



Introduction
Nearly one-third of adolescents in the United States will meet diagnostic criteria for a mental health disorder (Merikangas et al., Reference Merikangas, He, Burstein, Swanson, Avenevoli, Cui, Benjet, Georgiades and Swendsen2010). However, of youth who need mental healthcare, only 36% ever receive it (Merikangas et al., Reference Merikangas, He, Burstein, Swendsen, Avenevoli, Case, Georgiades, Heaton, Swanson and Olfson2011) and even fewer receive treatment grounded in evidence-based practices (EBPs; Garland et al., Reference Garland, Haine-Schlagel, Brookman-Frazee, Baker-Ericzen, Trask and Fawley-King2013). Primary barriers to treatment include practical or logistical impediments such as provider waitlists or transportation difficulties, as well as social barriers such as stigma, distrust of clinic-based care, and economic hardship. A significant advantage of school-based delivery of EBPs is the capacity to overcome many of these barriers (Hoover et al., Reference Hoover, Lever, Sachdev, Bravo, Schlitt, Acosta Price, Sheriff and Cashman2019; Kern et al., Reference Kern, Mathur, Albrecht, Poland, Rozalski and Skiba2017).
Cognitive behavioral therapy (CBT) is a leading EBP for addressing symptoms of mental illness, such as depression and anxiety, in school-age youth (Rasing et al., Reference Rasing, Creemers, Janssens and Scholte2017; Weisz et al., Reference Weisz, Kuppens, Ng, Eckshtain, Ugueto, Vaughn-Coaxum, Jensen-Doss, Hawley, Krumholz Marchette, Chu, Weersing and Fordwood2017). Its delivery in schools can increase access to, and more equitable delivery of, effective mental health services (Kern et al., Reference Kern, Mathur, Albrecht, Poland, Rozalski and Skiba2017), and improve students’ clinical and associated educational outcomes (Hoover et al., Reference Hoover, Lever, Sachdev, Bravo, Schlitt, Acosta Price, Sheriff and Cashman2019; Joe et al., Reference Joe, Joe and Rowley2009). Recently, studies have reported that about 35–56% of youth who receive mental health services do so in schools (Ali et al., Reference Ali, West, Teich, Lynch, Mutter and Dubenitz2019; Green et al., Reference Green, McLaughlin, Alegría, Costello, Gruber, Hoagwood, Leaf, Olin, Sampson and Kessler2013), underscoring the importance of this delivery setting.
School-based delivery of effective mental healthcare is predicated on school mental health providers (SMHPs), such as social workers, counsellors and school psychologists, having competence in delivering relevant EBPs. Therefore, programmatic efforts to implement CBT in schools must assess and track SMHP’s knowledge, perceptions, and use of CBT to optimize training methods and inform efforts to promote both initial adoption and long-term sustainment. Unfortunately, few validated measures for CBT competence are available (Muse and McManus, Reference Muse and McManus2013; Simons et al., Reference Simons, Rozek and Serrano2013), and even fewer are appropriate for school settings. This article reports on the development and validation of the Cognitive Behavioral Therapy Competence Scale (CCS), designed to assess SMHPs implementing CBT with youth.
CBT competence
A primary factor for ensuring effective and sustainable implementation of CBT interventions is practitioners’ CBT competence, defined here as ‘the degree to which a [practitioner] demonstrates the general therapeutic and treatment-specific knowledge and skills required to appropriately deliver CBT interventions’ (Muse and McManus, Reference Muse and McManus2013; p. 485). Competence requires both foundational and procedural skills. Foundational skill refers to factual knowledge of the theory and practice, as well as to practical knowledge of how and when to use that information. Procedural skills are abilities to effectively apply that knowledge in a variety of settings (Miller, Reference Miller1990; Simons et al., Reference Simons, Rozek and Serrano2013). While foundational knowledge of EBPs is necessary for effective and long-term treatment delivery, practitioners must also demonstrate knowledge of when and how to use the skills (Frank et al., Reference Frank, Becker-Haimes and Kendall2020). Furthermore, motivation to learn, use and apply an EBP is influenced by a provider’s belief that the EBP is likely to be helpful for their target population (Aarons et al., Reference Aarons, Glisson, Green, Hoagwood, Kelleher and Landsverk2012; LoCurto et al., Reference LoCurto, Pella, Chan and Ginsburg2020; Lyon et al., Reference Lyon, Ludwig, Romano, Leonard, Stoep and McCauley2013; Rogers, Reference Rogers2003). Finally, sustained implementation is predicated on providers initiating appropriate use of relevant treatment skills. Thus, these four criteria together – (a) foundational knowledge, (b) practical or applied knowledge about how and when to use an EBP’s component skills, (c) perceptions of the EBP, and (d) actual use of skills – comprise core competencies that are essential to assess when implementing a new EBP (Miller, Reference Miller1990; Muse and McManus, Reference Muse and McManus2013).
