



Introduction
Staphylococcus aureus is a major cause of skin and soft tissue infections (SSTIs) worldwide [Reference Lowy1, Reference Dryden2]. Community-associated methicillin-resistant S. aureus (CA-MRSA) has been a global concern since it emerged in the 1990s. Although CA-MRSA strains can cause nosocomial infections, and healthcare-associated MRSA (HA-MRSA) strains do circulate in the community, CA-MRSA is epidemiologically, clinically and genetically different from HA-MRSA [Reference David and Daum3]. CA-MRSA infections tend to occur in otherwise healthy younger patients with SSTIs; such strains may be susceptible to a wider range of antibiotics, and usually harbour the staphylococcal cassette chromosome mec (SCCmec) types IV or V. The most prevalent clones of CA-MRSA have relatively unique geographic distributions, for instance, sequence type 8 (ST8, USA300) clones have mainly been reported in the USA, ST80 in Europe, ST30 in western Pacific area and ST59 in the Asia-Pacific region [Reference Deurenberg and Stobberingh4]. The global epidemic of CA-MRSA continues to evolve, and the potential shift of epidemic clones at the local, national and international levels is of great interest.
Clinicians and researchers are primarily concerned with CA-MRSA, but community-associated methicillin-susceptible S. aureus (CA-MSSA) should not be overlooked as they are the most common causative agent of SSTIs in North America, Latin America and Europe [Reference Moet5], as well as in Japan [Reference Watanabe6]. It is hypothesised that MRSA strains probably originate from MSSA strains which acquire the SCCmec determinants. Therefore, epidemiological surveillance of CA-MSSA is as important as for CA-MRSA in order for effective control of infection and transmission in the affected communities.
Currently, limited molecular characterisation data of S. aureus strains isolated from community-acquired SSTIs are available in mainland China, and particularly regarding paediatric patients in Shanghai. The aim of the present study was to determine the prevalence and molecular characteristics of S. aureus isolates recovered from paediatric patients with community-acquired SSTIs in Shanghai, the most developed city in eastern China.
Methods
Ethics
The Ethics Committee of Shanghai Children's Medical Centre exempted this study from review as it focused on bacterial isolates alone. The review board waived the need for written consent, and guardians of patients provided oral informed consent.
Bacterial isolates
This retrospective study included S. aureus isolates recovered from all paediatric patients with community-acquired SSTIs between January 2015 and January 2018 in a university teaching hospital in Shanghai (Shanghai Children's Medical Centre, one of the largest and best paediatric hospitals in China with 604 beds and approximately 22000 hospital discharges per year). SSTIs were identified by the presence of redness, swelling and localised pain. In order to eliminate possible culture contamination or bacterial colonisation, only those isolates from febrile patients (axillary temperature ≥37.5 °C or rectal temperature ≥38 °C) with increased white blood cell count were included. Community-acquired S. aureus was defined as an isolate from either an outpatient, or an inpatient within 48 h of hospitalisation, who had no medical history of S. aureus infection/colonisation, hospitalisation, surgery, dialysis or indwelling catheter in the past year. The first S. aureus isolate obtained from each patient was selected for analysis.
Antimicrobial susceptibility testing
All isolates were subjected to antimicrobial susceptibility testing using the bioMérieux Vitek 2 system according to the manufacturer's instructions. Results were interpreted following the recommendations and definitions of the Clinical and Laboratory Standards Institute (CLSI, 2017). The following 17 drugs were tested: penicillin, oxacillin, cefoxitin, erythromycin, clindamycin, gentamicin, moxifloxacin, levofloxacin, ciprofloxacin, tetracycline, rifampicin, trimethoprim-sulfamethoxazole, quinupristin/dalfopristin, nitrofurantoin, vancomycin, linezolid and tigecycline. S. aureus ATCC 29213 was used as the quality control strain. Criteria for defining multidrug-resistant S. aureus are: (i) an MRSA and (ii) an MSSA not susceptible to at least one agent in three or more antimicrobial categories [Reference Magiorakos7].
Multilocus sequence typing (MLST), staphylococcal protein A gene (spa) and SCCmec typing
All isolates were screened according to protocols described on the S. aureus MLST website (https://pubmlst.org/saureus/) and the S. aureus spa type database (https://www.spaserver.ridom.de/). Clonal complexes (CCs) were analysed using eBURST on the basis of related STs. All MRSA strains were subjected to SCCmec typing as reported previously [Reference Kondo8].
