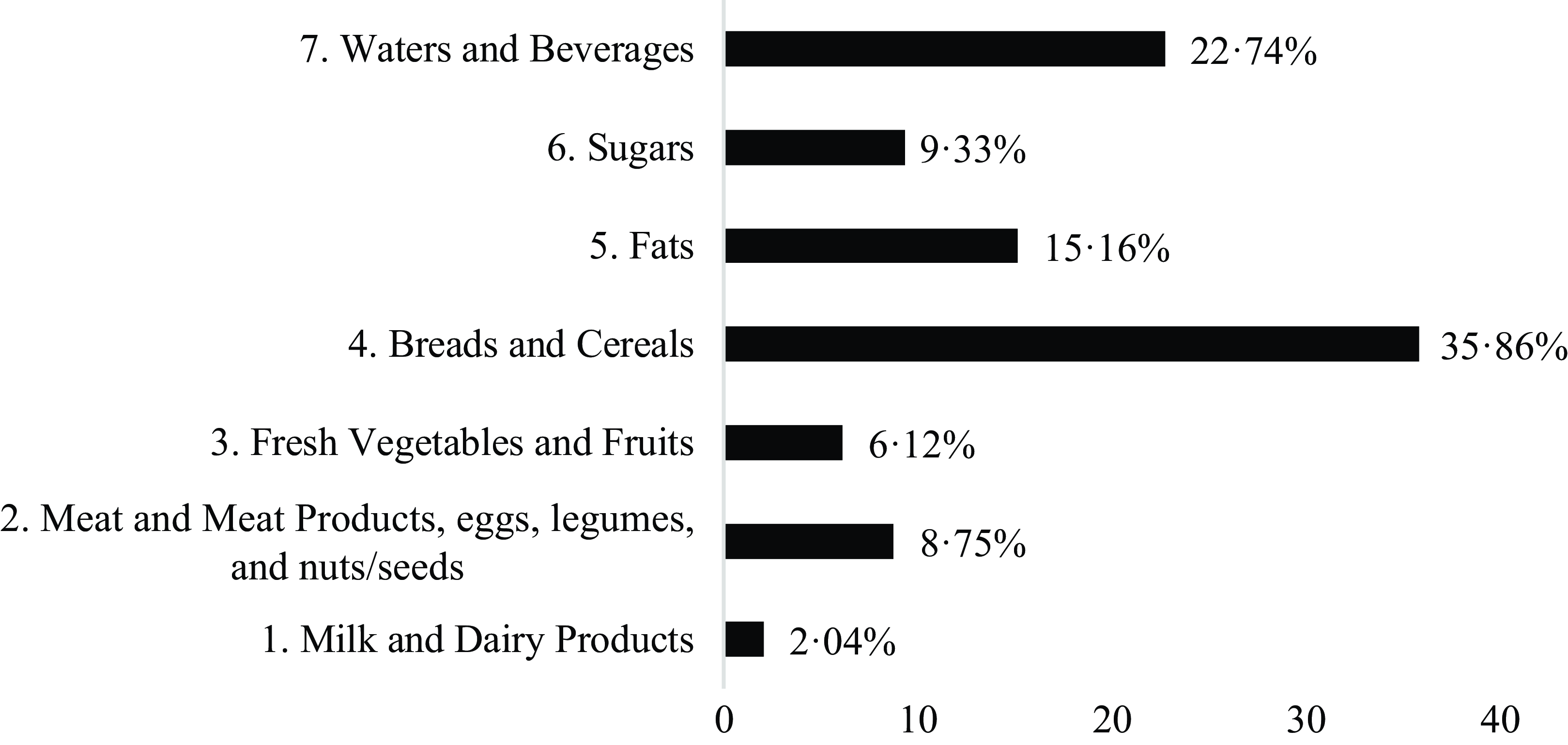
Fig. 2. Distribution of meals and foods served at the observed centres according to the food groups in TDG. TDG, Türkiye Dietary Guidelines.
