


1. Introduction
Political violence and terrorism, are increasingly being recognized as a major social threat worldwide. For instance, the 9/11 attacks in 2001 killed almost 3000 individuals, the London 7/7 bombings in 2005 resulted in 52 lethal victims, the Paris 13/11 attack (Bataclan) in 2015 killed 90 persons, while the Brussels 22/3 terrorist attacks in 2016 killed 32 people. The number of terrorism-related deaths increased by 80% in the years 2013–2014 [Reference Alcalá, Sharif and Samari1]. Apart from direct effects related to mortality, violent terrorist attacks aim to initiate fear and anxiety as well as lead indirectly to social diversion. These effects are widely related to several mental health outcomes, including PTSD, depression, anxiety disorders and substance use disorders [Reference Alcalá, Sharif and Samari1]. Sometimes mass shootings are described as terrorist incidents. Although various definitions are used to capture mass shooting, most commonly they are defined as an event with at least four people killed, not including the perpetrator [Reference McPhedran and Baker2]. In turn, terrorism refers to “the use of violence and intimidation in the pursuit of political aims” [Reference Dom, Schouler-Ocak, Bhui, Demunter, Kuey and Raballo3]. It follows that mass shootings that have political aims through violence or intimidation may indeed be considered forms of terrorism. Others may not be politically motivated but driven by personal grievances or anger. The groups claiming responsibility for terrorism attacks often refer to religious motivation to justify violent activity [Reference Ripley4], though other considerations underlying mass violence acts are also invoked, especially in case of lone-actor terrorism [Reference Rahman, Resnick, Harry and Breivik5].
The term radicalization has been proposed to describe the process, by which individuals adopt political, social and religious ideation that leads to the initiation of mass violence acts. According to recent conceptualizations, it is a multi-step process with mutually reinforcing stages [Reference McCauley and Moskalenko6]. Recognizing risk and protective factors through public health approaches has been proposed as a promising strategy for prevention of radicalization and mass violence [Reference Bhui, Hicks, Lashley and Jones7]. However, risk factors associated with radicalization remain largely unknown. To date, several social determinants have been proposed to promote radicalization, including low cultural integration, discrimination with subsequent sense of inequity and injustice, social disparities and low social cohesion or gang violence [Reference Alcalá, Sharif and Samari1, Reference McGilloway, Ghosh and Bhui8, Reference Victoroff9]. However, it should also be noted that social backgrounds of terrorist groups might change over time [Reference Strentz10]. A recent systematic review further revealed that radical engagement among European youths might be promoted by early experiences of abandonment, perceived injustice, personal uncertainty, family dysfunction, friendships with radicalized individuals and social changes [Reference Campelo, Oppetit, Neau, Cohen and Bronsard11]. It should be noted that social determinants of radicalization have been also related to several mental disorders [Reference Allen, Balfour, Bell and Marmot12]. In addition, mental health of perpetrators is widely commented in case of mass violence acts. However, caution should be taken on the way such causal inferences are being established. It has been reported that mass violence acts trigger fear and anger accompanied by small but significant increases in the stigmatization measures, such as feelings of unpredictability and dangerousness or less desire to help, towards individuals with mental disorders [Reference Von Dem Knesebeck, Mnich, Angermeyer, Kofahl and Makowski13–Reference Schomerus, Stolzenburg and Angermeyer15]. Moreover, there is a limited body of evidence for high prevalence rates of mental disorders among terrorists [Reference Dom, Schouler-Ocak, Bhui, Demunter, Kuey and Raballo3]. Terrorist groups might indeed be unlikely to wish to recruit individuals with mental disorders if this is perceived to risk their mission [Reference Bhui, James and Wessely16]. Moreover, it has been suggested that lone-actors and group terrorists might differ in terms of radicalization pathways, group dynamics and prevalence rates of mental disorders [Reference Corner, Gill and Mason17].
