



Introduction
Antimicrobial resistance (AMR) has risen on the global agenda across various sectors [1]. Drug-resistant infections cause more than 700 000 deaths worldwide each year, and are projected to rise to 10 million per year by 2050 [2]. AMR may threaten patient safety by changing the outcome of infectious disease treatment, which in turn may lead to prolonged illness and hospital admissions, disabilities or even increased mortality [3, Reference Zhen4]. Further, the impact of AMR may result in a reduction of the annual global gross domestic product, which according to current estimates could cost the world up to 100 trillion US dollars by 2050 [Reference O'Neill5].
Antibiotic resistance (ABR) is defined as the ability of bacteria to resist antibiotic agents [6]. As part of AMR, ABR is also a global health crisis [Reference Prestinaci, Pezzotti and Pantosti7], and increases the global burden of infectious diseases [2, Reference Cassini8]. Thus, alongside the continuous development of new antibiotics, a comprehensive strategy to minimise further development of ABR is critical [Reference Holmes9].
In human health, inappropriate medical prescribing practices, poor patient adherence to antibiotic therapies, and insufficient oversight and regulation are associated with the development and spread of ABR [2]. According to the US Centers for Disease Control and Prevention (CDC), despite the proportion of unnecessary prescribed antibiotics reducing from 50% to 30% in 2019, there are still over 2.8 million ABR-related infections each year in the US, resulting in more than 35 000 deaths annually [10]. Insufficient oversight and regulation on antibiotics include easy access these agents which are frequently available over-the-counter in many countries [11].
China is among the world's leading countries in terms of serious problems with AMR and ABR [Reference Tang12, Reference Tian, Zhang and Sun13]. Despite a slight decline over time, the prevalence of ABR of organisms such as carbapenem-resistant Pseudomonas aeruginosa has remained at c. 20% while carbapenem-resistant Acinetobacter baumannii has continuously risen to c. 60% [Reference Wen14]. China has more than five times the per capita use of antibiotics compared to Europe or the US [Reference Zhang15], and the country is one of the largest consumers of agricultural antibiotics worldwide [Reference Van Boeckel16]. An important driving factor of the high rates of ABR is the inappropriate use of antibiotics in healthcare settings, where strong incentives are provided for overprescribing. This trend underlines the importance of antibiotic policies to restrict their overuse [Reference Yezli and Li17–Reference Xie20]. In China, national guidelines for antimicrobial therapy were developed in 2012, and a decree for country-wide monitoring of ABR was released [Reference Xiao and Li21]; these were revised in 2017 [Reference Wen14]. China's recent health system reform suggested a pharmaceutical policy including a strategy for the rational use of medication [Reference Heddini22], but the aim of reducing overuse of antibiotics remains a significant challenge for the country [Reference Ma23–Reference Tong25].
For this paper, we systematically reviewed publications on ABR in China with the aim of identifying modifiable risk factors within healthcare settings.
Methods
Search strategy
This study aimed to systematically review research on ABR in humans and the related healthcare-associated risk factors in mainland China. The literature search was conducted using the Cochrane Library (CENTRAL), PubMed, The China National Knowledge Infrastructure (CNKI), Wanfang and VIP. The search terms were defined over the course of discussions between the authors and included controlled vocabulary (Medical Subject Headings (MeSH)). Search strategies were developed by the main researcher (QC) and three experts (CB, GL, BM) (online Supplementary Table S1).
Inclusion and exclusion criteria
Studies were included that were published between 1 January 2003 and 30 June 2019 and in either English or Chinese. Articles were included that presented original data focusing on ABR among patients in hospital settings. Reviews, opinion papers, commentaries, communications, theses and conference reports were excluded, as well as studies that did not focus on humans. There were no exclusion criteria regarding study methodology. Articles on viral, parasite and fungal drug resistance were also excluded.
