


There has been a remarkable increase in the rate of multiple births in most developed countries in recent years (Hoekstra et al., Reference Hoekstra, Zhao, Lambalk, Willemsen, Martin, Boomsma and Montgomery2007; Imaizumi, Reference Imaizumi1997; Pison & Addato, Reference Pison and Addato2006). The twin birth rate in the United States increased by 70% between 1980 and 2004 (from 18.9 to 32.2 per thousand births; Martin et al., Reference Martin, Hamilton, Sutton, Ventura, Menacker and Kirmeyer2010), reaching 32.6 per thousand births in 2008. In Norway, the overall twin birth rate increased from 1.1% in 1988 to 1.9% in 2004 (Tandberg et al., Reference Tandberg, Bjorge, Bordahl and Skjaerven2007). The increasing secular trend of twin births in developed countries has been mainly attributed to assisted reproductive technology (ART), ovulation-inducing treatments, and delayed childbearing (ESHRE, 2004; Jewell & Yip, Reference Jewell and Yip1995; Lynch et al., Reference Lynch, McDuffie, Murphy, Faber, Leff and Orleans2001; Reynolds et al., Reference Reynolds, Schieve, Martin, Jeng and Macaluso2003). However, few population-based studies in China have been conducted regarding the epidemiology of twin births in recent years. The present study aimed to examine the temporal trend of twin birth rates in southeast China from 1993 to 2005.
Materials and Methods
We used data from the population-based perinatal healthcare surveillance system (PHCSS) that was established along with the community intervention trial to prevent neural tube defects with the peri-conceptive supplementation of 400 μg folic acid daily. The intervention trial was conducted from October 1993 to December 1996. The original project design and results of the neural tube defects prevention program have already been published elsewhere (Berry et al., Reference Berry, Li, Erickson, Li, Moore, Wang and The1999). The PHCSS continued to function after the original project ended in 1996. The surveillance system monitored 27 cities or counties in Hebei Province (northern China) and Jiangsu and Zhejiang Provinces (southeast China), with a population of approximately 20 million. Women were registered when they obtained a marriage license, at their first prenatal care visit, or when they sought perinatal care services.
After the women were enrolled, they were followed up through pregnancy until 6 weeks after birth. Data on the maternal demographic characteristics, medical and reproductive history, prenatal care, complications during pregnancy, pregnancy outcome, and postpartum conditions were collected using a paper booklet. The booklet was filled out by local prenatal and obstetric care providers at each prenatal visit, delivery, and postpartum visit. After the 6-week postpartum visit, the booklet was returned to the county/city Maternity and Child Health (MCH) institute, and the data were entered into a computer. The data were then transferred over a telephone line to the National Centre for Maternal and Infant Health (NCMIH) at the Beijing Medical University (BMU) for data checking and cleaning (Wang et al., Reference Wang, Zhang, Lu, Xi and Li2011).
In 2001, an electronic surveillance system was established in the southern project sites. Electronic questionnaires were used to collect the data, and the data were transferred electronically via the Internet every day from the clinics and hospitals to the server located at the county/city MCH institute. The county/city MCH institute then transferred the data electronically to the NCMIH monthly. The electronic surveillance system has been described in detail elsewhere (Zhang et al., Reference Zhang, Liu, Meikle, Zheng, Sun and Li2008).
The data collection and all methods used in the surveillance program were approved by the institutional review board (IRB) of the Peking University Health Science Centre. Informed consent was obtained from every subject (Wang et al., Reference Wang, Zhang, Lu, Xi and Li2011).
We used the data from 18 surveillance cities and counties from which data were available from 1993 to 2005. The women's characteristics were classified by province (Jiangsu or Zhejiang), residence (urban or rural), educational level (middle school or less/high school or above), and parity (primiparae or multiparae). The mother's age was divided into three groups (<25, 25–29, or ≥30) as the percentage of mothers older than 35 years was very low (1.6%).
We defined twin births as any pregnancy outcome that resulted in the delivery of two infants or fetuses, either liveborn or stillborn, at a gestation of 28 weeks or greater. Triplets and higher-order births were excluded from our analysis.
At the time of prenatal care visits or delivery, the number of fetuses or infants was noted. At birth, a separate delivery form was completed for each infant. The twin birth status was assessed based on the maternal ID number, noted number of fetuses or infants at the time of prenatal care or delivery, and the birthdates of the two infants.