Table 2. Evaluation of the total energy content of the meals served in 1 d at the observed food distribution centres according to 8368 kJ (2000 kcal)/d and 8786·4 kJ (2100 kcal)/d
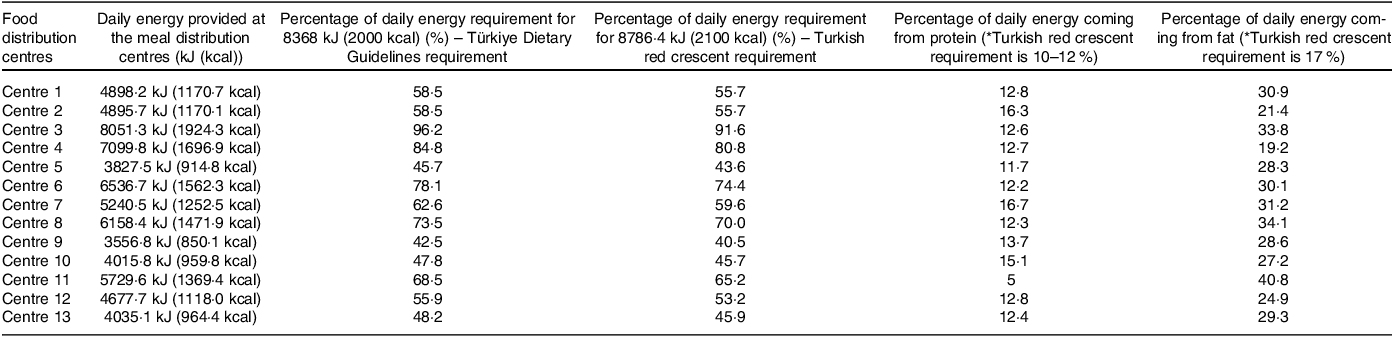
Table 3. The distribution of total daily energy and nutrients of the foods/meals served at the observed food distribution centres and the percentages of meeting TDG recommendations/thresholds for 19–70 years
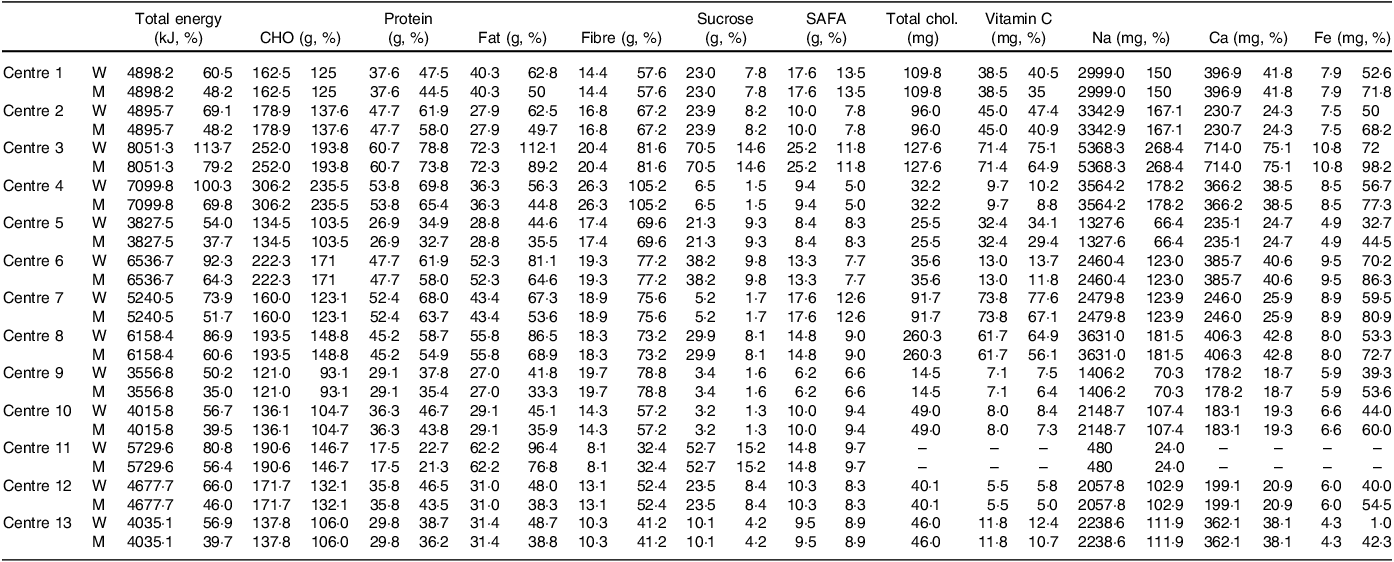
CHO: carbohydrate; SAFA: saturated fatty acids.