This limited body of evidence on the relationship between radicalization and mental health contrasts with the public media and some government actions suggesting violent (terroristic) acts are very frequently associated with perpetrators’ mental health status; this is then seen to be a consequence of failings in mental health systems [Reference DeFoster and Guns18]. This stigma-driven prejudgement frequently surfaces in the public eye where mental illnesses are equated with danger and violence. It is important that psychiatrists and mental health professionals are informed of the evidence on this complex problem, in order to help to inform the public opinion correctly and better shape their professions.
Factors associated with mental health that might predict mass violence incidents have not been subjected to qualitative synthesis. Therefore, in this article we aimed to perform a systematic review of studies addressing the relationship between mental health characteristics, radicalization and mass violence acts. We hypothesized that certain variables related to mental health status of personality traits may make individuals more prone to engage in mass violence acts. In addition, we assumed that lone actor terrorists and group terrorists might differ in terms of mental health characteristics, radicalization pathways and group dynamics.
2. Material and methods
2.1. Search strategy
Independent online search was performed by two reviewers and covered the following databases: MEDLINE/Pubmed, ERIC and Health Source: Nursing/Academic Edition from their inception until 8th Apr 2018. In addition, reference lists of eligible publications were reviewed. The following combination of keywords was used to retrieve eligible publications: mental or “psychiatr* or psychosis or delusion or paranoia or schizophr* or personality or depress* or suicid* or PTSD or substance abuse or addiction or bipolar or religious AND terrorism or mass violence or bombing or radicalization or lone-actor or lone-wolf or extremism”. Discrepancies regarding the inclusion of particular publications were resolved through discussion with the third reviewer (BM). We included the following publication records: 1) original studies investigating factors related to mental health (specific mental disorders, the measures of psychopathology and personality traits) with respect to radicalization proneness or resistance in terms of political authoritarianism, extreme religious beliefs or being in favour for violent activities; 2) case reports analysing mental health of perpetrators of mass violence acts and 3) articles written in the English language. The following exclusion criteria were used: 1) non-original publications (reviews, commentaries, editorials, perspectives and viewpoints); 2) case reports or case series; 3) studies addressing mental health outcomes of mass violence acts and 4) publications written in non-English language. Publication records based on overlapping samples were not excluded due to a variety of hypotheses tested in each publication. Our search strategy was developed in accordance with the PRISMA guidelines [Reference Moher, Liberati, Tetzlaff, Altman, Altman and Antes19].
2.2. Data extraction and quality assessment
The following data was extracted from original studies: sample size, age and sex of participants, study design, mental health assessment tools and main findings. For case reports, we recorded early signs in the radicalization process, mass violence acts in the context of radicalization and terrorism, participation in terrorism organization and activities as well as psychiatric diagnosis. Quality assessment was performed based on the SIGN grading system (1999–2012) that recognizes the following levels of evidence: 1++ - high quality meta-analyses, systematic reviews of randomized controlled trials, or randomized controlled trials with a very low risk of bias; 1+ - well-conducted meta-analyses, systematic reviews, or randomized controlled trials with low risk of bias; 1− - meta-analyses, systematic reviews, or randomized controlled trials with high risk of bias; 2++ - high quality systematic reviews of case control or cohort studies; 2+ - well conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal; 2− - case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal; 3 – non-analytic studies, e.g. case reports or case series and 4 – expert opinions [20].