The twin birth rate (per 100 maternities) was calculated. As information on zygosity is not recorded in the surveillance system, the twin birth rates according to zygosity were estimated by applying Weinberg's rule (Cavalli-Sforza & Bodmer, Reference Cavalli-Sforza and Bodmer1971), in which the proportion of opposite-sex twins and the newborn sex ratio are used to estimate the number of dizygotic (DZ) twins. The number of monozygotic (MZ) twin pairs is the total number of twin pairs minus the estimated number of DZ pairs.
The χ2 test was used to determine the differences between groups. The χ2 test for trends was also applied. A log binomial model was used to calculate the adjusted risk ratio (aRR) and 95% confidence interval. SPSS 11.5 (SPSS Inc., Chicago, IL) was used for the data analysis.
Results
From 1993 to 2005, there were 1,234,117 mothers recorded in the database. We deleted the mothers who met one or more of the following criteria: triplets and higher-order births (n = 62), more than one day between the first-born baby's birthday and the last-born baby's birthday under the same maternal ID number (n = 160), missing infant gender data (n = 3,274), gestational age at birth of fewer than 28 weeks or more than 44 weeks (n = 36,453), and maternal characteristics missing (n = 27,617). Finally, 1,166,551 mothers remained in the study group.
The distribution of maternal characteristics is presented in Table 1. From 1993 to 2005, the number of women living in urban areas increased. The percentage of women who had a high school or higher education, the percentage of women 25 years and older, and the percentage of primiparae also increased. Due to the very large sample size, all differences were considered statistically significant at p < .001.
TABLE 1 Maternal Characteristics of 18 Counties/Cities in Southeast China, 1993–2005 (%)

From 1993 to 2005, maternal age and parity changed in this population. The percentage of primiparae younger than 25 years decreased, while the percentages of primiparae aged 25–29 years and primiparae 30 years and older both increased. The percentages of multiparae younger than 25 years and between 25 and 29 years decreased.
Of all the births, 1,159,020 were singletons and 7,531 were twins (15,062 infants). The twin birth rate was 0.65%. There were estimated 4,559 (0.39%) MZ twins and 2,972 (0.25%) DZ twins.
Table 2 presents the twin birth rates according to maternal characteristics from 1993 to 2005. Residence and the mother's education level were not correlated with twin births, whereas an older maternal age was associated with twin births. In 2001–2005, this association became stronger. In 1993–1996, mothers who were multiparae were more likely to have twins (aRR = 1.26, 95% CI: 1.12–1.41). In 2001–2005, the aRR of twin births for multiparae reversed to 0.79 (95% CI: 0.68–0.91).
TABLE 2 Twin Birth Rates by Maternal Characteristics in Southeast China, 1993–2005
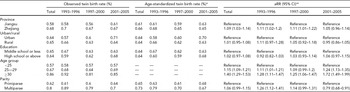
*Direct standardization with the maternal age distribution for 1993–1996 as the standard population.
**aRR adjusted relative risk, CI = confidence interval. Log binomial regression adjusted for province, age group, and parity.
The twin birth rates from 1993 to 2005 are shown in Figure 1. The total twin birth rate remained constant (0.60–0.70%) in this population, while the incidence of DZ twins tended to increase (χ2trend = 7.384, p = .007). The p value for the trend test of MZ twins was .05 (χ2trend = 3.848).

FIGURE 1 Twin birth rates in southeast China, 1993–2005.
During the three periods of 1993–1996, 1997–2000, and 2001–2005, the twin birth rates in some maternal characteristic subgroups changed (Table 2). The rates increased in urban areas (χ2 = 10.441, p = .005) and in mothers who had a high school or higher education level (χ2 = 6.176, p = .046). The twin birth rate increased in primiparae (χ2 = 6.260, p = .044) but decreased in multiparae (χ2 = 14.306, p = .001). These changes still existed after adjusting for maternal age groups.
The twin birth rates according to maternal age group and parity were also calculated. Figure 2 shows the trend for the twin birth rates among primiparae in the three age groups. The twin birth rate among primiparae younger than 25 years and primiparae aged 25–29 years remained constant. The twin birth rate among primiparae 30 years and older exhibited large fluctuations. After 2000, the birth rate increased from 0.72% to above 1.20%. In contrast, the twin birth rate among multiparae 30 years and older decreased from 0.93% (1993–1996) to 0.66% (2001–2005) (χ2 = 17.228, p = .000).