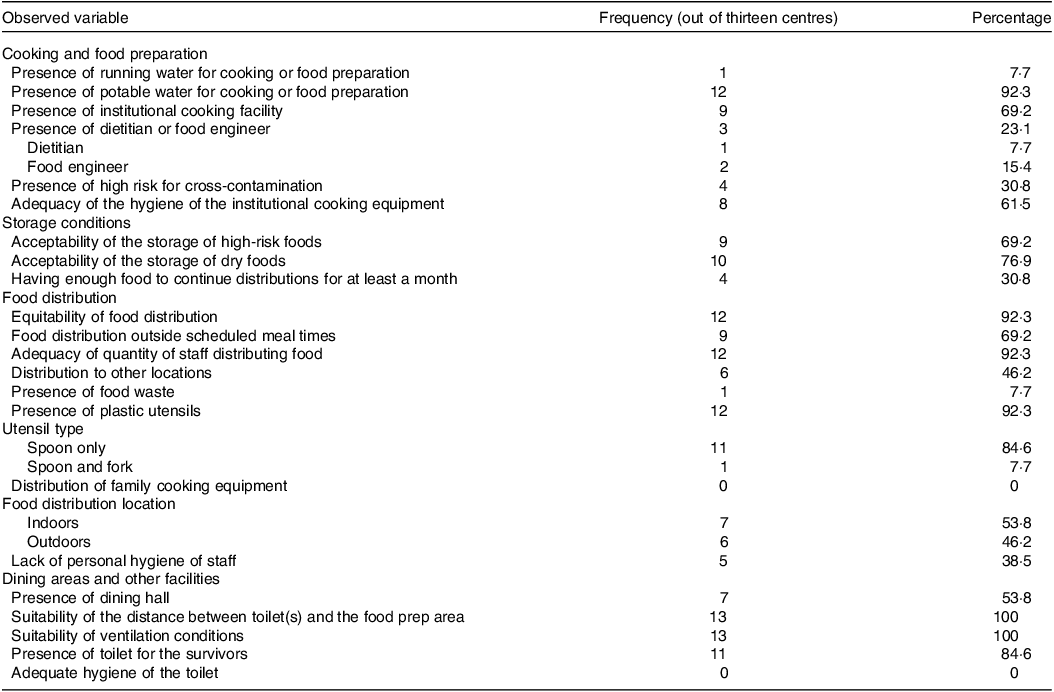
Table 4. Characteristics of the cooking and food preparation areas, dining areas and other facilities
Eleven of the sites also distributed beverages, with bottled water being the most common offering. In addition to drinking water, distribution of tea, coffee, milk, ayran (a savoury yogurt drink), fruit juice and soda was observed. Sugar-sweetened beverages were distributed only sporadically at five centres (38·5 %).