3. Results
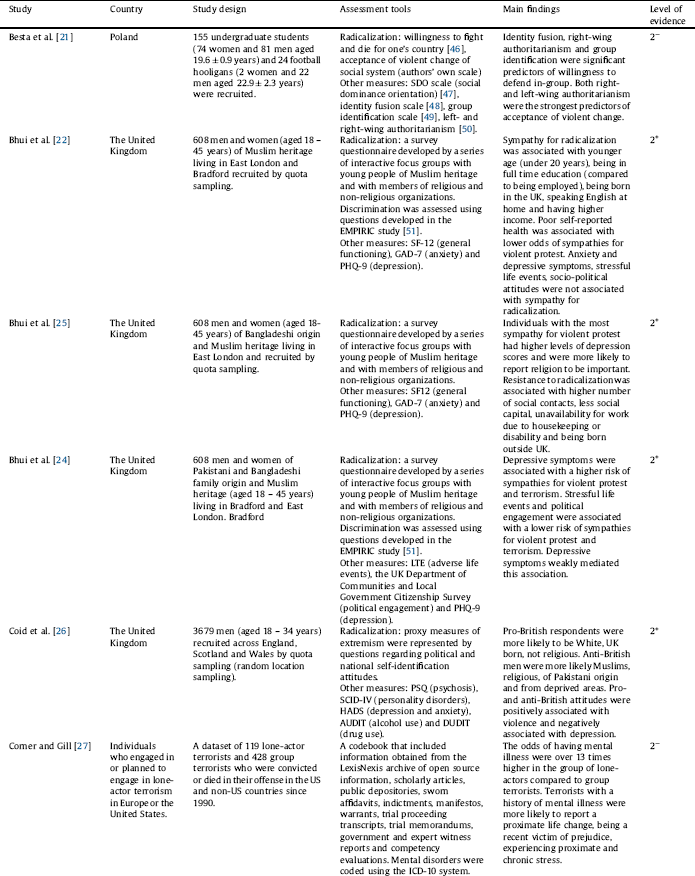
Out of 2768 records identified, 12 studies [Reference Besta, Szulc and Jaskiewicz21–Reference Soliman, Bellaj and Khelifa32] were found to be eligible for systematic review (Fig. 1). General characteristics of these studies and main findings were provided in Table 1. In the majority of studies, radicalization was measured using various self-administered questionnaires of attitudes toward ideology-based violence, political and national self-identification or political activism. One study was based on in-depth interviews with White supremacists [Reference Simi, Sporer and Bubolz31] and two studies applied the analysis open source information, scholarly articles, public depositories, sworn affidavits, indictments, manifestos, warrants, trial proceeding transcripts, trial memorandums, government and expert witness reports and competency evaluations [Reference Corner and Gill27, Reference Gill, Horgan and Deckert29]. Quality of evidence was scored 2+ in three studies [Reference Bhui, Warfa and Jones22, Reference Bhui, Everitt and Jones25, Reference Coid, Bhui, MacManus, Kallis, Bebbington and Ullrich26]. These studies recruited representative samples of Muslim participants [Reference Bhui, Warfa and Jones22, Reference Bhui, Everitt and Jones25] or the general population [Reference Coid, Bhui, MacManus, Kallis, Bebbington and Ullrich26]. In the majority of studies, quality of evidence was scored 2− mainly due to doubtful sample representativeness. One study provided only descriptive statistics based on life-history interviews (level of evidence: 3) [Reference Simi, Sporer and Bubolz31].
In the studies by Bhui et al. [Reference Bhui, Warfa and Jones22, Reference Bhui, Silva, Topciu and Jones24, Reference Bhui, Everitt and Jones25] performed in Muslim participants living in the UK, sympathies for radicalization were associated with the following factors: younger age, being in full education, being born in the UK, speaking English at home, having higher income, higher levels of depression and perceiving religion as an important aspect. In turn resistance to radicalization was predicted by higher number of social contacts, stressful life events, political engagement, less social capital, unavailability for work due to housekeeping or disability and being born outside UK. Depressive symptoms weakly mediated the effects of stressful life events and political engagement on sympathies for violent protest and terrorism. The role of depressive symptoms was also addressed in two other studies providing inconsistent findings. Indeed, the study of 3679 men recruited across England, Scotland and South Wales revealed that Pro-British and anti-British attitudes were both linearly associated with violence [Reference Coid, Bhui, MacManus, Kallis, Bebbington and Ullrich26]. However, both poles of political attitudes were negatively associated with scores of depressive symptoms. The role of depressive and anxiety symptoms in shaping radicalization was not confirmed in a small study of Palestinian refugee adolescents [Reference Victoroff, Quota, Adelman, Celinska, Stern and Wilcox23]. The authors found that greater support for religious-political violence was only related to the loss of family members in Israeli-Palestinian violent activities or feelings of being treated unjustly.