Existing CBT competence measures
Two reviews of CBT competence measures have been published within the past decade (Muse and McManus, Reference Muse and McManus2013; Simons et al., Reference Simons, Rozek and Serrano2013). Both demonstrate that the majority of existing measures rely on either observational ratings or self-report measures. While relatively objective, observational measurement is burdensome and resource-heavy, as it requires trained experts to observe delivery of at least a subset of clinical skills. The Cognitive Therapy Rating Scale (CTRS; Young and Beck, Reference Young and Beck1980) is an example of a commonly used observational tool that requires trained raters to observe and code practitioners’ proficiency in specific strategies as well as general therapeutic skills (e.g. agenda-setting and feedback). While observational measures can provide valuable data on a practitioner’s CBT skill, they require a high level of expertise, training and time to conduct, and yet still suffer from poor reliability (Rodriguez-Quintana and Lewis, Reference Rodriguez-Quintana and Lewis2018). Additionally, observational measures fail to examine factors critical for predicting sustained delivery, such as provider perceptions of the EBP (Aarons et al., Reference Aarons, Glisson, Green, Hoagwood, Kelleher and Landsverk2012; LoCurto et al., Reference LoCurto, Pella, Chan and Ginsburg2020). These characteristics render observational tools both impractical and insufficient for use in settings with limited resources and exceptional need, such as schools. Other objective methods for measuring competence include the use of role-plays; however, these too are time-consuming and are probably infeasible for use in school-based implementation efforts (Dorsey et al., Reference Dorsey, Lyon, Pullmann, Jungbluth, Berliner and Beidas2017; Liness et al., Reference Liness, Beale, Lea, Byrne, Hirsch and Clark2019).
Self-report surveys and knowledge questionnaires are more practical and efficient for implementation purposes. However, use of such tools is less common (Muse and McManus, Reference Muse and McManus2013; Simons et al., Reference Simons, Rozek and Serrano2013) due to a number of limitations. First, surveys are frequently designed to accompany a specific CBT protocol or focus on highly technical language and concepts, thus rendering them minimally generalizable (Muse and McManus, Reference Muse and McManus2013; Simons et al., Reference Simons, Rozek and Serrano2013). Second, most self-report tools focus exclusively on foundational knowledge, thus failing to measure other competencies known to be critical for implementation success, such as provider perceptions and clinical use of CBT (Herschell et al., Reference Herschell, Kolko, Baumann and Davis2010). One example of a self-report measure of CBT competence that has shown some evidence of validity includes the Cognitive Behavioral Knowledge Quiz (CBT-KQ; Myles and Milne, Reference Myles and Milne2004). The CBT-KQ was developed to evaluate practitioner’s CBT knowledge acquisition after completing a CBT training program. The CBTKQ uses highly technical language and focuses on theoretical knowledge, rather than more practical use, making it most useful for assessing knowledge acquisition among practitioners with extensive and specific training. It is also probably a poor fit for evaluating or informing implementation efforts, as it does not assess foundational knowledge, applied knowledge, perception of skills, or use of skills. Another example is the Knowledge of Evidence Based Services Questionnaire (KEBSQ; Stumpf et al., Reference Stumpf, Higa-McMillan and Chorpita2009), a measure of knowledge of evidence-based practices in treatments for youth. However, the KEBSQ is considered burdensome, as the reporter has to fill out 160 yes/no decisions, although it has recently been used with 48 yes/no decisions (Okamura et al., Reference Okamura, Hee, Jackson and Nakamura2018). Ultimately, while several CBT competence measures are available, none is designed to support or inform implementation in low-resourced settings, such as schools.
Current study
The present study sought to address the need for a psychometrically sound measure of competence for implementing CBT in schools. Informed by research identifying key predictors of adoption and sustainment of EBPs, provider competence was conceptualized to include: (a) applied knowledge of how and when to use individual CBT skills (Knowledge), (b) perceptions of CBT utility for their local settings (Perceptions), (c) frequency of skill use (Use), and (d) perceived level of expertise and comfort of CBT theory and component skills (Expertise). It was hypothesized that the resultant composite measure, the CBT Competence Scale (CCS) would demonstrate good reliability and validity among school-based providers with various levels of familiarity with CBT including novice clinicians. Figure 1 depicts the hypothesized dimensions for the CCS.

Figure 1. Conceptual model for the CBT Competence Scale (CCS).
Method
Setting
The CCS was originally developed to inform and evaluate training and post-training support offered by the TRAILS (Transforming Research into Practice to Improve the Lives of Students) program, an implementation program for school-based CBT housed at the University of Michigan and currently active in more than 75% of Michigan’s 83 counties. Programming provided to schools by the TRAILS program includes: daylong didactic training in core CBT techniques (e.g. relaxation, cognitive restructuring, exposure), provision of accessible and comprehensive clinical resources and materials, and in-person coaching (for more details on the TRAILS program model, see Koschmann et al., Reference Koschmann, Abelson, Kilbourne, Smith, Fitzgerald and Pasternak2019 and TRAILStoWellness.org. The TRAILS program model is designed to help overcome primary factors that have been shown to preclude SMHPs from utilizing CBT, including (1) minimal CBT knowledge and skills, (2) lack of access to high-quality training or post-training implementation support, (3) inadequate clinical materials and resources to support direct services to students, and (4) weak perceptions of the utility of CBT for the school setting (Langley et al., Reference Langley, Nadeem, Kataoka, Stein and Jaycox2010).