The officials interviewed in the field stated that baby formulas were distributed at seven locations (53·8 %) if requested on the dates before the current study’s observation. However, such a distribution was not observed by the research team during the structured observation days. Only one of the storage spaces had sufficient supplies to provide paediatric nutrition to meet the needs of children 0–2 years of age and only four of the sites (30·8 %) had space to prepare baby formulas hygienically if people managed to obtain some. Furthermore, no special formulas or products for children with metabolic or chronic diseases were found at any point in the field. However, six of the interviewed officials (46·2 %) stated that a special area was reserved for breast-feeding. Although most of the earthquake victims sent their children to other provinces within their financial means, the number of children in the field was observed to be quite high. However, the nutritional environment was inadequate to meet the increasing Fe needs of growing children and women who are menstruating.
Similar to the lack of paediatric nutrition for children, the nutrition environment was also not suitable for certain adults, such as those with chronic diseases or other nutritional needs (e.g. celiac disease). These individuals were not able to follow their diet since the first day of the earthquake. Anecdotally, a small number of survivors mentioned issues such as hyperglycaemia and high blood pressure due to the problem of consuming the available products and/or meals. The patients with celiac informed us about their severe diarrhoea problem when they could not follow their gluten-free diet. Overall, food for specific dietary requirements was not readily available.
With respect to chronic diseases, some officials in the field stated that the practice regarding people who say they have a chronic disease may be to put these people ahead of the line during meal distribution. Yet, everyone had to eat the food that was being distributed without any modifications. The study team noted much of the food served had a high glycaemic index value, which could be problematic for diabetics. For instance, whole grain bread was not distributed at any of the sites and white bread was frequently served as part of a meal along with foods such as white rice or pasta (Fig. 3).

Fig. 3. Examples of some meals delivered in the field study (photo on the left contains a lunch meal of white bread, white rice and potato casserole; photo on the right contains a lunch meal of pasta cooked with tomato paste and white bread).
Among the top problems that were encountered in the field was the long-term stability of the food supply. According to the officials, only four of the centres (30·8 %) could continue to provide the current menus, which were already inadequate in terms of nutritional value. Elsewhere, the officials stated that the centres were temporary and supplies would be enough to prepare food for only a few more days. In spite of the uncertainty of the source of more food, everyone was initially given the same serving size and people who requested more food were given additional servings. With respect to drinking water, the supplies were observed to be sufficient in centres that were run by local municipalities and KIZILAY.
The primary challenges associated with food distribution were prominently observed within a state college dormitory facility where food services were outsourced to a private entity. This situation arose when, on 11th February, the Council of Higher Education mandated the transition of higher education to an online format(31), necessitating the allocation of state college dormitories across Türkiye to accommodate survivors of the seismic event(32). Consequently, the responsibility of providing sustenance to these survivors was transferred to private foodservice contractors, displacing the customary student population. Access to bottled water was restricted with no alternative sources of potable water made available. Subsequent discussions with representatives of the contracted foodservice company, who were themselves survivors of the earthquake, uncovered their apprehensions were due to uncertainty about financial recompense for the additional food and beverage provisions.
Last but not least, in some centres the meals for the staff and the survivors were different, as organisers deemed it important for their staff to have sufficient energy to continue working. Also, one of the officials informed the research team that if they received a donation of only one sheep, that would not be enough to use it in the meals that were prepared for hundreds of portions. Since providing meat to some survivors and not to others may cause unrest, in such cases the meat was used to feed the staff and volunteers that were working in food preparation, food distribution and removal of debris.
Cooking/food preparation and food safety
Out of thirteen centres, nine had cooking equipment (69·2 %). These kitchens were suitable for cooking food in large quantities with all the needed basic equipment (Table 4). Food was brought to the other four locations from sites with cooking facilities. Although Malatya’s tap water was potable before 6th February 2023, the quality of the water was affected negatively after the earthquake(Reference Eye33). For this reason, water was brought from the neighbouring city of Elazig to the biggest KIZILAY kitchen, which was established in the main institutional kitchen of Inonu University, Malatya. This transport enabled the water to be potable at this location. In other locations, despite the presence of running water, it was not suitable for cooking and cleaning. Hence, all the officials that were working at kitchens reported to use purchased or donated bottled water.