Fig. 1. The PRISMA flow diagram illustrating selection of studies.
Prevalence of mental disorders among subjects involved in terrorist activities were evaluated in three studies [Reference Corner and Gill27, Reference Gill, Horgan and Deckert29, Reference Simi, Sporer and Bubolz31]. The study by Simi et al. [Reference Simi, Sporer and Bubolz31] performed by means of life-history interviews with 44 former members of violent White supremacist groups demonstrated that mental health problems before or during extremism involvement as well as problems with alcohol or illicit drugs were present in 41% of participants. Suicidal ideation and family history of mental disorders were reported by 57% and 48% of extremists, respectively. However, some important limitations of this study should be taken into account, including a study design based on convenience sample, potential recall bias and a lack of using standardized tools for assessment of current and lifetime history of mental disorders. Similar limitations might be relevant to other publications [Reference Corner and Gill27, Reference Gill, Horgan and Deckert29] that addressed social and mental health characteristics of lone-actor terrorists. Both publications were based on the analysis of the same sample of 119 lone-actor terrorists. The authors found that the odds of having mental illness (ICD-10 codes F00 – F99) were over 13 times (OR = 13.49, 95%CI: 4.63–40.0) higher in lone-actor terrorists compared to group terrorists. Specific ICD-10 diagnoses were recorded based on extensive analysis of the Lexis Nexus database, sworn affidavits, indictments, manifestos, warrants, trail proceeding transcripts, trial memorandums, government and expert witness reports, and competency evaluations. Terrorists who injured in an attack were almost 12 times more likely to have a diagnosis of schizophrenia-spectrum disorders (F20 – F29) and almost 46 times more likely to be diagnosed with mood disorders (F30 – F39). Schizophrenia-spectrum disorders and mood disorders were also more likely in individuals, whose spouse or partner was involved in terrorism activities. Additionally, terrorists with a history of mental illness were more likely to report a proximate life change, being a recent victim of prejudice, experiencing proximate and chronic stress. Lone-actors confessing single-issue ideologies (animal rights, antiabortion and environmentalism) were significantly more likely to have a history of mental disorders compared to those holding other ideologies (right-wing-related or al-Qaeda-related ideology).
Table 1 General characteristics of original studies included in systematic review.


Abbreviations: ARIS – the Activism-Radicalism Intention Scale [Reference Moskalenko and McCauley56], AUDIT – the Alcohol Use Disorders Identification Test [Reference Babor57], BAI – the Beck Anxiety Inventory [Reference Beck, Epstein, Brown and Steer58], BAQ – the Buss Aggression Questionnaire [Reference Buss and Perry59], BDI – the Beck Depression Inventory [Reference Beck, Ward, Mendelson, Mock and Erbaugh60], CCI – the Cognitive Complexity Instrument [Reference Bagdasarov61], CSI – the Cognitive Style Index [Reference Allinson and Hayes62], DUDIT – the Drug Use Disorders Identification Test [Reference Berman, Bergman, Palmstierna and Schlyter63], FDS – the Frustration-Discomfort Scale [Reference Harrington64], GAD-7 – Generalized Anxiety Disorder Assessment [Reference Swinson65], HADS – the Hospital Anxiety and Depression Scale [Reference Zigmond and Snaith66], IUS-12 – the Intolerance of Uncertainty Scale – short form [Reference Freeston, Rhéaume, Letarte, Dugas and Ladouceur67], LTE – the List of Life Threatening Experiences [Reference Bebbington and Hurry68], NTB – the Need to Belong Scale [Reference Leary, Kelly, Cottrell and Schreindorfer69], PHQ-9 – the Patient Health Questionnaire [Reference Kroenke, Spitzer and Willams70], PSQ – the Psychosis Screening Questionnaire [Reference Bebbington and Nayani71], RDMS – the Radical Decision Making Scale [Reference Scott and R a72], SCATI – the Short Coolidge Axis II Inventory [Reference Coolidge, Segal, Cahill and Simenson73], SCID-IV – the Structured Clinical Interview for DSM-IV (personality disorders screening) [Reference Ullrich, Deasy, Smith, Johnson, Clarke and Broughton74], SF12 – the Short-Form Health Survey [Reference Ware, Kosinski and Keller75], TCI – the Temperament and Character Inventory [Reference Cloninger, Przybeck, Svrakic and Wetzel76].
