


Previous research has documented marked differences in the risk of suicide in different occupational groups.Reference Milner, Spittal, Pirkis and LaMontagne1 However, most studies focus on single occupationsReference Hawton, Clements, Simkin and Malmberg2–Reference Heller, Hawgood and De Leo5 and the most recent studies for England are based on data from more than 10 years ago and some used potentially biased methods to assess risk.Reference Meltzer, Griffiths, Brock, Rooney and Jenkins6–Reference Roberts, Jaremin and Lloyd8 Analysis of deaths registered between 2001 and 2005 found the highest risk of suicide in males was among health professions and agricultural workers, and in females among health as well as sports- and fitness-related occupations.Reference Meltzer, Griffiths, Brock, Rooney and Jenkins6 Changes in the workplace together with the availability of census data on occupation mean an updated assessment of occupation-specific suicide risk is timely.
Three factors are thought to contribute to occupational suicide risk. First, job-related features such as low pay, low job security and risk of injury are important;Reference Agerbo, Gunnell, Bonde, Mortensen and Nordentoft9 debt, unemployment and physical health problems are, in turn, well-recognised risk factors for suicide.Reference Mäki and Martikainen10,Reference Jonsson, Alexanderson, Kjeldgård, Westerlund and Mittendorfer-Rutz11 Second, selection effects whereby people who are potentially more vulnerable to suicide because of specific personality or behavioural characteristics may choose particular occupations, e.g. caring professions, publicans.Reference Kelly and Bunting7,Reference Goldney12 Third, some occupations provide ready access to, or technical knowledge about, highly lethal methods of suicide such as drugs or firearms; this physical and cognitive accessibility increases risk, as suicide attempts are more likely to result in death.Reference Hawton, Clements, Simkin and Malmberg2,Reference Malmberg, Simkin and Hawton3,Reference Goldney12–Reference Skegg, Firth, Gray and Cox14 Based on an Office for National Statistics (ONS) review of occupational suicide risk,15 this paper presents an analysis of occupational suicide risk for deaths between 2011 and 2015 in England.
Method
Using data held by the ONS on death registrations in England during the calendar years 2011–2015, standardised mortality ratios (SMRs) were calculated for suicides among people aged 20–64 years old for each occupation.
Suicide was defined as deaths given as an underlying cause of self-harm (ICD-10 codes: X60–X84) and deaths due to injury or poisoning of undetermined intent (Y10–Y34); most of the latter deaths are thought, on clinical review, to be likely suicides.Reference Gunnell, Bennewith, Simkin, Cooper, Klineberg and Rodway16
The deceased's occupation at the time of death is recorded on the death certificate and, in some instances, is based on the last occupation of the deceased if they were out of work (e.g. due to retirement, being unemployed, being sick). The ONS codes this information using the Standard Occupation Classification (SOC2010)17 which includes 9 major groups of occupations and more than 350 individual occupations. To provide the population at risk, population counts for occupations among those who said they were employed, also coded to SOC2010, were obtained from the information collected at the 2011 Census. We restricted the analysis to people aged 20–64 years to improve the comparability between the occupation recorded at census and that at the time of death registration.
We summarise the occupation-specific risks of suicide using the SMR (indirect standardisation). This commonly used measure establishes whether the number of suicides in an occupation is high or low relative to age- and gender-specific patterns of suicide in the broader population (i.e. all usual residents in England aged 20–64 years). Other studiesReference Meltzer, Griffiths, Brock, Rooney and Jenkins6–Reference Roberts, Jaremin and Lloyd8 have quantified occupation-specific risk using the proportional mortality ratio (PMR); the PMR establishes whether the proportion of total deaths due to a specific cause (e.g. suicide) is higher or lower than the proportion of deaths due to that cause in the wider population, and is often used in the absence of reliable population denominators. A limitation of the PMR is that, in healthier/higher-income occupations, the incidence of some common causes of death such as cardiovascular disease and cancer is low; hence suicide – as a proportion of all deaths among those in these occupations – will be high, leading to a spuriously high estimate of risk.