Chinese academic journals are evaluated and ranked according to different criteria and institutions and are summarised in so-called ‘core academic journal lists’ [Reference Li26]. CNKI offers the possibility to search only papers from journals which are part of these lists, and we selected core academic journal lists for our study. Only the Chinese articles that appeared in the lists were included to ensure that high quality studies were included.
Study selection
The initial screening of papers was done independently by two researchers (QC, DL) who also conducted full-text screenings a random sample of which were rechecked by GL. Disagreements were resolved through joint discussion. The study selection process followed the ‘Preferred Reporting Items for Systematic Review and Meta-Analysis’ (PRISMA) guidelines and is shown in the PRISMA flow diagram (Fig. 1) [Reference Liberati27].
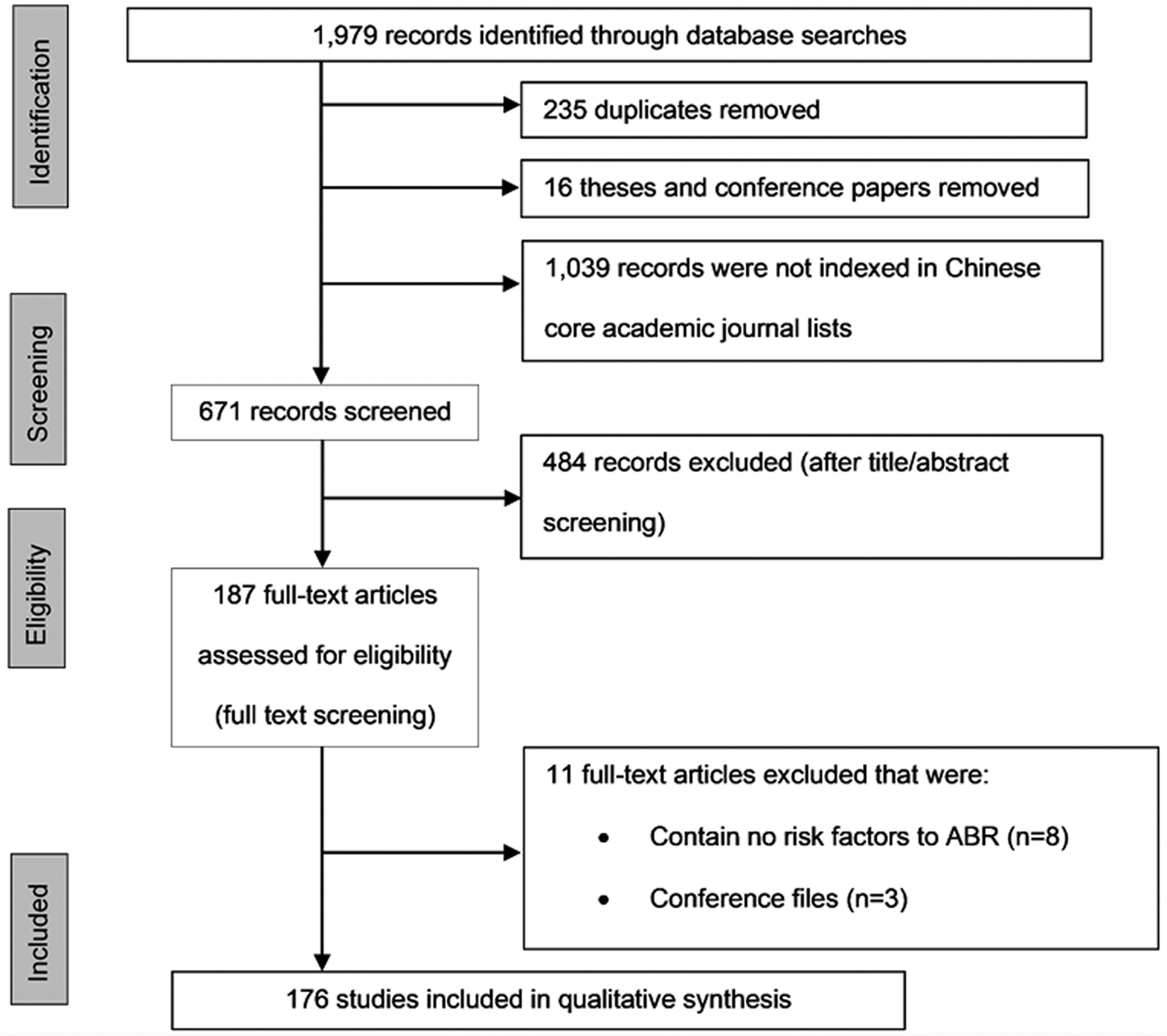
Fig. 1. Process of study selection for systematic review based on PRISMA flow diagram.