FIGURE 2 Twin birth rates of primiparae in three age groups, 1993–2005.
The percentage of twin births by primiparae younger than 25 years decreased from 49.08% in 1993–1996 to 42.05% in 1997–2000 and then stayed constant. The percentage of twin births by primiparae aged 25–29 years increased from 24.67% in 1993–1996 to 33.84% in 2001–2005. The percentage of twin births by primiparae 30 years and older was greater than 3% in 1993–1996 and 1997–2000 and increased to 8.11% in 2001–2005. From 1993 to 2005, the rate of twin births by multiparae in each of the three age groups decreased.
Discussion
The twin birth rate from 1993 to 2005 in southeast China was 0.65%. This result confirms the conclusion of the most recent literature that the very low natural twinning rate of six to nine per thousand births is the dominant pattern in the Asian region (Smits & Monden, Reference Smits and Monden2011).
Before the twin birth rates began to rise, the MZ and DZ twinning rates were approximately 4 and 2 pairs per thousand, respectively, in Japan (Imaizumi & Nonaka, Reference Imaizumi and Nonaka1997) and approximately 3.5–4 and 1–1.5 pairs per thousand, respectively, in South Korea (Hur & Kwon, Reference Hur and Kwon2005). The MZ and DZ twin rates were 0.39% and 0.25%, respectively, in southeast China. Considering the fact that the women in China were all young and primarily primiparous, the natural twinning rate in southeast China was most likely to be higher than that in Japan and Korea. However, comparisons are difficult because of differences in the populations studied, definitions of the twin rate, maternal age structure and parity.
Additionally, comparing the twin rates between different ethnicities in China would be interesting. The minority nationalities live in northeast, northwest, and southwest China, whereas our surveillance was conducted in the southeast, where most of the residents are of Han nationality (99.42%). It was a pity that the sample of minority nationalities was too small to perform analyses.
The twin birth rates may be different between urban and rural areas (Eriksson et al., Reference Eriksson, Abbott, Kostense and Fellman1995; Parisi & Caperna, Reference Parisi and Caperna1981), although the reasons for this difference are complicated. For example, between the urban and rural populations in China, there were significant differences in economic opportunities, nutrition accessibility, environment, types of work and lifestyle, family planning, physical development, life span, and so forth (Gan et al., Reference Gan, Wu, Tu and Zheng2007). Using the birth record data from the National Vital Statistics in the 1990 Census of China, Gan et al. (Reference Gan, Wu, Tu and Zheng2007) analyzed the differences between urban and rural areas with regard to the MZ and DZ twin rates according to maternal age in 1989. In all maternal age groups except for the 24- to 26-year-old age group, the DZ twinning rate in urban areas was higher than that in rural areas (Gan et al., Reference Gan, Wu, Tu and Zheng2007). In the past 13 years, although the number of women living in urban areas more than doubled, the twin birth rate was not different between urban and rural areas.
ART is more easily available to parents of high socioeconomic status. In Korea, in each year between 2003 and 2006, percentages of parents who completed college or higher level of education were higher in the twin than in the singleton group (Hur & Song, Reference Hur and Song2009). In the United States, the rates of multiple births generally parallel increasing maternal education (Luke & Martin, Reference Luke and Martin2004). In China, the education level has greatly increased over the past 13 years. The percentage of mothers who had an education level of high school or higher in 2001–2005 was almost three times that in 1993–1996. Education level was not correlated with the twin birth rate before 2005.
A higher twin birth rate has been reported in older mothers (Astolfi et al., Reference Astolfi, Ulizzi and Zonta2003; Jewell & Yip, Reference Jewell and Yip1995) and mothers with higher parity (Astolfi et al., Reference Astolfi, Ulizzi and Zonta2003; Katz et al., Reference Katz, West, Khatry, LeClerq, Christian, Pradhan and Shrestha2001). The variation in the twinning rate with maternal age and parity is largely due to variations in dizygotic twinning and is thought to be associated with gonadotrophin production (Katz et al., Reference Katz, West, Khatry, LeClerq, Christian, Pradhan and Shrestha2001). In 1993–1996 and 1997–2000, older mothers and multiparae had more twins in southeast China. In 2001–2005, the association between twin births and maternal age became stronger, and primiparae had more twins after adjusting for other confounders.