Detection of virulence genes
The presence or absence of the following 33 virulence genes was tested in all isolates as previously described [Reference Arvidson and Tegmark9–Reference Bubeck Wardenburg, Patel and Schneewind11]: staphylococcal enterotoxin genes (sea, seb, sec, sed, see, seg, seh, sei, sej, sek, sel, sem, sen, seo, sep and seq), toxic shock syndrome toxin gene (tsst-1), arginine catabolic mobile gene (arcA), exfoliative toxin genes (eta and etb), genes encoding Panton-Valentine leukocidin (PVL) and other leukocidins (lukF/S-PV, lukE and lukM), hemolysin genes (hla, hlb, hld, hlg and hlg2) and adhesin genes (clfA, icaA, sdrC, sdrD and sdrE).
Statistical analysis
Statistical analyses were performed by Stata software (version 10.1/SE, Stata Corp, College Station, TX, USA) via the χ 2 test and Fisher's exact test. Statistical significance was set at P value ⩽ 0.05.
Results
Clinical features
A total of 91 children aged 7 days to 17 years with community-acquired S. aureus SSTIs were identified. Of these, 47.3% (43/91) were male, 62.3% (57/91) were inpatients, 13.2% (12/91) were neonates, 41.8% (38/91) were under 1-year old, 20.9% (19/91) were 1 to 3 years old, 31.9% (29/91) were 4 to 10 years old and 5.5% (5/91) were teenagers.
Abscess (68.1%, 62/91) was the most common type of infection, followed by vulvitis (11.0%, 10/91), otitis externa (7.7%, 7/91), infection of eyelid and lacrimal apparatus (4.4%, 4/91) and other presentations (cellulitis, neonatal omphalitis, paronychia and wound infection). Among the 57 inpatients, 54 (94.7%) underwent surgical intervention (drainage/debridement); only 2 of 34 (5.9%) outpatients required incision and drainage.
Fifty (54.9%) children were infected with MSSA, the remainder with MRSA. Among the MSSA patients 52% (26/50) were admitted to hospital, compared with 75.6% (31/41) MRSA patients who required hospitalisation.
Molecular typing
Eighteen distinct STs were identified by MLST (Table 1); ST59 was the most common (27 MRSA and 3 MSSA isolates). All strains were clustered by eBURST into 13 CCs (CC59, CC188, CC398, CC7, CC5, CC15, CC25, CC22, CC121, CC8, CC20, CC1 and CC30) and 1 singleton (ST89) (Fig. 1).

Fig. 1. Distribution of sequence types in the CCs. The purple numbers represent 18 sequence types found in 91 community-associated S. aureus strains isolated from SSTI samples. Sequence types belonging to the same cluster are connected by a line. Each circle size is proportional to the number of isolates within the sequence type.
Table 1. Molecular typing of 91 community-acquired S. aureus isolates from paediatric patients with SSTIs
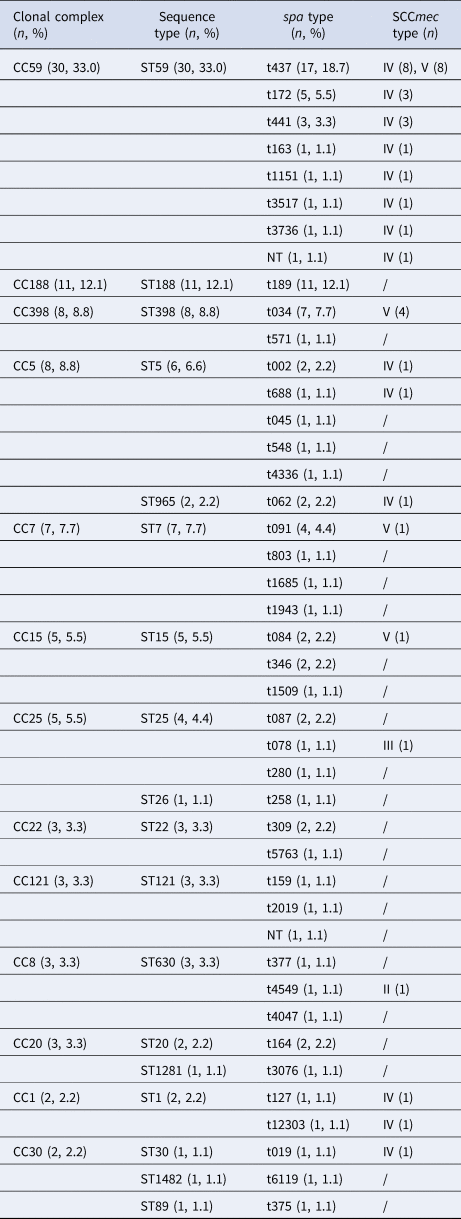
The genetic diversity of all isolates was confirmed by the identification of 41 spa types (Table 1); t437 (18.7%, 17/91: 16 MRSA, 1 MSSA) was the predominant spa type, followed by t189 (12.1%, 11/91), t034 (7.7%, 7/91), t172 (5.5%, 5/91), t091 (4.4%, 4/91) and t441 (3.3%, 3/91). Other spa types were each represented by fewer than three isolates. All t437 strains belonged to ST59, and the majority (56.7%, 17/30) of strains in this ST were spa type t437. All t189 strains fell in ST188, and vice versa.