Quality assessment
The quality assessment of the selected studies was done according to the Methodological Index for Non-Randomized Studies (MINORS) [Reference Slim28]. Accordingly, 12 methodological domains were evaluated and each was scored as 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). A ‘not applicable’ category was added in case the domain did not apply to the respective study design. The risk of bias assessment was performed by QC, with a random sample of paper assessments rechecked by DL (Chinese papers) and CB (English papers).
Data extraction and analysis
Due to the heterogeneity of research in the included papers, a quantitative analysis of the data was not appropriate. Study characteristics (design and setting) were extracted, and distributions of drug-resistant bacteria, antibiotic treatment and risk factors were summarised. Identified bacterial strains and their antibiotic susceptibility test results via standard microbiological methods based on laboratory guidelines such as the Clinical and Laboratory Standards Institute were described.
The type of ABR was classified into single drug resistance (DR), multidrug resistance (MDR), extended drug resistance (XDR), and pan-drug resistance (PDR). MDR was defined as non-susceptibility of an isolate to at least one agent in three or more antimicrobial categories [Reference Magiorakos29]; XDR, as non-susceptibility to at least one agent in all but two or fewer antimicrobial categories [Reference Magiorakos29], and PDR, as non-susceptibility to all agents in all categories of antimicrobials [Reference Magiorakos29].
As a benchmark for data extraction and analysis, we adopted a method from the systematic review conducted by Chatterjee et al. [Reference Chatterjee30]. Building on this review, we summarised risk factors that were identified by the papers as statistically significant (P-values <0.05 among univariate or multivariate analyses) into four domains: (1) sociodemographic factors, (2) patient clinical information, (3) admission in healthcare settings and (4) drug exposure. Reported sociodemographic risk factors included age, sex, education level, patient residence (local or migrant) and annual income. Risk factors within the patient clinical information category included assessments for the severity of underlying disease (i.e. high scores in certain clinical assessments performed – for a detailed list of the assessments, see online Supplementary Table S3), abnormal laboratory test results (e.g. haemoglobin level, TB sputum smear-positivity and drug susceptibility of bacteria), underlying diseases (non-communicable diseases (NCDs)], infectious diseases (IDs) and other predispositions) and bacteria-related risk factors (including production of extended beta-lactamases, presence of virulence associated genes, i.e. esp, etc.). Admission in healthcare settings risk factors included previous and current hospital stay, the type of hospital facility (e.g. general department or intensive care unit (ICU)), length of hospital stay and exposure to surgery and other invasive procedures. Drug exposure risk factors included the risks of prior and current medications (especially antibiotics), monotherapy, combination therapy and longer duration of treatment or drug exposure. Prior medication refers to the medication history of the investigated patients within the past 3 months, such as prescriptions from clinical staff before having been transferred to another hospital or clinical department, or self-medication by patients.
Studies included in the review were managed in EndNote (Version X9, Philadelphia, USA, for Windows & Mac). The quality assessment was conducted in Review Manager (Version 5.3, Copenhagen, Denmark, for Windows). A data extraction table was developed in Microsoft Excel (Version 2016, Washington, USA, for Windows), and results were analysed and described accordingly. Scalable Vector Graphics (Version 1.1 Second Edition, Cambridge, USA, for Windows) was used to draw Figure 2 [31].