Similar to the developed countries, a trend toward older childbearing age was found in China. The percentage of primiparae in the older age groups increased in southeast China from 1993 to 2005. In England, Wales, France, the United States, and Sweden, one-fourth to one-third of the increase in twin or triplet pregnancies is attributable to the increase in maternal age (Blondel & Kaminski, Reference Blondel and Kaminski2002). In southeast China, although the percentage of primiparae in the older age group increased and the twin birth rate of primiparae 30 years and older increased, the percentage of primiparae in the older age group among the entire population was still low. At the same time, the percentage of multiparae and the twin birth rate of multiparae both decreased. Maternal age and parity were both important factors associated with twin births. The increase and the decrease canceled out each other. To remove the influence of the changes in maternal age and parity, we generated age-and-parity-adjusted rates using the direct method of standardization and 1993 as the base year. The results were similar to the original data. The changes in maternal age and parity did not yield an increase in the twin birth rate over the past 13 years.
From 1993 to 2005, the total twin birth rate remained constant over time, while the DZ twin rate increased slightly. The twin birth rate among the primiparae older than 30 years significantly increased. These changes in twin birth rates occurred after 2001, and we attempted to identify the factors responsible for the changes. The data collection methods were considered first. In 2001, the surveillance system was converted into an electronic system. Some differences in the two data collection methods may have caused these changes. However, the total twin birth rate remained constant in primiparae younger than 25 years. The two data collection methods were not different with respect to the twin pregnancy surveillance.
After the introduction of ARTs, natural twin birth rate has been changing depending on how popular these techniques have been in each country. Namely, the variations of these rates among countries were not only due to biological factors but also due to ARTs (Pison & Addato, Reference Pison and Addato2006). The increased use of fertility treatments such as in vitro fertilization (IVF), intracytoplasmic sperm injection, intra-uterine insemination, and ovulation induction is commonly cited as the main cause of the steep increase in twin births over the past two decades (Hoekstra et al., Reference Hoekstra, Zhao, Lambalk, Willemsen, Martin, Boomsma and Montgomery2007). The proportion of twin births in the United States estimated to have been conceived naturally decreased from 73.2% to 67.3% from 1997–2000, whereas the proportion attributable to ART increased from 9.1% to 11.8% (Reynolds et al., Reference Reynolds, Schieve, Martin, Jeng and Macaluso2003).
In China, the first IVF baby was born in 1988. ART developed rapidly. By the end of 2006, there were 88 institutions approved by the government to practice ART. In 2010, the number increased to more than 200 (including institutions conducting trials; Zhou, Reference Zhou2010). However, there were no population-based data from which to estimate the percentage of infertile individuals or individuals who recently used ART in China. Shanghai is one of the most developed cities in China. The multiple pregnancy rate in Shanghai from 1993 to 2002 was surveyed using hospital-based data, and the results revealed that there was no significant difference in the multiple pregnancy rate between the first and last 5 years of the survey period. The multiple pregnancies associated with ARTs (e.g., IVF-ET) were more in the last 5 years (27 cases) than in the first 5 years of the survey (1 case) (Clinical Investigatory Group of Multiple Pregnancies in Shanghai, 2004).
Social and cultural factors also contribute to the use of fertility drugs in China. Women may take such medications because they have problems conceiving or because they want to circumvent China's restrictions on the number of children they can have. The Ministry of Health issued a document in January 2005 prohibiting healthy women from using fertility drugs, but those medications are not specially protected, with both hospitals and pharmacies having the right to sell them. Women from rural areas and some well-off urban families who want more children, a dream that is impossible under the country's present family planning policy, are the two main groups of people who take such medications (Wu, Reference Wu2006).
The weakness of the present study is that we did not have accurate information regarding the potential influence of ART on twin birth rates, as information regarding fertility treatments was not collected under the perinatal healthcare surveillance system. The increases in the twin birth rates in urban areas among mothers who had a high school or higher education level and among primiparae 30 years and older indicate that one or more factors, such as ART (including fertility drugs), might have been present in these populations. However, the affected people were still in the minority and did not constitute a large enough group to influence the twin birth rate in the overall population.
To summarize, the twin birth rate in southeast China remained constant from 1993 to 2005. It was not affected by changes in the maternal age and the development of ART until 2005. However, given the changes in the maternal age and the fast development of ART, we should pay close attention to the twin birth rate among primiparae older than 30 years and the infertile population.