In some studies, personality traits related to radicalization proneness were also addressed [Reference Besta, Szulc and Jaskiewicz21, Reference Feddes, Mann and Doosje28, Reference Laor, Yanay-Shani, Wolmer and Khoury30, Reference Soliman, Bellaj and Khelifa32]. Feddes et al. [Reference Feddes, Mann and Doosje28] investigated the effects of resilience training on own violent intentions and attitudes toward ideology-based violence in 46 Muslim adolescents with migrant background. The authors found that the training significantly increased the levels of agency and a marginal increase was found in reported self-esteem, empathy, perspective taking and narcissism. Attitudes toward ideology based violence and own violent intentions were significantly lower after the training. Higher levels of empathy were associated with less positive attitudes toward ideology-based violence. In two studies [Reference Besta, Szulc and Jaskiewicz21, Reference Laor, Yanay-Shani, Wolmer and Khoury30], factors associated with left- and right-wing authoritarianism were explored. In the study of undergraduate students and football hooligans, identity fusion, right-wing authoritarianism and group identification were significant predictors of willingness to defend in-group [Reference Besta, Szulc and Jaskiewicz21]. Both right- and left-wing authoritarianism were the strongest predictors of acceptance of violent change. Similarly, both poles of political extremism were associated with high level of ideological and morbid transcendence in the study by Laor et al. performed in a convenience sample of Israeli-Jewish participants [Reference Laor, Yanay-Shani, Wolmer and Khoury30]. Additionally, right-wing extremists had higher perceived threats to physical existence and national identity. Left-wing extremists scored highest on perceived moral integrity threat. Higher perceived threats to national identity and moral integrity, risk, and self-transcendence were associated with morbid transcendence. More complex associations were tested by Soliman et al. [Reference Soliman, Bellaj and Khelifa32], who examined several cognitive, behavioural and personality characteristics with respect to radicalization proneness in 662 Egyptian adults. On the basis of structural equation modelling, the authors found that a number of personality traits play a key role in radicalization. The most important predictors of radicalization included rational decision-making, dependent decision style, cognitive complexity, uncertainty and an analytical cognitive style. Radicalization was also associated with higher scores of paranoid personality disorder, self-defeating personality disorder and schizotypal personality disorder.
4. Discussion
Results of this systematic review indicate that a unique profile of psychopathology or personality traits that makes individuals more prone to radicalization cannot be proposed based on available evidence. Results of studies included in this review should be interpreted with caution taking into account a number of limitations. Firstly, these studies were mostly cross-sectional and thus causal associations between mental health status and radicalization proneness cannot be established. At this point, it is important to note that the extent of psychopathology might be different in individuals at various stages of radicalization process, including subjects in the development of extreme beliefs, early and late offenders or convicts. For instance, these differences might underlie discrepancies across studies testing the association between depressive symptoms and radicalization proneness. The use of various measures of radicalization might further complicate drawing unequivocal conclusions. Further, the majority of studies did not control for the effects of general criminality falling beyond radical ideation that might bias the association between mental health characteristics and radicalization. Another point is that mental health of participants was not assessed using standardized tools or only self-administered tools were used. Additionally, sample representativeness in some of these studies remains doubtful. Finally, in-depth interviews or self-reports that were used in some studies might also create recall biases.