Procedures
A pool of 59 items was generated by three lead clinicians and CBT experts at the TRAILS program with the goal of covering the most fundamental, common elements of CBT interventions (Chorpita et al., Reference Chorpita, Daleiden and Weisz2005). Clinicians helped develop the CBT training of the TRAILS program and their backgrounds are a PhD in Clinical Psychology, a PhD in School Psychology, and a MD with specialization in child psychiatry. Items were reviewed by a national panel of 10 research and clinical CBT experts to establish face validity (i.e. that the items appeared to assess the hypothesized four dimensions of CBT competence) and content validity (i.e. that they covered appropriate content for each domain as it pertains to delivery of CBT in schools). All data collection procedures were approved by the Institutional Review Board at University of Michigan School of Medicine (IRBMED).
Participants
Participants were 387 SMHPs working with students in Michigan, who completed the CCS assessment through a paper-and-pencil survey or an online survey platform, Qualtrics. Data were collected between September 2018 and February 2019, from three samples: (1) n=116 eligible SMHPs recruited to complete the online assessment through a targeted Facebook advertisement (47.7% response rate); (2) n=74 SMHPs participating in a countywide TRAILS initiative, who were invited to complete the CCS prior to participating in a daylong CBT training (81% response rate); and (3) n=197 SMHPs participating in a large scale implementation trial, the Adaptive School-based Implementation of CBT (ASIC) study (Kilbourne et al., Reference Kilbourne, Smith, Choi, Koschmann, Liebrecht, Rusch, Abelson, Eisenberg, Himle, Fitzgerald and Almirall2018), who completed a baseline survey which included the CCS, prior to attending a daylong TRAILS CBT training session (87% response rate). All participants received gift cards (range $10–25) for completing the assessment, which took approximately 25 minutes.
Measures
CBT Competence Scale (CCS)
The initial CCS had 59 items examining: Knowledge, Perceptions, Use, and Expertise (see Fig. 1 for hypothesized components). The Knowledge items (n=23) assessed factual knowledge and practical understanding of CBT by asking SMHPs to identify particular CBT components or select appropriate CBT-based techniques for provided clinical scenarios. For example, one item asked SMHPs to identify the three components of the CBT model (i.e. thoughts, feelings and behaviors); while the other 22 items presented vignettes about six youth experiencing various depression/anxiety symptoms and some brief contextual descriptions, each followed by three to five CBT components from which SMHPs were asked to select the most appropriate for delivery. Expertise items (n=12) asked SMHPs to self-evaluate how comfortable they were using common components of CBT, including psychoeducation, relaxation, exposure, behavioral activation, and cognitive coping. The responses ranged from 0 (Very low: I do not really understand this skill) to 4 (Very high: I have significant expertise in this skill and understand it very well). Use items (n=12) queried how frequently SMHPs used these same CBT components with their students on a scale ranging from 0 (Never: I never or almost never use this skill) to 4 (Always: I use this skill all the time with many students). The Perceptions items (n=12) asked SMHPs to rate the effectiveness, appropriateness or helpfulness of CBT: 10 items with response choices of strongly disagree, disagree, agree, strongly agree, and don’t know, one true/false item, and one with response choices of not at all helpful, a little bit helpful, very helpful, extremely helpful, and I don’t use CBT with students.
Validation measures
Prior training and overall confidence
Two items from the survey were used to assess construct validity: (1) whether SMHPs had any prior graduate-training in CBT and (2) whether they have overall confidence in delivering CBT. We hypothesized that self-reported confidence in CBT would have a moderate correlation with the CCS, and that prior training in CBT would show a weak positive correlation.
CBT-KQ and exposure therapy knowledge
For additional validity assessments, the cohorts recruited through the Facebook advertisement and Washtenaw Intermediate School District (WISD) training (n=190) were further asked to complete two sets of additional questions: (1) eight questions from the Cognitive Behavioral Therapy Knowledge Questionnaire (CBT-KQ; Myles and Milne, Reference Myles and Milne2004) that were categorized to the General CBT Issues and Practice of Cognitive Therapy subscales of the CBT-KQ, a 26-item multiple-choice assessment of CBT declarative knowledge, and (2) an open-ended question about exposure therapy: ‘Imagine you have completed Psychoeducation, Relaxation, and Cognitive Coping with a student/patient with anxiety and at an upcoming session, you will begin Exposure. Identify 4 main components of the session plan that you would prepare.’ Responses to the exposure therapy question were then graded by a team member with a rubric, and corroborated by two expert CBT practitioners when needed; with SMHPs receiving up to 4 points. At the time the CCS was developed, no comparable instrument measured the intended construct. Therefore, the open-ended exposure question and rubric were generated internally. For both the CBT-KQ and the Exposure Therapy Knowledge, we hypothesized a weak positive correlation with the CCS total and a moderate correlation with the Objective CBT Knowledge subscale, as the CBT-KQ was developed for clinical practitioners focusing on theoretical knowledge.