SCCmec typing revealed 4 types (types II, III, IV and V) among the MRSA isolates (Table 1) with type IV being the most common accounting for 25 of 41 isolates (61.0%) followed by type V (34.1%, 14/41). Types II and III were each represented by single isolates.
Antimicrobial susceptibility profiles
The antimicrobial resistance profiles of isolates classified according to MLST are listed in Table 2. All were susceptible to quinupristin/dalfopristin, nitrofurantoin, vancomycin, linezolid and tigecycline. The vast majority of isolates (94.5%) were resistant to penicillin, 61.5% to erythromycin, 58.2% to clindamycin and 45.1% to oxacillin and cefoxitin. Among the MSSA isolates, 38% (19/50) were multidrug-resistant, and 24.4% (10/41) of the MRSA were resistant to ≤1 antimicrobial besides penicillin, oxacillin and cefoxitin.
Table 2. Antimicrobial susceptibility profiles of 91 community-acquired S. aureus isolates from paediatric patients with SSTIs
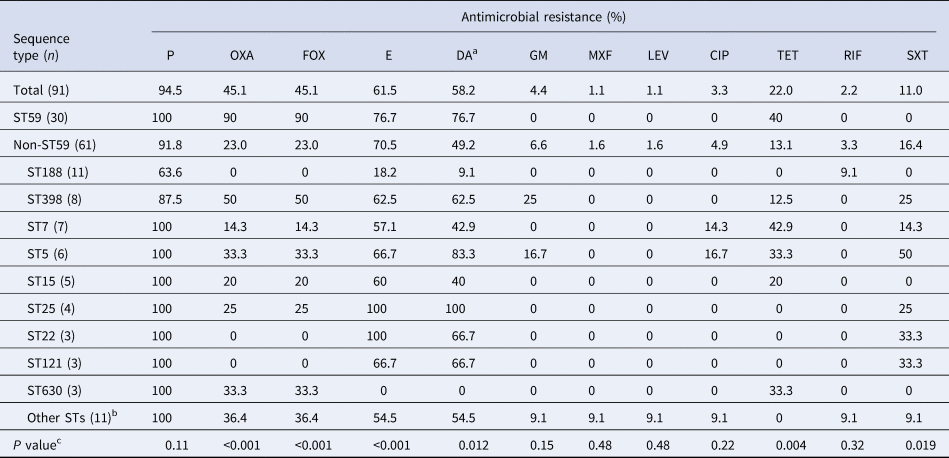
P, penicillin; OXA, oxacillin; FOX, cefoxitin; E, erythromycin; DA, clindamycin; GM, gentamicin; MXF, moxifloxacin; LEV, levofloxacin; CIP, ciprofloxacin; TET, tetracycline; RIF, rifampicin; SXT, trimethoprim-sulfamethoxazole.
a Inducible clindamycin resistance was performed with the bioMérieux Vitek 2 system.
b Other STs included ST965, ST26, ST20, ST1281, ST1, ST30, ST1482 and ST89.
c The resistance rates of antimicrobials were compared between ST59 and non-ST59 isolates.