There is some evidence from large population-based surveys that depressive symptoms might be related to radicalization proneness. However, studies addressing this association have provided mixed results. Cluster analysis performed by Bhui et al. in the study of Muslim participants living in the UK revealed that the participants being most sympathetic for violent protest had the highest scores of depressive symptoms [Reference Bhui, Everitt and Jones25]. However, a linear association with depressive symptoms was not found in neither of clusters capturing participants with various degrees of sympathies for violent protest (most condemning, intermediary group and most sympathetic for violence). A cross-sectional study design does not allow to infer regarding causality. Therefore, a steady or staged association should be also considered. At this point, it should be noted that depression shares overlapping characteristics with radicalization. A recent Swedish study comparing 47,158 outpatients with a diagnosis of depressive disorders and 898,454 individuals with a negative history of depression demonstrated three times higher odds (OR = 3.0, 95%CI: 2.8–3.3) of committing violent crimes in the depressed sample [Reference Fazel, Wolf, Chang, Larsson, Goodwin and Lichtenstein33]. Moreover, depression has been widely associated with a number of vulnerabilities that have been linked to radicalization in some studies, including social isolation and adverse life events [Reference Ge, Yap, Ong and Heng34, Reference Tennant35]. Finally, depression has been associated with high risk of suicide. In turn, the largest survey of 3679 men recruited across England, Scotland and Wales demonstrated that pro- and anti-British had been related to higher levels of violence but lower levels of depression [Reference Coid, Bhui, MacManus, Kallis, Bebbington and Ullrich26]. These findings imply that individuals with ambiguous or undecided views might be vulnerable to develop depressive symptomatology. The authors proposed that a lack of identity and uncertainty might serve as risk factors for depression. In other studies, the association between depression and radicalisation was not confirmed [Reference Bhui, Warfa and Jones22, Reference Victoroff, Quota, Adelman, Celinska, Stern and Wilcox23]. These discrepancies might be explained by several factors. Firstly, the relationship between depressive symptoms and radicalization has been addressed in various samples recruited by different methodological approaches, using various tools for assessment of depressive symptomatology. Secondly, a cross-sectional study design does not enable to establish causal inferences. Finally, it has long been argued that depression might have various clinical manifestations that cannot be comprehensively assessed using distinct instruments [Reference Goldberg36]. In addition, our understanding of affective symptomatology evolves with ongoing research in the field and changes of international classification systems. For instance, a new diagnosis of disruptive mood dysregulation disorder has been recently added in the DSM-5 for children and adolescents with persistent irritability accompanied by violent behaviours and depressive symptoms [Reference Copeland, Shanahan, Egger, Angold and Costello37]. Moreover, subthreshold depressive symptoms are also prevalent in a number of mental disorders, including personality disorders, that might contribute to violent behaviours. Finally, it seems important to understand whether suicide terrorists share similar mental health characteristics with others who commit “conventional” suicide [Reference Sela and Shackelford38].
Emerging evidence from studies included in this systematic review suggests that lone-actors and group terrorists might be two distinct groups of radicalized individuals in terms of mental health characteristics. According to studies based on a database of lone-actor terrorists [Reference Corner and Gill27, Reference Gill, Horgan and Deckert29], prevalence of mental disorders is significantly higher in this group of radicalized individuals, especially those motivated by single-issue ideologies, compared to group terrorists. This is in agreement with the observation that terrorism groups are reluctant to recruit individuals with a history of mental illness [Reference Dom, Schouler-Ocak, Bhui, Demunter, Kuey and Raballo3]. More specifically, the authors observed higher prevalence of schizophrenia-spectrum and affective disorders in lone-actors. Further, prevalence rates of various mental disorders in terrorist groups were compared to the general population data [Reference Corner, Gill and Mason17, 39]. These comparisons should be interpreted with caution as general population data comes from representative samples that were examined using valid assessment tools as opposed to data derived from terrorist groups. The analysis of descriptive statistics revealed that only schizophrenia, delusional disorder and autism-spectrum disorders might be more prevalent among lone-actors compared to the general population. Prevalence of all diagnostic categories of mental disorders was considerably lower among group terrorists than in the general population. Interestingly, the authors found no significant differences in criminality rates before terrorism acts between those with a history of mental illness compared to individuals without a psychiatric diagnosis [Reference Corner and Gill27]. This observation raises the question whether terrorism acts appear as the first manifestation of mental illness. In agreement with a number of previous studies [Reference Green, Girshkin, Teroganova and Quidé40], authors confirmed that terrorists with a history of mental illness had been more likely to be the victims of prejudice, and experience proximate and chronic stress. One study [Reference Simi, Sporer and Bubolz31] also revealed high prevalence rates of childhood adversities among group terrorists similar to those observed in patients with psychotic disorders [Reference Bonoldi, Simeone, Rocchetti, Codjoe, Rossi and Gambi41]. Although there are certain limitations of these studies, originating from a lack of head-to-head clinical assessment or selectivity bias associated with using open-source data, mental health of lone-actors warrants further investigation. The observation that lone-actors with single-issue ideologies might be more likely to present with higher rates of mental disorders compared to other lone-actor terrorists raises further questions whether there are differences in mental health characteristics between religious and secular groups or between ideologically-driven and grievance-driven terrorism [Reference Atran42].