To estimate SMRs we used Stata (version 11 for Windows). We used age- and gender-specific rates of suicide in England (2011–2015) in 5-year age bands to calculate the number of suicides expected in an occupation, given its age structure. The ratio of the observed to the expected number of deaths is multiplied by 100 to provide the SMR. An SMR higher than 100 indicates a greater risk in that occupation; values less than 100 suggest a lower than expected risk (e.g. an SMR of 150 means a 50% increase in risk relative to peers of the same age and gender in the population). We calculated SMRs for males and females separately because of the marked gender differences in suicide rates and variations in the proportion of men and women in different occupations. In this paper, we focus on occupations where there was statistical evidence that risk was higher or lower than that expected, as indicated by the range of the lower and upper 95% confidence intervals excluding 100. We restricted our analysis to occupations with at least 20 deaths.
Rates of unemployment and inactivity vary considerably by occupation. As death certificates may record the last occupation of the deceased if they were unemployed or inactive, levels of risk among occupations associated with high levels of unemployment or ill health may be overestimated, particularly as unemployment or disability are associated with increased risk of suicide.Reference Mäki and Martikainen10,Reference Jonsson, Alexanderson, Kjeldgård, Westerlund and Mittendorfer-Rutz11 To assess the impact of this on our findings, we conducted a sensitivity analysis using data from the UK's Annual Population Survey 2011–15 to estimate the number of employed, unemployed and economically inactive people aged 20–64 in each of the nine major occupational groups (https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/employmentandemployeetypes/methodologies/annualpopulationsurveyapsqmi). We re-estimated occupational SMRs after subtracting from total number of deaths in each occupational group/occupation the proportion (derived from the Annual Population Survey) that may have been unemployed or inactive. We used a similar approach to the specific occupations, but in the absence of reliable occupation-specific employment/inactivity rates, we applied the occupational group rates to all occupations within that group.
Results
Of the 18 998 suicide deaths among people aged 20–64 years between 2011 and 2015, 13 232 (70%) had an occupation recorded on the death certificate. The majority (10 688; 81%) of the suicides were among men. The main reason for the absence of a recorded occupation was that insufficient detail about the nature of the occupation was given by the person registering the death to enable occupational coding or the person did not have an occupation (74%); for the remaining 26% with missing data, the deceased was recorded as retired, permanently sick, unemployed, living by independent means or a student. Males were less likely than females to have no occupation recorded (70 v. 81% of all suicides); the mean age of those with missing occupation data was 40 years versus 44 years among those with occupational data.
Males
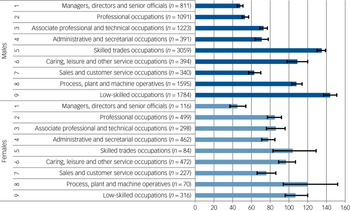
Three of the nine major occupation groups had statistically elevated risk of suicide (Fig. 1). The lowest risks were seen among managers, directors and senior officials. Low-skilled occupations (i.e. mostly involving routine tasks, often with the use of handheld tools and, in some cases, requiring a degree of physical effort) had the highest level of risk (SMR 144, 95% CI 137–151) and accounted for 17% of male suicide deaths where the occupation was stated. The highest level of risk among specific occupations in this group was seen in low-skilled construction workers (SMR 369, 95% CI 333–409); this occupation also had the highest risk among all individual occupations (Table 1).

Fig. 1 Suicide standardised mortality ratios for major occupation groups. Error bars show 95% confidence intervals; for females these are much wider due to the smaller number of deaths creating more statistical uncertainty. n details the number of deaths for each group.
Table 1 Suicide Standardised Mortality Ratios (SMRs) for specific occupations

For clarity we excluded individual occupations that specified ‘not elsewhere classified’ in the title.
a. We ranked occupations with at least 20 deaths.
b. Only six occupations among females had SMRs whose 95% CIs excluded 100.