Demographics
SMHPs also reported gender, race, ethnicity, highest level of education, current professional position, years in current position, years in professional field, whether they currently saw students for individual or group support/therapy, and whether they had attended professional development on CBT in the previous 5 years.
Statistical analysis
CCS validation proceeded in three steps. First, in an effort to identify the most important Knowledge items and reduce overall instrument burden, we used item response theory (IRT) to reduce the number of Knowledge vignette cases. In a second step, we combined this shorter set of vignettes with the other remaining 36 items using factor analysis to extract and validate the factor structure of the overall measure. Finally, we assessed the reliability and validity of the final composite scale and subscales: reliability was assessed via Cronbach’s alpha, and validity by examining correlations between the final CCS total and subscales and several previously validated and/or clinically informed measures.
Item response theory (IRT)
The Knowledge items were shortened using a two-parameter IRT model in Stata 15.1 with full information maximum likelihood (FIML) estimation to handle missing data. IRT provides information about each item and the test as a whole, accounting for the respondent’s ability level (Edelen and Reeve, Reference Edelen and Reeve2007; Raykov and Marcoulides, Reference Raykov and Marcoulides2018; Thomas, Reference Thomas2011; Toland, Reference Toland2014). The difficulty parameter, b, represents the level of ability required to answer each item correctly, and the discrimination parameter, a, indicates how well an item differentiates between respondents with similar ability levels. IRT also estimates how much information the instrument captures as a wholeFootnote 1 , as well as expected test scores at different levels of ability.
Our IRT analyses were applied to 23 graded Knowledge items (0=incorrect or 1=correct). The analysis proceeded as follows: first, we removed items with either a small discrimination parameter (a<.5) or an extreme difficulty parameter (b>3 or b<–3). Second, we selected the combination of vignettes with the highest maximum value of the test information function (TIF), among all possible combinations of a smaller number of cases. Third, similarities between selected items were examined using the items’ information function (IIF). The final set of Knowledge items was selected based on the IIFs and consultation with clinical experts at the University of Michigan.
Factor analyses
The shortened set of Knowledge items was combined with Perceptions, Expertise, and Use items. Perceptions items were dichotomized for the analyses: ‘1’ indicates positive perceptions and ‘0’ non-positive perceptions.Footnote 2 Factor analyses were used to extract and evaluate the instrument’s factor structure. The sample was randomly split, stratified by recruitment method. The first half (n=193) was used for exploratory factor analysis (EFA) and the second (n=194) for confirmatory factor analysis (CFA). Expertise items and Use items were considered continuous; Perceptions items and Knowledge items were analysed as binary. Factor analyses were conducted using the fa function in the psych package and cfa function in the lavaan package in R 3.5.2. Missing data were handled using pairwise deletion.Footnote 3
Exploratory factor analysis
To account for varying levels of measurement, a correlation matrix combining Pearson, tetrachoric, and biserial correlations was calculated for the EFA. Minimum residual factoring with oblique rotation was used to account for presumed correlation between factors. Items with unique contributions to one factor (i.e. primary loading ≥0.40 and cross-loadings ≤0.30) were retained, and the number of factors retained was determined based on eigenvalues, scree plot, variance explained, and factor loadings (Fabrigar et al., Reference Fabrigar, Wegener, MacCallum and Strahan1999; Zwick and Velicer, Reference Zwick and Velicer1986). Input was also sought from clinical experts throughout the process and used to adjudicate when criteria consensus was not achieved.
Confirmatory factor analysis
CFA was used to confirm the EFA factor structure. Parameters were estimated using the weighted least square mean and variance adjusted estimator (WLSMV) and robust standard errors to account for non-continuous items (Li, Reference Li2016). Model fit was assessed using the Satorra-Bentler scaling-corrected test statistic (recommended when n<250 and the normality of variables is limited; Hu and Bentler, Reference Hu and Bentler1999; Yu, Reference Yu2002), which suggests a good model fit when the Tucker-Lewis index (TLI) and comparative fit index (CFI) exceed .95 and the root mean square error of approximation (RMSEA) index is less than 0.05 (Baldwin, Reference Baldwin2019; Medina et al., Reference Medina, Smith and Long2009). Two additional measures, chi-square test and the standardized root mean square residual (SRMR) are also reported, but were not used to determine fit, given sensitivity to sample size (Hu and Bentler, Reference Hu and Bentler1999).
Reliability and validity analyses
Cronbach’s alpha was used to test the internal consistency reliability of final CCS total scale and subscales. Construct validity was assessed by examining how CCS total and subscale scores were correlated with four validation measures as discussed above. Our a priori hypotheses for the relationship between these measures and the CCS total and subscale score are shown in Table 1.
Table 1. A priori hypothesized relationships between CCS and validation measures

CBT-KQ, Cognitive Behavioral Therapy Knowledge Questionnaire; (+), positive correlations.
Results
Sample demographics
Participants were predominantly white/Caucasian (87.9%), female (88.1%), and held Master’s degrees in social work, counselling or psychology (84.8%). They had been in their current professional fields for a mean of 12.5 years (range 0–45, standard deviation (SD)=9.05, median=11) and in their current positions for a mean of 7.6 years (range=0–45, SD=7.58, median=4.25); 50.1% were school counsellors and 29.5% were school social workers; the remainder were other professionals working with students, including school psychologists, behavioral intervention specialists, and school nurses. Almost all of participants (92.8%) saw students for individual counselling, and 49.6% conducted support groups. The majority (62.5%) had attended professional development on CBT in the past 5 years, and 38.8% had received graduate training in CBT.