Virulence gene profiles
Table 3 shows that each isolate carried at least six virulence genes, and 72 (79.1%) isolates were positive for ≥10 genes. All isolates carried hla, hld, icaA and clfA but none was positive for lukM and arcA genes. PVL genes were identified in 30.8% (28/91) of all isolates, with ST59 (50.0%, 14/28) being predominant. Twelve (24%, 12/50) MSSA and 16 (39.0%, 16/41) MRSA were PVL-positive (24% vs. 39.0%, P = 0.122). Twenty-two (78.6%, 22/28) patients who were infected with PVL-positive strains and 34 (54.0%, 34/63) patients who were infected with PVL-negative strains underwent surgical intervention (78.6% vs. 54.0%, P = 0.026).
Table 3. Virulence gene profiles of 91 community-acquired S. aureus isolates from paediatric patients with SSTIs
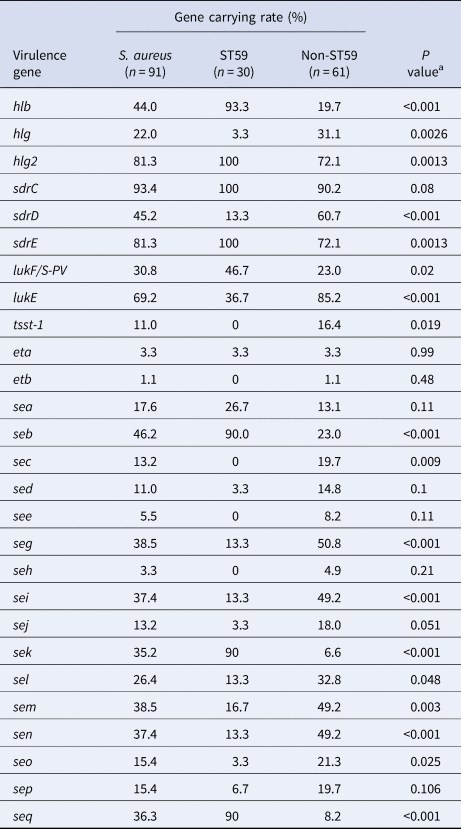
a The positive rates of virulence genes were compared between ST59 and non-ST59 isolates.
Molecular characteristics of the prevalent clone ST59
Compared with strains of other sequence types, ST59 were associated with higher resistance rates to oxacillin, cefoxitin, erythromycin, clindamycin and tetracycline, but with lower resistance to trimethoprim-sulfamethoxazole (Table 2). Likewise the presence of PVL genes among ST59 isolates was higher than for non-ST59 clones. Besides pvl, only six virulence genes: 2 encoding for haemolysin (hlb and hlg2), one adhesin (sdrE) and three enterotoxin genes (seb, sek and seq), were more common among ST59 isolates, while hlg, sdrD, lukE, tsst-1 and the enterotoxin genes (sec, seg, sei, sel, sem, sen and seo), were more common among non-ST59 isolates (Table 3).
Discussion
The proportion of CA-MRSA infections globally has increased significantly during the past 30 years. The prevalence of CA-MRSA SSTIs was reported to be 57% in the US in 2004 [Reference Moran12], but there was no report of such infections in mainland China before 2009. A few studies reported that CA-MRSA accounted for 4.0% of community-acquired S. aureus SSTIs in Beijing (northern China, isolates collected from children between 2008 and 2009), 3.4% in Guangzhou (southern China, 2006–2011, adults and children) and 10.3% in Wuhan (central China, 2011–2013, adults and children) [Reference Wu13–Reference Liu15]. Likewise a multicentre study (2009–2011, adults and children) found a low prevalence of CA-MRSA SSTIs ranging from 1.3% in northern China to 6.1% in southwestern China, and 3.8% in a children's hospital in Shanghai [Reference Liu16]. In contrast, we found the prevalence of CA-MRSA SSTIs in the present study to be surprisingly high (45.1%, 41/91). Between July 2012 and December 2013 in Shanghai Children's Medical Centre, only 3 of 13 patients (23.1%) were diagnosed as CA-MRSA SSTIs [Reference Wang17]; this rate rose to 42.1% (8/19) in 2014 (unpublished data), reaching 45.1% in the series of patients reported here. No statistically significant difference between the proportions of the initial and current was evident. Nevertheless, the data do indicate a marked increase in the total number of these infections since 2014. Although there may be regional variations, differences between adults and children and a data bias due to of small sample size, our findings indicate that the proportion of CA-MRSA SSTIs has increased rapidly in China.