Fig. 2. Geographical distribution of included studies (adapted from Wikimedia Commons contributors) [31].
Results
Search results and study description
The search yielded a total of 1979 results (Fig. 1). After removing duplicates (n = 253), theses and conference papers (n = 16), and papers that were not indexed in Chinese core academic journal lists (n = 1039), a total of 671 papers remained for title and abstract screening; of these 484 were excluded during title and abstract screening, resulting in 187 articles for full-text screening. From the latter, 11 papers were excluded for specific reasons (Fig. 1). Finally, 176 studies were included in this review for synthesis (Supplementary List 1). Of these, 116 (65.9%) were written in Chinese and 60 (34.1%) in English. Table 1 details the studies included in the review. Almost all were observational, with case-control studies dominating, and all studies were facility-based. Most papers reported the number of patients included, totalling n = 53 056. Information on the number of resistant patients, isolates and resistant isolates was also reported by most papers.
Table 1. Information on included papers (n = 176)

a Two papers applied their methodologies including one case report (0.6%) and one clinical trial (0.6%).
b A total of 12 other specialty hospitals including: cancer hospital (n = 2, 1.1%), Chinese medical hospital (n = 2, 1.1%), eye, ear, nose, and throat hospital (n = 1, 0.6%), geriatric hospital (n = 1, 0.6%), maternity and child health hospital (n = 2, 1.1%), metabolic disease hospital (n = 2, 1.1%), pulmonary hospital (n = 1, 0.6%), and sexually transmitted infection and skin disease hospital (n = 1, 0.6%).
c Not every paper reported all general information (for example, the numbers of males and females do not add up to the total number of participants).
Study quality
The quality assessment graded the studies as overall low risk for bias in most domains (online Supplementary Figure S1). High risk of bias was found only in 8/176 (4.5%) in the domain of adequate statistical analyses and 11/176 (6.3%) in the domain of the prospective calculation of the study size. The domains follow-up period appropriate to the aim of the study and loss to follow-up less than 5% were not applicable to case−control and cross-sectional studies, hence the high proportions of ‘not applicable.’
Study regions
The studies took place in all regions of China (Fig. 2). In addition to the 168 regional studies, five (2.8%) targeted the whole of mainland China, two (1.1%) were conducted in the east and southwest regions, and one focused on a total of six provinces, covering north, northeast, east, south-central and southwest regions of the country.
Characteristics of antibiotic-resistant bacteria
Of the 176 included papers, 159 (90.3%) studied either DR resistance phenotypes (n = 64, 36.4%), MDR (n = 87, 49.4%), XDR (n = 3, 1.7%), or PDR (n = 5, 2.8%). Another 14 (8.0%) reported both DR and MDR pathogens; two, both MDR and XDR bacteria and one, both MDR and PDR phenotypes (0.6%).
An overview of the bacterial species reported is given in Table 2; the majority (n = 107, 60.8%) of papers documented single species, and the remainder reported on more than one. Some papers provided information about the studied bacteria at genus level only or as species pluralis (spp.), without further species definition. More reports concerned Gram-negative antibiotic-resistant bacteria than their Gram-positive counterparts.
Table 2. Antibiotic-resistant species as reported by studies (n = 176)

a No further details given by the paper.
Risk factors for ABR in healthcare settings
Applying the risk categories used by Chatterjee et al. [Reference Chatterjee30], we identified 62/176 (35.2%) papers with significant risk factors by univariate analysis, 60 (34.1%) by multivariate analysis, and 54 (30.7%) from both analyses.
An overview of the risk factors reported by the 122 (69.3%) studies analysed through univariate analysis is given in Figure 3. The percentages in the figure are the proportions of papers that reported significant effects of respective risk factor categories; frequently more than one significant effect occurred in the individual studies (i.e. adding up to more than 100%).