Item response theory
Twenty-three graded items of Knowledge were analysed using a two-parameter IRT model. Of 387 respondents, 14 (4%) who had no response on all 23 Knowledge items were excluded from IRT modelling, leaving n=373 SMHPs. IIF criteria were used, first, to remove two items with a discrimination parameter (a) less than .5 and a difficulty parameter (b) greater than 3 or less than –3. The TIF for the resulting 21-item model [a maximum TIF value, I(θ)=4.44 at latent ability level, θ=–.42] was comparable to the TIF from the 23-item model [I(θ)=4.49 at θ=–.42]. Second, the TIFs of 44 models that selected a smaller number of vignettes plus the CBT model question were compared [I(θ) ranged from 1.77 to 3.77] and three models with the highest I(θ) were selected for further examination. Next, these selected models were closely examined in terms of discrimination and difficulty parameters and IIFs in tandem with clinical expert consultation.
The final 15-item model, which includes the CBT model and four vignettes, has I(θ)=3.67 at θ=–.25, with standard error of the ability estimation (SEE)=.522 (see Appendix A in Supplementary material). Above-average respondents were expected to score >=8.3 (out of 15), and 95% of respondents were expected to score 3.17–12.7. Dropping two of six vignette cases reduced the maximum TIF value by 0.8, and the 15-item model provided sufficient amount of information over a broad range of item difficulty, while also substantially reducing respondent time and cognitive burden.
Factor analyses
Factor analyses were performed with 51 items: the 15 IRT-informed set of Knowledge items and 36 items on Perceptions, Expertise, and Use. Seventy-five (19%) respondents had missing data for one or more item, which were handled using pairwise deletion.
Exploratory factor analysis
Nearly all selection criteria endorsed the 4-factor solution; factor loadings for 5- and 6-factor solutions further found that no items had loadings above 0.4 for the final factor(s). An iterative process was then used to retain or remove items based on the statistical and conceptual inclusion criteria described above. In the first iteration, we removed ten items with primary factor loadings <0.4 and four items with cross-loadings >0.3. In the second iteration, two items were removed due to cross loadings >0.3. In the third iteration, one item with a low primary loading was removed. This set of items (n=34) was then presented to clinical experts to assess face validity; they suggested removing three items due to ambiguity and adding back two items to ensure proper coverage of key CBT elements. The four factors on n=33 final items explained 52% of the total variance (16, 16, 12 and 8%, respectively).
Confirmatory factor analysis
CFA with four latent, correlated factors was used to test the identified factor structure.Footnote 4 Standardized factor loadings and fit statistics are presented in Table 2. Goodness-of-fit indices indicated a fair to good fit using the Satorra-Bentler scaling-corrected test statistic.
Table 2. Factor loadings from exploratory factor analysis (EFA) and confirmatory factor analysis (CFA)
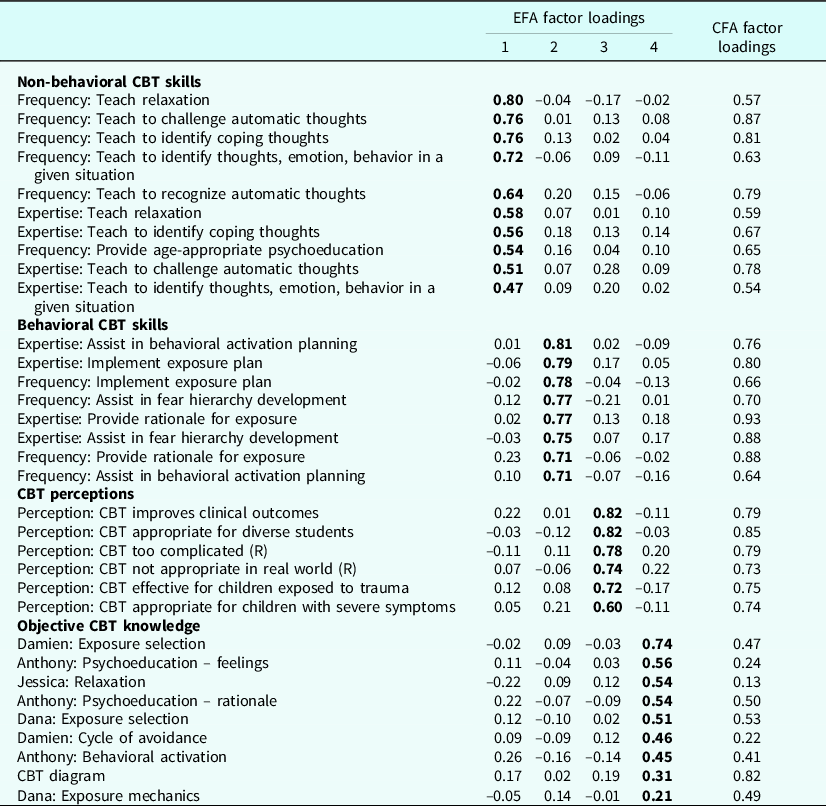
n=193 for EFA; the EFA factor loadings are in bold font where an item loads on to the factor (i.e. subscale). n=194 for CFA; the CFA factor loadings are standardized and p-values are 0.000, except for three items in Objective Knowledge (Anthony: Psychoeducation – feelings (p=0.059), Jessica: Relaxation (p=0.316), and Damien: Cycle of avoidance (p=0.088)). Goodness of fit indices from CFA: χ2 (d.f.)=804.06, p<0.001; CFI=.97; TLI=0.96; RMSEA=0.05, 90% CI [0.04, 0.05]; and SRMR=0.10
Final CCS description
The final scale included 33 items loading uniquely on four factors, defined below. Scoring instructions can be found in Appendix B of the Supplementary material. Notably, two of the originally proposed dimensions, Expertise and Use, did not inform separate factors but were split with respect to non-behavioral and behavioral CBT skills (see Fig. 1 for details).