Ventilation conditions in the kitchens were suitable during the daytime as either kitchen ventilation equipment was present or the windows and doors were opened periodically to let in fresh air, and the distance between food preparation areas and toilet(s) was over 10 ms.
With respect to the storage conditions, lack of refrigeration was not a big issue because it was cold enough outside to not require electric refrigeration with daytime temperatures ranging from −1 to 2°C(34). Nevertheless, 69·2 % of the locations had cold storage areas, but the temperatures were not monitored.
More problems were noted with food storage practices. Date marking was not done at all in the storage spaces. Although the duration of our observation period within the kitchens was insufficient for a comprehensive assessment of longitudinal adherence to the first-in-first-out principle(35), it was observed that a high level of proficiency in executing proper rotation practices was demonstrated by the food handlers when the ingredients were kept in their original packaging. However, important problems were observed in both cold and dry storage areas. There were many unlabelled products that were not being kept in their original packaging/container, hindering implementation of the first-in-first-out principle. Also, temperature controls were lacking at many storage spaces. In addition, ready-to-eat food was observed to be stored without being wrapped or covered, which increased the risk of cross-contamination in the storage spaces. Moreover, while products should be kept at a height of at least 15 cm above the ground(35), in each centre we saw food that was stored on the ground. In addition, we observed that in some storage spaces, spills and leaks were not cleaned immediately. The ordering of foods in the refrigerator was wrong in many places. For example, at one site, chicken was stored on the top shelf, creating a microbiological risk (Fig. 4). In addition, in one of the centres, vegetables and fruits, which were very difficult to find under earthquake conditions, were placed in an area that received sunlight at room temperature. Even though the risk of pest infestation in dry storage areas was not very high due to the winter season during the observation period, not enough precautions were taken against pests. Improper storage, cracks in walls, holes around pipes and inadequate cleaning after food and beverage spills could be potentially favourable for pests to enter the observed centres. Considering the amount of dry food that was being stored in all the visited centres, lack of integrated pest management was noted as a priority problem. Food waste was minimal, as surplus food was delivered to people working near the rubble and villages.

Fig. 4. Examples from the field kitchens in Malatya.
The food distribution personnel were experienced in working in kitchens, and there was an appropriate number of staff to prepare and serve food. However, only three of the centres (23·1 %) had either a disaster dietitian or food engineer. Moreover, kitchen staff roles changed substantially compared with before the earthquake. For example, in one site, a steward became the manager of the kitchen, as many of the cooks died during the earthquake. Even though a lot of people came to earthquake zones from the non-affected provinces to work and to volunteer, the majority of the kitchen staff was actually the local survivors themselves.
One of the most important issues to be improved in kitchens was hygiene practices (Fig. 5). An overwhelming majority of the survivors could not shower even once since the beginning of the earthquake, including staff working in food preparation and distribution areas. Additionally, despite the presence of running water, hand cleaning could not be done with the sensitivity required by food safety. Gloves and bonnets were not used in food preparation and distribution at many points despite their availability at all the visited sites.

Fig. 5. Examples of food safety risks seen in four different kitchens.
Furthermore, a substantial quantity of ready-to-eat foods were found to be stored within the temperature danger zone, defined as being maintained at ambient temperature or exceeding 5°C. Additionally, the conditions within the food preparation and distribution environments were conducive to the risk of cross-contamination due to inadequate separation of raw and cooked foods, improper storage, poor hand hygiene practices, inadequate temperature control and high traffic of people moving in a limited space (Fig. 6).

Fig. 6. Examples of improper food storage in the field study.