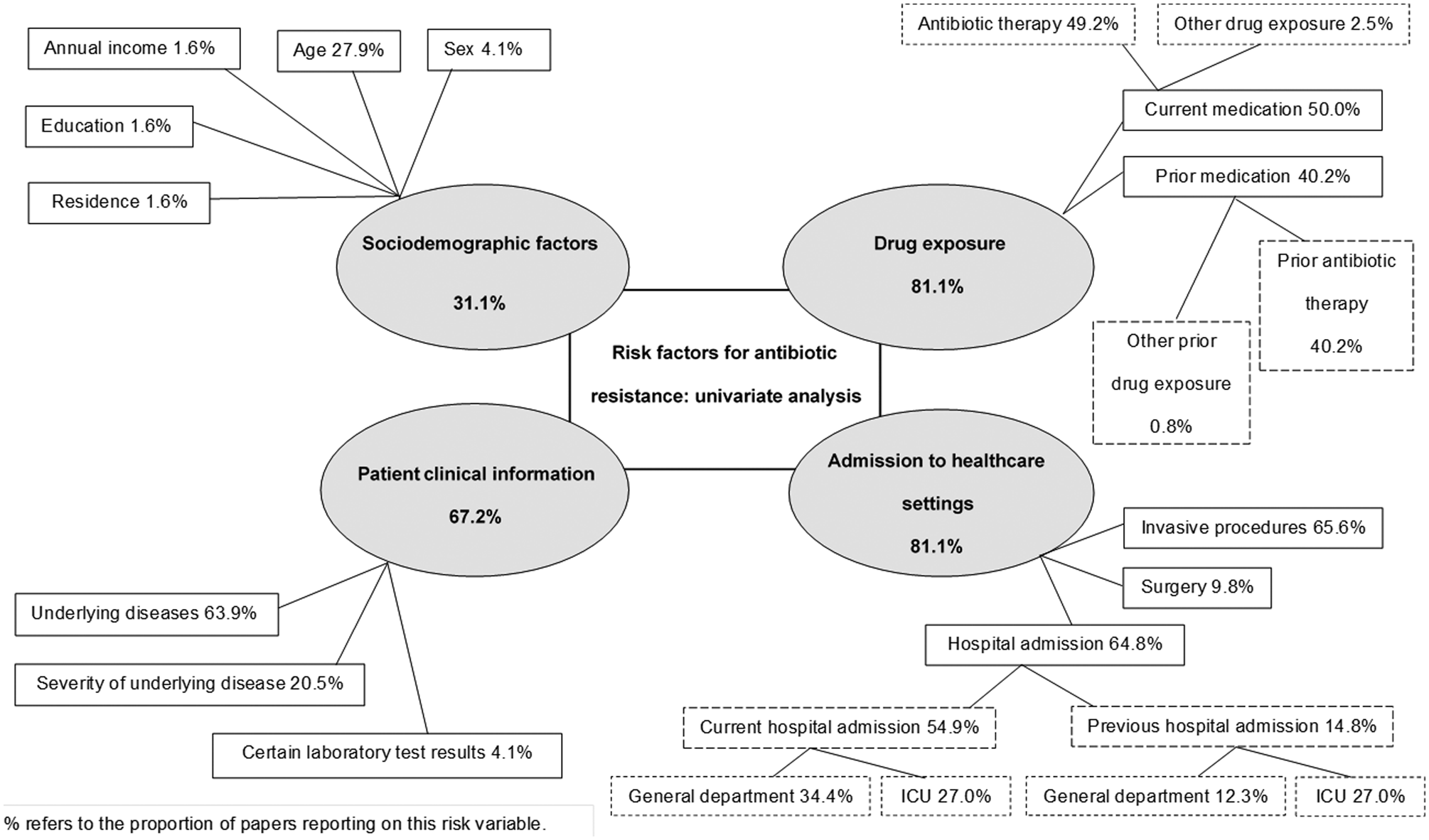
Fig. 3. Significant healthcare sector-associated risk factors from univariate analyses (n = 122).