Non-behavioral skills (10 items)
The first factor reflects the degree to which SMHPs report being comfortable with and frequently using foundational, non-behaviorally oriented CBT components (i.e. psychoeducation, relaxation, and cognitive coping). Six items reflect the frequency of SHMP skill usage, and the other four items reflect self-rated expertise in implementing those skills.
Behavioral skills (8 items)
The second factor reflects SMHPs’ comfort with and use of two advanced, behaviorally oriented CBT components: behavioral activation and exposure. Four items reflect the frequency of SMHPs skill usage and four reflect self-rated expertise and comfort in implementing those skills.
Perceptions (6 items)
The third factor reflects SMHPs’ beliefs that implementing CBT will result in positive outcomes for their students. Six items reflect the level of agreement of SMHPs with statements about CBT’s appropriateness and helpfulness.
Knowledge (8 items)
The fourth factor captures SMHPs’ applied knowledge and appropriate use of common CBT components. Eight items reflect the SMHP’s knowledge about appropriate usage of CBT skills in a set of case vignettes and the components of the CBT model.
Reliability and validity
Summary statistics and correlations for the total scale and the four subscale scores are shown in Table 3.Footnote 5 The Behavioral Skills subscale showed a lower mean score (0.84) while the Perceptions subscale had a higher mean score (3.07). The four factors were weakly-to-moderately correlated, with the highest correlation between the two skills (r=0.57). These factors were weakly correlated with Perceptions (r=0.34 and 0.26, respectively). Knowledge had the weakest correlation with other three factors (r=0.20, 0.01 and 0.23, respectively) Cronbach’s alpha internal consistency for total CCS score was 0.92, and subscale scores were 0.94, 0.92, 0.77 and 0.58, respectively. The Knowledge subscale was retained for the final CCS scale, in spite of its relatively lower level of internal consistency, as clinical experts believed it reflected an important, distinct construct for understanding and assessing CBT practice among non-clinicians. Notably, several other scales measuring cognitive constructs or knowledge assessments also report Cronbach’s alpha below .60 (Taber, Reference Taber2018).
Table 3. Summary statistics and correlations for the CCS total and subscale scores
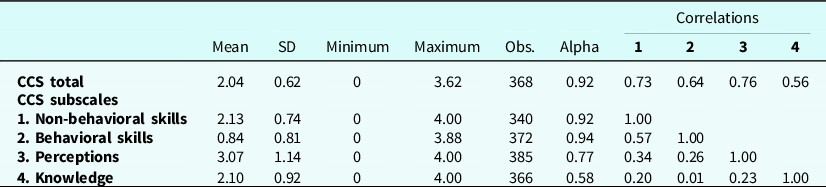
See scoring instructions for details (Appendix B in Supplementary material). Perceptions and Knowledge subscales consist of all dichotomous items; their scores were multiplied by 4 to range from 0 to 4 to compute the total score. Subscale scores were not calculated if a respondent was missing more than half of the subscale items; total score was not calculated if a respondent was missing two or more subscale scores. Cronbach’s alpha of 0.92 for total score was calculated using 33 items in their original scale.
Table 4 summarizes correlations between CCS total and subscales scores and four validation measures. As hypothesized, CCS total score showed weak positive correlations with CBT-KQ and Exposure Therapy Knowledge (r=.04, p=0.585 and r=.18, p=.02, respectively); the Objective CBT Knowledge subscale had moderate correlations with these measures (r=.31, p<.001 and r=.27, p <.001, respectively), among the cohorts recruited through Facebook advertisement and WISD training (n=190). CCS total score was positively correlated with prior graduate training in CBT (r pb=.27, p<.001), and with overall confidence in CBT (r pb=.35, p<.001), among all participants (n=387). CCS total scores were also significantly higher among those with confidence in using CBT (t 356=7.11, p<.001) and those with graduate training in CBT (t 362=5.41, p<.001). All CCS subscales except for Knowledge showed similar relationships.