Dining areas and other facilities
Although there were eating areas in 53·8 % of the observed centres, the seating capacities of these areas were not very large. For this reason, many earthquake survivors had to eat either standing up or crouching on the ground. The most commonly distributed utensil was plastic spoon, which was provided at 84·6 % of the locations. However, if only soups were distributed, then no utensil was given most of the time. Many people cut their mouths on these spoons, which was yet another difficulty for the survivors, especially young children (Fig. 7). In addition, although 84·6 % of the centres had toilet(s) that earthquake survivors could use, they were unhygienic. Survivors reported they restricted their fluid consumption to avoid needing to use the toilets (Fig. 8).

Fig. 7. Examples of lack of hygiene during food distribution.

Fig. 8. Living conditions in earthquake shelters and tents.
Discussion
Türkiye is located on one of the most active seismic belts of the world and 75 % of the country’s population lives in areas where destructive earthquakes can occur(36). Following the earthquake that occurred on 17 August 1999, in Istanbul, it is well-documented that a significant build-up of seismic stress has accumulated beneath the Marmara Sea, heightening the anticipation of a substantial earthquake event in the region(Reference Eriş, Alparslan and Karadayı37–Reference Bohnhoff, Bulut and Dresen40). By 2034, there is a 62 % chance of an earthquake with a magnitude greater than 7 (Richter scale) under the Marmara Sea that poses a threat against the city of Istanbul(Reference Parsons41). Therefore, TSE was not the first major natural disaster of the century, and it is unlikely to be the last. The current study demonstrates emergency nutrition management is present, yet insufficient, as the foods offered to survivors were deficient in total energy and crucial macro and micro-nutrients. While the food provided was no doubt very helpful for survivors, it is important to identify gaps in current efforts to plan and implement better emergency nutrition support in the future.
The main findings of the study indicate that the survivors were receiving nutritionally inadequate food and meals at the visited sites. Since almost all the markets and restaurants were closed at the time of the observation, the earthquake survivors were exclusively eating the meals provided at the food distribution points. Cooking at home was also not an option as even the standing buildings were totally deserted. The study team toured across the city on both evenings of the fieldwork as part of night observations, and no lights were seen in the apartments along the streets. Since the aftershocks were still powerful enough to destroy buildings, residents could not risk entering their homes to cook food. Hence, a lot of food was being distributed throughout the city.
Although the study took place in the immediate aftermath of the earthquake, the considerable losses that occurred due to the disaster could result in an extended post-disaster period. The cost of the destruction caused by the earthquake is estimated to reach up to 104 billion dollars for Türkiye. In response to that, the highest donation pledge as of March 2023 was 7 billion Euros to both Türkiye and Syria from European Union-led donors, which will be mostly used for cleaning the debris(42). The region that was struck by the earthquake accounts for 14·5 % of Türkiye’s total agricultural GDP. TSE is estimated to have killed 815 000 livestock, halted the fishery sector and destroyed agriculture equipment such as tools and tractors. Farmers have either lost their lives or the survivors emigrated from the region if they have the financial means(43).
In addition to the effects on food production, a major challenge in Malatya is that infrastructure central to the area’s food supply chains was heavily damaged. Many food shops and restaurants were created by improperly cutting columns on the ground floors of buildings to create space. In fact, the entrance floor stores and restaurants were part of the reason why so many buildings across the whole region were heavily damaged. Not only did this practice make the buildings less earthquake resistant(Reference Koç44), it hindered the return to normal food distribution because there were no open stores or restaurants to buy food. Natural disaster survivors are thus entirely dependent on emergency food distribution.
Although rebuilding efforts have been in place since March 2023, it is hard to predict when emergency food will no longer be the main source of nutrition for the survivors. Since natural disaster survivors were found to use emergency foods for extended periods even in smaller scale disasters than the TSE, the nutritional status of the TSE survivors could become worse than it did after those previous disasters. In Türkiye, even before the disaster, a considerable majority did not meet the dietary guidelines according to TNHS 2017 results(7).