A single-centre study of children with SSTIs in Beijing found ST59-SCCmec IV-spa t437 to be the major clone among CA-MRSA isolates, but no predominant spa type was evident for CA-MSSA isolates [Reference Wu13]. Likewise, a prospective surveillance study of community-acquired SSTIs conducted in 23 hospitals over a 24-month period in China, revealed that ST121 was the predominant CA-MRSA clone followed by ST59 [Reference Liu16]. Moreover, two other studies from China reported that the livestock-associated ST398 was the most prevalent PVL-positive clone of MSSA causing SSTIs [Reference Zhao18, Reference Gu19]. In our study, ST59-t437 was the major CA-MRSA clone, and ST188-t189 the most prevalent among CA-MSSA. Overall, ST59-t437 was the most common clone among community-acquired S. aureus strains isolated from paediatric SSTI patients in Shanghai. Antimicrobial resistance rather than virulence-associated genes may contribute to the spread of ST59 clone among children. As Shanghai has a highly mobile population, further studies monitoring the genotype distribution and dynamics of community-acquired S. aureus strains would be of value.
Testing for inducible clindamycin resistance was performed with the Vitek 2 system in this study. As this system has been associated with false susceptible results with for this agent [Reference Bobenchik20], the actual rate of clindamycin resistance may be higher than the 58.2% observed. However, we did not focus on clindamycin resistance as neither lincosamides nor macrolides are used for empiric or first-line treatment for SSTIs in Shanghai. The high prevalence of resistance to both erythromycin and clindamycin in our series of isolates may be associated with overuse of azithromycin in paediatric patients with acute upper respiratory infection in China, but formal evidence for this is lacking.
PVL, a bicomponent pore-forming leukotoxin inducing leukocyte destruction and tissue necrosis, is more frequently detected in S. aureus isolates associated with SSTIs and in community-acquired strains [Reference Lina21, Reference Naimi22], and the determinant genes have been reported to be more common in MRSA than in MSSA [Reference Martinez-Aguilar23, Reference Kuehnert24]. The prevalence of PVL-positive strains causing SSTIs in China was reported to range from 9.8% (5/51) to 71.4% (10/14) among CA-MRSA isolates, and from 4.2% (14/337) to 41.5% (66/159) among CA-MSSA isolates [Reference Wu13, Reference Liu16, Reference Zhao18]. Our findings for rates of PVL genes among both CA-MRSA and CA-MSSA are consistent with previous studies with a similar prevalence of PVL genes in both groups. The association of PVL with an enhanced inflammatory response and pus-forming lesions that often require surgical intervention is well documented [Reference Zhao18, Reference Bocchini25, Reference Changchien26]. Our patients with PVL-positive strains also had a higher surgical intervention rate; however, among these 56 patients the majority (60.7%, 34/56) were infected with PVL-negative trains. The actual correlations between PVL and the pathogenesis of different SSTI clinical presentations warrant further study.
This study has some limitations. Although patients came from all over China, this is a single-centre study with a relatively small sample size due to the lack of wider microbiological screening. Nevertheless, as our medical centre is ranked within the top three best and top five best paediatric hospitals in the region, and China as a whole, we consider that our findings are likely to be representative of children both regionally and nationally. In addition, as only isolates obtained from SSTI patients with fever were included, and hence classified as complicated infection [Reference Dryden2], our results may not necessarily apply to uncomplicated SSTIs, which are generally treated in community or district hospitals.
In conclusion, this study revealed that the prevalence of CA-MRSA was surprisingly high among children with community-acquired SSTIs in Shanghai, China. Clones ST59-t437 and ST188-t189 were most representative of CA-MRSA and CA-MSSA respectively; overall, ST59-t437 was the most prevalent among community-acquired SSTIs.
Acknowledgements
The authors would like to thank all the patients who contributed their specimens and clinical data for this study. We also thank the microbiologists and technical staff of Shanghai Children's Medical Centre for collecting the bacterial isolates and laboratory testing.
Author contribution
Xing Wang designed the study, collected the bacterial strains, performed the experiments, analysed the data and drafted the manuscript. Yanyun Shen designed the study, recorded the clinical data, analysed the data and drafted the manuscript. Weichun Huang collected the bacterial strains and performed the experiments. Yun Zhou designed the study, recorded the clinical data, analysed the data and reviewed and revised the manuscript. All authors approved the final manuscript as submitted.
Financial support
This work was supported by the National Natural Science Foundation of China (grant number 81301392).
Conflict of interest
None.





 Open access
Open access