Table 4. Construct-based validity evidence correlations
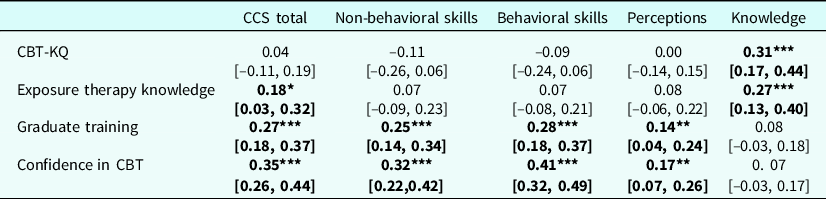
***p<.001; **p<.01; *p<.05. 95% CIs are in square parentheses. n=147–190 for CBT-KQ (a composite score from the graded eight items of CBT-KQ, ranged from 0 to 6), Exposure Therapy Knowledge (range from 0 to 4). CBT-KQ and Exposure Therapy Knowledge were asked only to the two cohorts, those who were recruited through Facebook advertisement and through WIDS training. n=329–381 for Confidence in CBT (vs none) and Graduate training (vs none). Pearson or bi-serial correlations were estimated using the cor.test function in R.
Discussion
The aim of this manuscript was to develop and validate a multi-dimensional measure of CBT competence for use with providers in school or other similar settings. Overall, following established criteria (Lewis et al., Reference Lewis, Stanick, Martinez, Weiner, Kim, Barwick and Comtois2015; Lewis et al., Reference Lewis, Mettert, Dorsey, Martinez, Weiner, Nolen, Stanick, Halko and Powell2018) the CCS demonstrated adequate psychometric properties in a sample of SMHPs, including excellent internal consistency of the total scale (Cronbach’s α=0.92), good convergent validity, excellent known-groups construct validity, and good dimensionality/structural validity, with factors explaining more than 50% of variance and a fair-to-good CFA model fit.
The CCS is a psychometrically sound and innovative multi-dimensional measure of CBT competency: Knowledge, Perceptions, Non-behavioral Skills, and Behavioral Skills. The CCS measure is a lower burden than other approaches, taking approximately 10 minutes for most respondents to complete. Practically, the CCS can be used at the total score, subscale scores, and/or item-by-item to identify specific implementation targets. For example, utilizing dimension scores might be particularly helpful in the Non-behavioral and Behavioral Skills subscales, as they encompass both frequency and comfort in using individual skills. For example, low usage and frequency of use of exposure might lead to follow-up training on this specific skill.
The CCS differentiated between SMHPs’ comfort with (as defined by both their perceived expertise and reported frequency of use of) non-behavioral and behavioral CBT common elements (i.e. psychoeducation, relaxation, and cognitive coping versus behavioral activation and exposure therapy). These findings are consistent with research indicating that behavioral elements are often under-implemented (Whiteside et al., Reference Whiteside, Deacon, Benito and Stewart2016; Wolk et al., Reference Wolk, Becker-Haimes, Fishman, Affrunti, Mandell and Creed2019), although these components, in addition to cognitive restructuring, are potentially the most effective components for youth experiencing depression or anxiety (e.g. Oud et al., Reference Oud, Winter, Vermeulen-Smit, Bodden, Nauta, Stone, Heuvel, Taher, Graaf, Kendall, Engels and Stikkelbroek2019; Whiteside et al., Reference Whiteside, Sim, Morrow, Farah, Hilliker, Murad and Wang2020). Indeed, SMHPs scored the lowest on the Behavioral Skills subscale. By differentiating between these two types of skill, CBT training programs can use the CCS to identify SMHPs for whom further scaffolding and training is needed to use the more advanced and most effective CBT components.
The relatively higher mean score for the Perceptions subscale might indicate that most SMHPs hold positive views on CBT in general, regardless of their comfort with using particular elements with students. Another explanation could be that participants were self-selected for the training, and might have come in with higher perceptions about CBT than the average SMHP. Prior research has indicated that positive perception is associated with sustained use over time (LoCurto et al., Reference LoCurto, Pella, Chan and Ginsburg2020). The Perceptions subscale was weakly to moderately correlated with other three subscales. In addition, the Knowledge subscale was weakly correlated with the other three CCS subscales. Particularly, SMHPs with higher scores on Knowledge were more likely to report slightly higher frequency of use and level of comfort using non-behavioral skills, but no such correlation was found with behavioral skills. These findings might reflect that knowledge is a precursor of skill use (Jensen-Doss et al., Reference Jensen-Doss, Cusack and de Arellano2008).
The absent correlation between the Behavioral Skills and Knowledge subscales was especially notable, contradicting expectations of their positive correlation given that literature points to knowledge preceding and being necessary for practice (Nelson and Steele, Reference Nelson and Steele2007; Rogers, Reference Rogers2003). There are several possible interpretations. First, as noted previously, few SMHPs reported high scores on the Behavioral Skills scale in our sample. Perhaps the absent correlation reflects a restricted range, thereby limiting our ability to examine scale correlates. It is also possible that the Knowledge subscale measures a broad range of knowledge related to CBT, which takes time to achieve as skills develop and generalize. To that end, respondents who had attended CBT training in the past 5 years demonstrated greater internal consistency (Cronbach’s α=0.66, n=232) than those who had not (Cronbach’s α=0.40, n=134). Future studies may examine if internal consistency for the Knowledge subscale, as well as the correlation between the Behavioral Skills and Knowledge subscales, increases over time as SMHPs receive CBT training or implementation support. Additionally, concurrent evaluation of implementation environment may help document implementation barriers that are external to the provider, such as setting constraints or low administrator support, that would not be measured by the CCS.