Some studies revealed that certain personality traits might predispose to develop extreme beliefs. The following characteristics were associated with radicalization proneness: identity fusion, the need for group identification, low levels of empathy, morbid transcendence, feelings of being treated unjustly together with harbouring high levels of grievance, rational decision-making, dependent decision style, cognitive complexity, uncertainty and an analytical cognitive style [Reference Besta, Szulc and Jaskiewicz21, Reference Feddes, Mann and Doosje28, Reference Laor, Yanay-Shani, Wolmer and Khoury30, Reference Soliman, Bellaj and Khelifa32]. These findings indicate that radicalized individuals are aware of their decisions, analyse available information and are able to anticipate potential outcomes of violent acts. The study by Soliman et al. [Reference Soliman, Bellaj and Khelifa32] also revealed that radicalized individuals might have the traits of following personality disorders: paranoid personality disorder, self-defeating personality disorder and schizotypal personality disorder.
Due to several limitations and methodological heterogeneity addressing mental health correlates of radicalization process, caution should be taken on the way final conclusions are being established. Mental disorders, especially depression, are often evoked as direct causes of terrorism acts by mass media. A recent study Peterson et al. [Reference Peterson, Skeem, Kennealy, Bray and Zvonkovic43] demonstrated that out of 429 investigated crimes, only 4% were directly related to psychosis, 3% were directly related to depression and 10% were directly associated with bipolar disorder. Media coverage of terrorism evokes anxiety-inducing effects that appear to be desirable for terrorist groups [Reference Slone44]. However, an indirect effect related to increasing stigmatizing attitudes toward people with mental disorders should be also taken into account as shown in experimental studies [Reference Corrigan, Powell and Michaels45] and population-based surveys [Reference Von Dem Knesebeck, Mnich, Angermeyer, Kofahl and Makowski13–Reference Schomerus, Stolzenburg and Angermeyer15].
In summary, available data does not allow to indicate a predefined profile of mental health characteristics that makes individuals prone to develop radical beliefs and attitudes. Some personality traits might play a role but more research is needed in this field. There is some evidence that lone-actor terrorists, who often remain socially isolated, might present higher prevalence rates of some mental disorders compared to group-terrorists and the general population. The relationship with social isolation indicates that targeting at risk individuals might be achieved through the activity of community services. However, more studies taking into account methodological limitations raised in this systematic review are needed to address the effects of mental disorders on radicalization proneness. It is unlikely that mental disorders directly impact the development of radical ideation and thus investigating the processes or characteristics that mediate or moderate the effects of mental health problems should serve as an imperative in future studies. Translation of findings from this systematic review towards clinical practice remains difficult, mainly due to a scarcity of studies and methodological heterogeneity. However, reviewing current evidence in the field is a point of further debate within professional community that might shape individual opinion and decision making processes.
Conflict of interest
None to declare.
Acknowledgements
Authors are deeply grateful to Filip Stramecki (Department of Psychiatry, Wroclaw Medical University, Wroclaw, Poland) and Bartłomiej Stańczykiewicz (Department of Nervous System Diseases, Wroclaw Medical University, Wroclaw, Poland) for their support in online search.



Comments
No Comments have been published for this article.