Sociodemographic risk factors were mentioned in 31% of the papers, with age (either very young and new-borns, or older age) being the most prominent (28%). Patient clinical information was reported as a risk factor by 67% of papers, with underlying diseases the most cited (64%). Admission to healthcare settings was found to be a risk factor in 81% of the papers, with hospital stay (65%) and the performance of invasive procedures (66%) the dominant factors. Drug exposure was found to be equally important as admission to healthcare settings, particularly current or previous antibiotic therapy.
Risk factors from papers reporting on multivariate analyses (n = 114) were summarised into the same four broad risk categories. To analyse the strength of the reported evidence, odds ratios (ORs) showing significant effects were grouped into 10 different ranges, adopted from Chatterjee et al. [Reference Chatterjee30] (Table 3 and online Supplementary Table S2). The ORs were generally between 1 and 5. In the four risk categories, the following factors were identified as important independent risk factors for ABR.
(1) Sociodemographic risk factors: Older people (45–60 years, >60 years), patients with a low annual income, migrants (people who moved from another area within 6 months and were not registered in the current living area), and residents living in urban environments were all identified to be at risk of ABR infection.
(2) Patient clinical information risk factors: Higher levels in clinical scores such as APACHE II (for a detailed list, see online Supplementary Table S3) as well as a number of abnormal laboratory findings (e.g. low haemoglobin levels, positive TB sputum smear) and bacteria-related risk factors (for a detailed list, see online Supplementary Table S3) were associated with ABR. Moreover, infections (including osteomyelitis, pneumonia, and tuberculosis), NCDs (including chronic respiratory diseases, diabetes, cardiovascular diseases, and malignancies), and some other specific underlying conditions (e.g. injuries) were identified as risk factors contributing to ABR.
(3) Admission in healthcare settings risk factors: Prolonged hospitalisation was associated with ABR. Surgery and other invasive procedures were also identified as risk factors. In particular, invasive procedures in the respiratory system (e.g. artificial respiration) and urogenital system (e.g. dialysis), as well as any kind of catheter application, were associated with ABR in many papers; prolonged length of invasive procedures was also identified as a risk factor.
(4) Drug exposure risk factors: Current and prior antibiotic medication was identified as a risk factor for ABR with monotherapy being more often mentioned than combination therapy. Longer duration of antibiotic therapy was also recognised as a risk factor for ABR during both current and prior medication, but only two papers reported associations between exposure to other drugs but these were not specifically listed. Table 4 specifies the OR distribution for drug classes used for antibiotic monotherapy in current and prior medications, that were identified by multivariate analyses as risk factors. Carbapenems and cephalosporins were widely cited as risk factors in many papers.
Table 3. Simplified table for OR ranges reported by risk factor domain from 114 papers applying multivariate analysesa

a The exact OR values and ranges is listed in the Supplementary Table S2.
b Risk factors are reported as mentioned in the papers (n = number of papers). Because some papers reported multiple ORs for multiple factors within each domain, the individual rows add up to more than 100%.
c Abbreviations: Non-communicable diseases, NCD; infectious diseases, IDs.
d Prior medication refers to the medication history of the investigated patients within the past 3 months, such as prescriptions from clinical workers before they transferred from another hospital or clinical department, or self-medication by patients.
Table 4. OR distribution for drug classes used during antibiotic monotherapies from 114 papers applying multivariate analyses

a 20/51 papers reported monotherapy in current or prior medication as a significant risk factor in multivariate analyses (see Table 3 and online Supplementary Table S2) respectively; among these, different and multiple drugs could have been in use – hence, the numbers of papers citing the specific drug adds up to more than 20/51.