The longer the people depend on emergency foods that are even further from dietary guidelines than the typical diet, the worse their health will be affected. Studies have consistently shown that the foods provided at the emergency shelters affect the health and physical state of the survivors both short and long term(Reference Maayeshi and Salehi-Abargouei25,Reference Magkos, Arvaniti and Piperkou26) . For example, lower intake of vegetables and protein sources was associated with an increased risk of common cold, gastrointestinal disorders and stress(Reference Okuda and Hiral45). Among the top nutrition-related medium- and long-term health issues following disasters are malnutrition, micronutrient deficiencies and stunting for children(46).
There may be other long-term nutritional impacts as well. Earthquakes have been demonstrated to be a major stressor, and the stress response becomes chronic in the aftermath of such destructive natural disasters. Extended stress has been linked to emotional eating, which led to an increase in overeating in one longitudinal study after the occurrence of an earthquake in New Zealand(Reference Kuijer and Boyce47). In another study, depressive symptoms following a natural disaster-related trauma were thought to be associated with overeating as a coping response(Reference Hikichi, Aida and Kondo48). Since ultra-processed food is consumed more in such stress-related conditions, the risk of unhealthy weight gain in earthquake victims could be a problem.
Apart from overeating, another potential and current problem was found to be consuming a monotonous diet for the survivors. Since they were observed to consume a diet that lacks variety, nutrient balance will not be achieved by all. In addition, there is a potential for people to develop aversions to some of the few healthy ingredients such as red lentil, green lentil and bulgur due to repetitive consumption. Multiple studies that evaluated the post-disaster nutrition environment also reported repetitious food items to be a major problem of the survivors. Lack of diversity and uniformity of the ready-to-eat food products were documented to be a top nutritional challenge after the natural disasters. In addition to loss of appetite, lack of food diversity was associated with constipation, nausea and nutritional deficiencies(Reference Ainehvand, Raeissi and Ravaghi49–Reference Inoue, Nakao and Kuboyama51).
Ideally, the 2023 TSE earthquake will be a turning point for major improvements in Türkiye’s disaster planning and preparedness just like the 1960 earthquake was for Chile and the 1995 Great Hanshin earthquake was for Japan. After the aforementioned earthquakes, both countries developed long-term restoration and disaster management strategies that strengthen buildings and create a culture of preparedness(Reference Kitagawa52,53) . To give an example, to ensure the nutritional adequacy following the Great East Japan Earthquake, the Ministry of Health, Labour and Welfare provided the required number of meals that provided 8368 kJ (2000 kcal), 55 g protein, 1·1 mg of thiamine, 1·2 mg of riboflavin and 100 mg of vitamin C in the emergency shelters for 3 months in Japan(Reference Tsuboyama-Kasaoka and Purba54). Considering the results of the present study, future emergency nutrition plans should incorporate first and foremost the timely deployment of personnel in charge of food distribution. Disaster preparation needs to account for the fact that some people with the means to do so will leave affected areas, reducing capacity to prepare and serve food. There will also be volunteers from other places, so planners need to be ready to efficiently route them to the places where they can be most supportive. Second, sanitised water should reach the disaster region as a top priority. Organisations like AFAD and KIZILAY should employ more experienced dietitians and food engineers and not only rely on volunteers who may not have the necessary skills to deal with such a complex operation. Taking into account the food safety issues that have been documented here and in the past, Hazard Analysis Critical Control Point system plans should be incorporated in emergency nutrition plans. Also, instead of having many small kitchen operations, it would be advisable to have fewer central and large-scale food preparation areas, where food safety principles could be applied meticulously.
Considering that together with the disaster victims, disaster response teams and volunteers benefit from the meals served in the earthquake area, the energy of the meals served should be increased by adding healthy foods in line with the TDG. Culturally appropriate shelf stable foods rich in protein and/or unsaturated fatty acids like lentils, beans, chickpeas, canned food and vegetable oil should be distributed in the emergency shelters instead of ultra-processed foods.