The next major group with elevated risk was males working in skilled trades (SMR 135, 95% CI 130–139). This group also had the highest proportion of deaths, accounting for 29% of all male suicides (3059 out of 10 688). Skilled trades cover occupations whose tasks involve the performance of complex physical duties that normally require a degree of initiative, manual dexterity and other practical skills. The individual occupations within this group with the highest levels of risk were roofers, roof tilers and slaters (SMR 266, 95% CI 217–323) as well as building-finishing trades such as plasterers (SMR 234, 95% CI 188–287) and painters and decorators (SMR 204, 95% CI 177–233).
The final major group with elevated risk was males working as process, plant and machine operatives (SMR 108, 95% CI 103–114). Occupations with particularly high levels of risk within this group were metal working machine operatives (SMR 207, 95% CI 182–235) and forklift truck drivers (SMR 185, 95% CI 150–225).
Other specific occupations identified as being at high risk included call and contact centre occupations (SMR 290, 95% CI 204–399), window cleaners (SMR 224, 95% CI 170–291), farmworkers (SMR 221, 95% CI 165–289), bakers (SMR 205, 95% CI 135–298), fitness instructors (SMR 186, 95% CI 120–275) and refuse and salvage occupations (SMR 184, 95% CI 137–241).
Females
None of the major occupation groups showed statistical evidence of an increased risk of suicide in females; nevertheless, the broad patterns were like those seen in males, but the confidence intervals are wider due to the smaller number of deaths. The lowest risk is seen among managers, directors and senior officials; the highest risks are in process, plant and machine operatives, low-skilled occupations and skilled trades (Fig. 1). Six specific occupations were found to be at high risk (Table 1) with the highest risk seen among artists (SMR 399, 95% CI 244–616) and the greatest number of deaths (n = 231) occurring among care workers and home carers (SMR 170, 95% CI 149–194).
Occupations where there has previously been concern
Previous research has paid attention to occupations where the high risk of suicide is attributed to the occupation providing access to and/or knowledge about a method of suicide. One example is medical professionals, who have access to and knowledge of medicines. Among medical professionals, females had an elevated risk (SMR 124, 95% CI 109–141), whereas males had a lower risk (SMR 84, 95% CI 72–97). The elevated risk of suicide among females was largely explained by the high risk among nurses (SMR 123, 95% CI 104–145). For males, none of the individual health professions had significantly elevated risk: male doctors had a significantly lower risk (SMR 63, 95% CI 48–81), and the risk among male nurses was not different from that in the broader population (SMR 112, 95% CI 86–143).
In the past, there has been concern about males working in agricultural-related trades, particularly farmers. In this analysis, there was no evidence of an increased risk among male farmers (SMR 101, 95% CI 78–130); although, as discussed above, farmworkers (those responsible for rearing animals and harvesting crops) were at increased risk. It was only when looking at men working in agricultural trades more generally (e.g. farmers, gardeners) that there was evidence of an elevated risk (SMR 169, 95% CI 151–188), in part due to the elevated risk among gardeners (SMR 201, 95% CI 173–232).
Other occupations at increased risk
We identified several occupations at increased risk which have not previously been a major focus of concern. First, as well as finding a high risk of suicide among male (SMR 215, 95% CI 152–295) and female artists (SMR 399, 95% CI 244–616), we also found high risk among male musicians (SMR 252, 95% CI 189–328) and male actors, entertainers and presenters (SMR 241, 95% CI 176–322). Second, we found elevated risk of suicide among male (SMR 192, 95% CI 165–221) and female (SMR 170, 95% CI 149–194) care workers and home carers. This occupation concerns those who are paid to attend to the personal needs and comforts of the elderly and the infirm, providing care and support in residential care establishments, day care establishments and within people's homes. Finally, we found elevated risk of suicide among female nursery and primary school teachers (SMR 142, 95% CI 116–172). However, subsequent analysis of the text on death certificates has shown that this finding might be explained by the automatic coding of female teachers to this group when the information provided by the informant does not specify the school age taught (i.e. nursery v. primary v. secondary).