Discussion
This narrative systematic review provides information on the healthcare-associated risk factors contributing to ABR in China from papers published over 16 years in English and Chinese. The relevant predominant risk factors identified from the papers included current or previous hospital stay, underlying diseases, invasive procedures, laboratory test results, age and current or prior medication.
The East Region was the most common location for the studies included in this review, followed by the South-Central and North Regions of China. These regions also have the highest populations, economic development, agricultural economies and healthcare service densities [32]. The tendency towards irrational use and consumption of antibiotics may explain the status and trends of ABR in these regions compared to others in China [Reference Hu33]. Correspondingly, the highest prevalence of resistance for certain species of bacteria and antibiotics was reported from the East Region, followed by the North and South-Central Regions [Reference Qu, Huang and Lyu34, 35]. This is comparable to other countries such as India, where a higher prevalence of ABR is reported from highly populated and economically productive regions [Reference Qu, Huang and Lyu34, Reference Yam36].
ABR was more frequently associated with Gram-negative than Gram-positive bacterial species which accords with observations worldwide [Reference Chatterjee30], with an increase in ABR among Gram-negative species, and often progressing to the development of MDR [10, Reference Qu, Huang and Lyu34, Reference Tadesse37, 38].
In terms of demographic characteristics, older age, male sex, a migration background, and living in an urban environment were all reported as risk factors. The literature on these factors, however, is often inconsistent; some reports have suggested that age and sex are risk factors for ABR [Reference Erb39, Reference Sinha40] while others have not found such an association [Reference Wolfe, Cohen and Larson41, Reference Lee42]. Moreover, ABR among patients is associated with both poor adherence to therapies and high consumption of clinically inappropriate antibiotics [2, Reference Wang SC43, Reference Lin44]. Our review recognised that the social situation of migrants may play a role in poor compliance to antibiotic treatment, while urban populations seem to consume antibiotics more frequently. The latter factors along with ease of access to antibiotics at an individual level are well documented contributors to resistance development [Reference Tong25, Reference Qu45], either at the household level [Reference Chatterjee30], among village doctors, in community pharmacies [Reference Chang46], and even among medical students [Reference Hu47].
Patients with a weaker health status are more likely to develop ABR [Reference Zheng48], and in our category of patient clinical information, abnormal laboratory test results, underlying diseases, and advanced disease status were frequently reported as risk factors. It is well known that more sick patients are predisposed to carry resistant bacteria primarily because they are more likely to have had previous exposure to antibiotic treatment [Reference Prestinaci, Pezzotti and Pantosti7]. This is sometimes exemplified by the emergence of hetero-resistance in the pathogen defined as ‘a phenotype in which a bacterial isolate contains subpopulations that show a substantial reduction in antibiotic susceptibility compared with the main population’ [Reference Andersson, Nicoloff and Hjort49], which may lead to failure of antibiotic treatment. The linkage between some specific bacteria (i.e. Enterococcus spp., Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp., termed ‘ESKAPE’) and their tendency to progress towards MDR has recently gained global attention [38, Reference Founou, Founou and Essack50, Reference Pendleton, Gorman and Gilmore51]. Accordingly, infections due to this group, which are at high risk of developing resistance, necessitate improvements in routine screening and prevention measures [Reference Founou, Founou and Essack50]. Underlying conditions such as NCDs and certain infections associated with ABR in China have also been identified as risk factors in other countries [10, Reference Qu, Huang and Lyu34, Reference Tadesse37, 38].
Much ABR development is well known to occur in healthcare settings such as hospitals where extended stays and ICU admission increase the risk for the development of resistant organisms in patients [38, Reference Sonmezer52], other contributors to their spread are poor hygiene standards and inadequate infection control practice [2]. Among invasive procedures, those concerning the respiratory system were most frequently reported as significant risk factors by the papers included in this review, in agreement with a number of other investigations and reports [2, 10, Reference Sonmezer52]. This observation thus underlines the need for efficient sterilisation of instruments and maintaining a clean environment to aid prevention of ABR [Reference Ramasethu53].