Finally, it is possible that SMHPs who reported that they used or felt comfortable using Behavioral Skills may not have accurate knowledge about what these skills entail (Mathieson et al., Reference Mathieson, Barnfield and Beaumont2010) and may actually be more likely to over-estimate their expertise (Kruger and Dunning, Reference Kruger and Dunning1999). Research also suggests that knowledge does not necessarily predict use of skills even though it is an important implementation target (Becker-Haimes et al., Reference Becker-Haimes, Okamura, Wolk, Rubin, Evans and Beidas2017). This discordance between Knowledge and Behavioral Skills subscales underlines the potential benefit of offering a multi-method assessment, such as the CCS that separately measures an individual’s perceived use/expertise with skills and a more objective measure of knowledge. Future research might examine how training and implementation support could be tailored to an individual’s CCS profile.
Limitations
This study has several additional limitations. First, SMHPs were not sampled randomly, but rather were included through either self-selection into a CBT training program or opting to complete a survey made available through targeted social media advertisements. Further validation efforts will need to explore the generalizability of the CCS, including evaluations of whether the observed psychometric properties of the CCS replicate with more representative samples, other populations (e.g. expert clinicians), or in different settings (e.g. in low- versus high-resource schools). Second, the size of the sample used for the analyses was only moderate and further validation with a larger sample would be beneficial. Although there is no consensus about the sample size requirement for a factor analysis or for a two-parameter IRT model, studies recommend sample sizes greater than 500 for more accurate estimations (Boateng et al., Reference Boateng, Neilands, Frongillo, Melgar-Quiñonez and Young2018). Third, predictive validity could not be evaluated in this study; future studies should assess the relationship between the CCS and key outcomes, such as CBT adoption. Fourth, even though the CCS is a lower burden measure of CBT competency, as compared with other approaches such as observational coding, it is still 33 items and takes an average of approximately 10 minutes to complete. This is probably still burdensome, especially for providers that have high volumes of cases, such as in schools that are under-resourced. More work should continue to be done to develop more pragmatic and lower burden competency measures that reduce barriers to use. Fourth, there is lack of comparison to the gold-standard approach to evaluating competency, direct observational coding. The CCS is a self-reported measure of competency, and prior literature suggests that practitioners might over-estimate their skills in self-reported measures (Hogue et al., Reference Hogue, Dauber, Lichvar, Bobek and Henderson2015). Fifth, the CCS focuses primarily on a specific set of skills used to treat depression or anxiety, which means it is not exhaustive and future iterations of the measure should consider additional skills and presenting problems.
Conclusion
The CCS is a pragmatic tool that can be utilized by a variety of stakeholders in need of evaluating SMHPs’ competence in delivering common CBT-based intervention components. The tool also has potential to serve as a CBT competence tool for broader settings undergoing implementation efforts. As demand for school- and community-based mental health EBPs increases, brief and reliable measures of SMHPs’ CBT competence will be needed to evaluate baseline skill and readiness for CBT delivery. The CCS holds promise for supporting the implementation of CBT skills among high-need settings, such as schools.
Key practice points
-
(1) Valid, reliable, and pragmatic tools of CBT competency are needed for routine care settings. The CCS attempts to fill this gap.
-
(2) Assessment of the CCS in school-based settings indicates that it has adequate psychometric properties.
-
(3) It will be important to evaluate the psychometric properties of the CCS in other routine care settings.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1754470X21000362
Acknowledgements
None.
Financial support
This work was supported by the National Institute of Mental Health (R01MH114203) and by the Centers for Medicare and Medicaid Services through the Masked Department of Health and Human Services.
Conflicts of interest
The authors have no known conflicts of interest to disclose.
Ethics statement
All data collection procedures were approved by the Institutional Review Board at the University of Michigan School of Medicine.
Data availability statement
Data are available on reasonable request to the authors.
Author contributions
Natalie RodriguezQuintana: Writing-original draft (lead), Writing-review & editing (lead); Seo Youn Choi: Data curation (lead), Formal analysis (lead), Methodology (equal), Validation (equal), Writing-original draft (equal), Writing-review & editing (equal); Emily Bilek: Supervision (equal), Writing-original draft (equal), Writing-review & editing (equal); Elizabeth Koschmann: Conceptualization- (equal), Funding acquisition (equal), Investigation-Equal, Methodology (equal), Resources (equal), Writing-review & editing (equal); Jeffrey Albrecht: Writing-original draft (equal); Michael Prisbe: Data curation (equal), Project administration (equal); Shawna Smith: Conceptualization (equal), Investigation (equal), Methodology (equal), Supervision (equal), Writing-review & editing (equal).








 Open access
Open access
Comments
No Comments have been published for this article.