In addition to providing more nutritious food to survivors, creating a welcoming atmosphere and distributing the food in a culturally appropriate manner should be ensured by local inspecting authorities. An example for Türkiye would be to provide a savoury breakfast (i.e. including olives, cheese, tomato and cucumber), which is among the pillars of the Turkish cuisine(Reference Kalyoncu, Demir and Ayaz55).
After the initial problems pertaining to residence are mitigated, survivors should be screened for malnutrition for medium- and long-term interventions. Infants, young children, people with special physiological conditions, elderly and people with disabilities are the most nutritionally vulnerable under temporary shelter conditions. Hence, timely detection is important for any deficiencies that may occur due to low intake of protein; vitamins A, D and B12; Fe and Zn(Reference Doğru and Ede17).
It is important to note that merely incorporating these concepts into guidelines or recommendations for disaster response may be insufficient. After the 1999 Izmit and 2002 Afyon earthquakes, issues with the emergency food responses included a limited range of food groups being served, people with chronic diseases not being able to follow their diets and food safety concerns(20). These issues persisted in the response to the TSE, despite KIZILAY publishing a comprehensive emergency nutrition plan in 2017(19). Thus, future efforts should focus on strategies to ensure timely implementation of the proposed nutrition and food safety guidelines.
In order to motivate people to donate money for providing food to victims, more transparent systems such as mobile applications could be implemented for donors to track the faith of their donations. In addition, media campaigns on the importance of healthy food could be developed to incentivise people and charitable organisations to contribute to ongoing food operations in the earthquake zones. Finally, the ultimate goal should be empowering local communities by providing a healthy nutrition environment.
A major limitation of the study was it evaluated a single province; it was not meant to be representative of all places affected by the earthquake. Second, the meals and foods could not be weighed, so standardised meal portions were used for quantitative calculations. However, direct observation of the foods and meals by a trained team of nutritionists enabled the results to be free from relying on disaster victims to remember what they ate, as would be the case for methods such as a 24-h recall. Moreover, the study team took a rigorous approach to measuring the food environment in emergency shelters. Explanations were built by both quantitative and qualitative analyses for internal validity, and a case study protocol was used for reliability purposes.
Conclusion
The findings of the current study demonstrate that the nutritional quality of the distributed foods is not compliant with the current TDG, increasing the negative impact of the natural disaster. In Türkiye, even before the disaster, a considerable majority did not meet the dietary guidelines, making it that much more important to provide adequate nutrition to avoid exacerbating existing nutritional problems. Since natural disaster survivors were found to use emergency foods for extended periods, gaps in the current emergency nutrition response were identified with an aim to plan and implement better emergency nutrition support in the future. Not only earthquakes but also other disasters such as floods, forest fires, landslides and avalanches are common in Türkiye. In order to be prepared for future disasters, the country should take this opportunity to improve emergency nutrition planning. Since natural and artificial disasters are increasing in frequency and severity globally, disaster planning and preparedness will only increase in importance in Türkiye and around the world.
Acknowledgements
We would like to thank Dr Murat Uguralp, Serkan Bentli and Arif Caliskan for their invaluable help in carrying out the field study.
The authors are grateful to The Scientific and Technological Research Council of Turkey (TUBİTAK) 1002-C Natural Disaster Focused Field Study Emergency Support Program for funding this research (grant number 85947872-605.99.09-373548).
Z. B. K. A.; Conceptualisation, methodology, investigation, and formal analysis, writing – original draft, review & editing, resources and supervision, funding acquisition. S. C. K.: Investigation, formal analysis, visualization, and writing – review & editing, J. B.-H.: Writing – original draft and writing – review & editing, S. S.: Formal Analysis and writing – review & editing, M. F. K.: Investigation and writing – review & editing and A. K.: Methodology, writing – review & editing and resources and supervision. All authors read and approved the final manuscript.
There are no conflicts of interest.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114523002672