Drug exposure plays a major role in the development of ABR because resistance is associated with high levels of antibiotic use [10, Reference Chatterjee30, Reference Hu33, Reference Lin44, Reference Shallcross and Davies54]. This is supported by our findings that prior antibiotic therapy is a common risk factor for the emergence of ABR, and more often a consequence of monotherapy than combination therapy. Carbapenem and cephalosporin treatment were strongly associated with ABR development in China, which threatens the effectiveness of these essential life-saving antibiotics. This is explained by the fact that these agents are widely prescribed and frequently misused in China [Reference Wen14, Reference Xiao and Li21, Reference Heddini22, Reference Qu45]. Interestingly, the use of glycopeptides has been cited as a factor promoting the increase of carbapenem resistance rates [Reference Wu, Cai and Liu55].
Periodic reviews of antibiotic susceptibility patterns for commonly used antibiotics and improved diagnosis of IDs have been recognised as effective measures for preventing ABR, alongside better training of healthcare workers and more dispersal of information to the population [Reference Shallcross and Davies54–Reference Dominey-Howes57]. The establishment of an early warning system flagging increased rates of ABR in healthcare settings is currently in preparation in China [Reference Wen14]. This approach combined with well-developed national and local guidelines for the management of antibiotics at different levels of the health system have also been proposed as valuable instruments for better control of ABR [Reference Labricciosa58, Reference Klugman and Black59]. Such surveillance networks, including monitoring of resistance trends, are under continuous development in China and other parts of the world [1, 10, Reference Hu33, 35, 38]. For China, multifaceted approaches to improving antibiotic use in the health system have been identified as effective tools to minimise the rise in ABR, including pharmacist-on-duty regulations, specific training of pharmacy staff, and general education of the public [2, Reference Chang46, Reference He60].
This review has some strengths and limitations. One strength is that it considered not only English but also Chinese literature, and for the latter only the highest-quality papers published in core academic journals over more than 16 years were considered. A possible limitation is that information on certain parameters might have been lost through exclusion of the Chinese language papers which did not pass the quality check.
Conclusion
ABR constitutes an ongoing major public health challenge in China. The healthcare sector-associated risk factors was the most important aspect identified in this review and such factors need to be addressed through a reduction of antibiotic exposures, long hospital stays and invasive procedures, within the hospital setting. The findings also point to a need to strengthen primary health care to prevent and control NCDs, over-prescription and overuse of antibiotics through better training of healthcare workers and pharmacists, as well as strengthening of health promotion and health literacy among the general population. Finally, AMR surveillance networks would benefit from being linked to other sectors, such as agriculture and veterinary practice, to further adopt the One Health Approach.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0950268821001254.
Acknowledgements
We acknowledge the financial support by the Open Access Publishing Fund of Ruprecht-Karls-Universität Heidelberg, and the financial support from the China Scholarship Council (CSC) to QC (No. (2016)3100).
Authors' contributions
The study was designed by OM and GL. The development of the search terms and search strategy was done by QC together with OM, CB, GL and BM. The quality check for the Chinese literature was performed by QC and GL. The risk of bias assessment was performed by QC. The assessment of Chinese papers was rechecked by DL. QC, DL and CB were involved in resolving disagreements. Title, abstract and full-text screening were done independently by QC and DL. Data extraction and synthesis were performed by QC. QC and CB wrote the first draft of the manuscript. All authors contributed to writing the manuscript.
Financial support
This review is funded by National Natural Science Foundation of China (NSFC) (Grant No. 71904165), and Jiangsu Planned Projects for Postdoctoral Research Funds (Grant No. 2020Z003).
Conflict of interest
We declare no competing interests.
Ethical standards
Not applicable.
Availability of data and material
The datasets of this narrative systematic review are included within this article and its supplementary materials.










 Open access
Open access
{kind=link}