Sensitivity analysis
Taking account of occupational group differences in unemployment and inactivity had no major impact on our findings, although all SMRs were reduced. Among males, levels of unemployment and inactivity ranged from 8.3% in professional occupations to 22.8% in low-skilled occupations, and in females from 13.5% (professional) to 31.2% (low-skilled) (Table 2). Among males the highest risks were still seen among skilled trades (SMR 119, 95% CI 115–124) and low-skilled occupations (SMR 111, 95% CI 105–117) (Supplementary Table 1 available at https://doi.org/10.1192/bjp.2019.69). In females the highest risks were in process, plant and machine operatives (SMR 88, 95% CI 65–115) and skilled trades (SMR 81, 95% CI 62–103). The relative rankings of specific occupations remained largely unchanged but, for some occupations (vehicle valets and cleaners in males; bar staff, waitresses, primary and nursery education teaching professionals and nurses in females), the 95% confidence interval for the SMRs included 100 (Table 3).
Table 2 Proportion of people in England aged 20–64 years who were employed, unemployed or economically inactive by occupation group, 2011–2015

Estimates used annual data from the Annual Population Survey (Office for National Statistics) and are based on weighted population denominators that account for survey design and non-response. During the 5-year period, there was a total sample of 284 563 men and 294 632 women. The sample concerned those who provided information on their current main job (if employed at the time of interview) or last main job (if not employed at the time of interview). International Labour Organisation definitions of economic activity are used. Unemployed concerns those who are not currently in work but who are looking for work. Inactive concerns those who are not in work and not looking for work.
Table 3 Suicide Standardised Mortality Ratios (SMRs) for specific occupations, adjusted for economic inactivity

Table excludes deaths where the deceased may have been unemployed or economically inactive at the time of death.
Discussion
Main findings
There were marked variations in suicide risk between people in different occupations. For males, risks were highest among low-skilled workers and skilled manual workers, particularly those in construction-related jobs and among process, plant and machine operatives. Similar risks were seen in females, but only six specific occupations were associated with high risk – artists, bar staff, care workers, waitresses, primary and nursery teachers and nurses. In both males and females, managers, directors and senior officials had the lowest risk of suicide. Several occupations we identified as being at a heightened risk have not previously been highlighted in studies of occupational suicide – these include male and female care workers, people in creative occupations (artists, musicians and presenters), waitresses (females only), and call- and contact-centre workers (males only).
Comparison with earlier studies
There are several similarities between the present findings and those reported in previous studies. However, here it must be noted that differences between studies could, in part, be a product of the methods used, such as use of the PMR rather than SMR to compare risk. Furthermore, given that the classification of occupations changes over time, it is only possible to make broad comparisons.
Our findings are broadly in keeping with Meltzer et al's analysis of suicide by occupation in England and Wales based on deaths from 2001 to 2005: they also found that the highest risk of suicide was among skilled trades and lower-skilled jobs.Reference Meltzer, Griffiths, Brock, Rooney and Jenkins6 Recent studies have also identified a high risk of suicide among males in the construction industry, especially low-skilled construction workers.Reference Milner, Spittal, Pirkis and LaMontagne1 Contributors to risk in such jobs are likely to include low pay, low job security and other aspects of lower socioeconomic position.Reference Agerbo, Gunnell, Bonde, Mortensen and Nordentoft9,18 Other research has found that suicides in the construction industry may be preceded by high levels of alcohol consumption, relationship problems and multiple stressful life events in the months before death.Reference Heller, Hawgood and De Leo5,18 Whereas research from the 1980s and 1990s which used PMRs to estimate occupational suicide risk generally found an elevated risk of suicide among male healthcare professionals,Reference Kelly and Bunting7 more recent studies (using other approaches to estimate risk) show that this is no longer the case.Reference Roberts, Jaremin and Lloyd8,Reference Goldney12
Meltzer et al Reference Meltzer, Griffiths, Brock, Rooney and Jenkins6 found an elevated risk of suicide among male farmers. In our data, farmers were not at increased risk – a finding which may represent an improvement in this sector. Although some previous studies have reported a higher incidence of suicide among artists,Reference Meltzer, Griffiths, Brock, Rooney and Jenkins6,Reference Roberts, Jaremin and Lloyd8 few have identified an increased risk in this sector more widely (for example, artists, musicians and entertainers or presenters). Past research has found an association between creativity and psychiatric illness, such as bipolar disorder,Reference Simeonova, Chang, Strong and Ketter19 which could be a potential explanation of this finding; other possible explanations include greater employment/financial insecurity in this group and higher levels of substance misuse.
Our research also found that some occupations with everyday access to alcohol had increased risk, namely female bar staff and waitresses. The consumption of alcohol is a factor known to increase the risk of suicide.Reference Hufford20 An elevated risk of suicide was also found among carers (both males and females); to our knowledge, this has not been identified previously.
Limitations
There are several potential limitations to our study. First, occupation was not recorded for approximately a third of the suicide deaths. Missing data were more likely for females and younger individuals. It is possible that this missing data, if differential across different occupational groups, may lead to underestimation of risk in some occupations.
The occupational data used in this paper are taken from two separate sources. Occupation at the time of death is reported by the person registering the death and may not contain enough information to enable accurate occupation coding, whereas the distribution of occupations in the general population was self-reported and recorded in detail at the national census. An occupation recorded on the death certificate could also be based on an individual's last meaningful occupation if the deceased was out of work (e.g. due to retirement, being unemployed, being sick). The misalignment between data from two sources may result in numerator–denominator error, however our sensitivity analysis indicated that the ranking of SMRs in different occupational groups/occupations was largely unchanged when we accounted for differing levels of unemployment and inactivity between occupational groups.
We investigated risk in many occupational groups and individual occupations, and so it is possible that risks highlighted in some occupations, particularly those where risk estimates were based on relatively few deaths, may be chance findings. We reduced the likelihood of this occurring by only describing findings in occupations with at least 20 deaths.
Implications of the work
The work reported here gives an important insight into current patterns of occupational suicide in England, providing a foundation for targeted suicide prevention initiatives. Measures to reduce risk include training packages designed to address modifiable risk factors in the workplace (e.g. low control, monotony); these packages also help staff to identify and offer support to those who may be at high risk.Reference Milner, Page, Spencer-Thomas and LaMontagne21 Studies that have investigated the effectiveness of training programmes, such as ‘MATES in Construction’ in Australia, have shown they can result in increased knowledge on risk factors, stigma and help-seeking behaviours.Reference Milner, Page, Spencer-Thomas and LaMontagne21 Basic mental health training for managers has also been found to have a positive impact on employee's sickness absence.Reference Milligan-Saville, Tan, Gayed, Barnes, Madan and Dobson22 There is a need to evaluate such training programmes in UK settings.
The occupations with the highest number of suicide deaths among high-risk jobs were: low-skilled construction occupations (n = 380; 3.6% male deaths), metal working machine operatives (n = 239; 2.2% male deaths) and care workers and home carers (n = 185 males and n = 231 females; 1.7% and 9.1% of male and female deaths, respectively). These occupations could be considered the most promising targets for intervention.
Although our study indicates the relative risk of suicide for different occupational groups, the analysis does not provide any direct evidence concerning causation. For instance, although it is possible that certain factors associated with the job itself (e.g. stress, long hours, low pay) make suicide more or less likely, it could also be the case that people's characteristics, including their previous history or risk of mental illness, attract them to certain occupations. Further detailed research on deaths within occupational groups is needed to delineate explanations for observed patterns of risk.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjp.2019.69.
Funding
D.G. was supported by the National Institute for Health Research Biomedical Research Centre at University Hospitals Bristol National Health Service Foundation Trust and the University of Bristol. The views expressed in this publication are those of the author(s) and not those of the National Health Service, the National Institute for Health Research, the Department of Health and Social Care or the Office for National Statistics.
Acknowledgements
We thank Louis Appleby and Keith Hawton for their comments on a previous version of this work.






eLetters
No eLetters have been published for this article.