



Myxomas are benign tumours derived from mesenchymal origin and account for about half of the benign cardiac tumours. Reference Yesodharan1 In the paediatric population, rhabdomyomas, teratomas, fibromas, and haemangiomas of the heart all are more common than myxomas, which account for only 2–4% of cardiac tumours. Reference McAllister2 Cardiac myxomas are known to cause neurological symptoms due to thromboembolic events and/or metastases to the brain. Reference Lee, Connolly and Brown3 Surgical resection is the treatment of choice. Reference Yesodharan1 Here we present a case of a 7-year-old male with history of high-risk neuroblastoma incidentally found to have cardiac myxoma at 1-year surveillance scan.
Case report
This is a 7-year-old male with history of stage IV high-risk neuroblastoma of the left adrenal gland, N-Myc non-amplified. He received intense therapy for neuroblastoma, which included chemotherapy (cyclophosphamide, topotecan, vincristine, doxorubicin, etoposide), I-131-Metaiodobenzylguanidine therapy, tandem autologous stem cell transplants, left adrenalectomy, proton beam therapy, immunotherapy with Anti-GD2 antibody (Dinutuximab), and Isotretinoin. During treatment, he also received Granulocyte-Macrophage Colony Stimulating Factor as well as Dexrazoxane.
A patent foramen ovale was noted on routine screening echocardiogram performed to assess cardiotoxicity from anthracycline therapy.
Physical exam was overall unremarkable except for pectus excavatum. His exam revealed proper growth with positive trend in his weight and height curves. Cardiac exam was unremarkable. On his routine one-year off-therapy CT scan of the chest and abdomen, he was found to have a 9 × 6 mm filling defect in the right atrium adjacent to the atrial septum. Subsequent transthoracic echocardiography was unable to visualise the mass. Transesophageal echocardiography revealed 8 × 6 mm echo-dense mass in the atrial septum, near the patent foramen ovale on the right side (Fig. 1). This study documented a finding most likely consistent with thrombus. He was started on therapeutic enoxaparin 1mg/kg twice daily dosing and thrombophilia workup was performed. Only lupus anticoagulant returned positive. EKG was normal. A three-month follow-up transthoracic echocardiogram was obtained, which revealed progression of the mass, now measuring 1.4 cm x 1.7 cm. This study revealed the lesion was more echobright than before, so there was uncertainty as to whether the lesion was truly larger or simply seen better with the increased echobrightness. Cardiac MRI showed a 16.3 × 11.3 mm pedunculated mobile mass attached to the right side of the atrial septum (Fig. 2). It had low signal on T1-weighted imaging and relatively high signal on T2-weighted imaging. There was a cleft of enhancement on first pass perfusion. Late gadolinium-enhanced sequences prescribed 10 minutes following administration of contrast demonstrate a cleft of central enhancement. The central enhancement made atrial thrombus less likely, as did progression of the lesion despite anticoagulation. An Metaiodobenzylguanidine diagnostic scan obtained also did not show abnormal uptake in the heart making it unlikely that the lesion was from neuroblastoma metastases. Tumour markers were within normal limits.
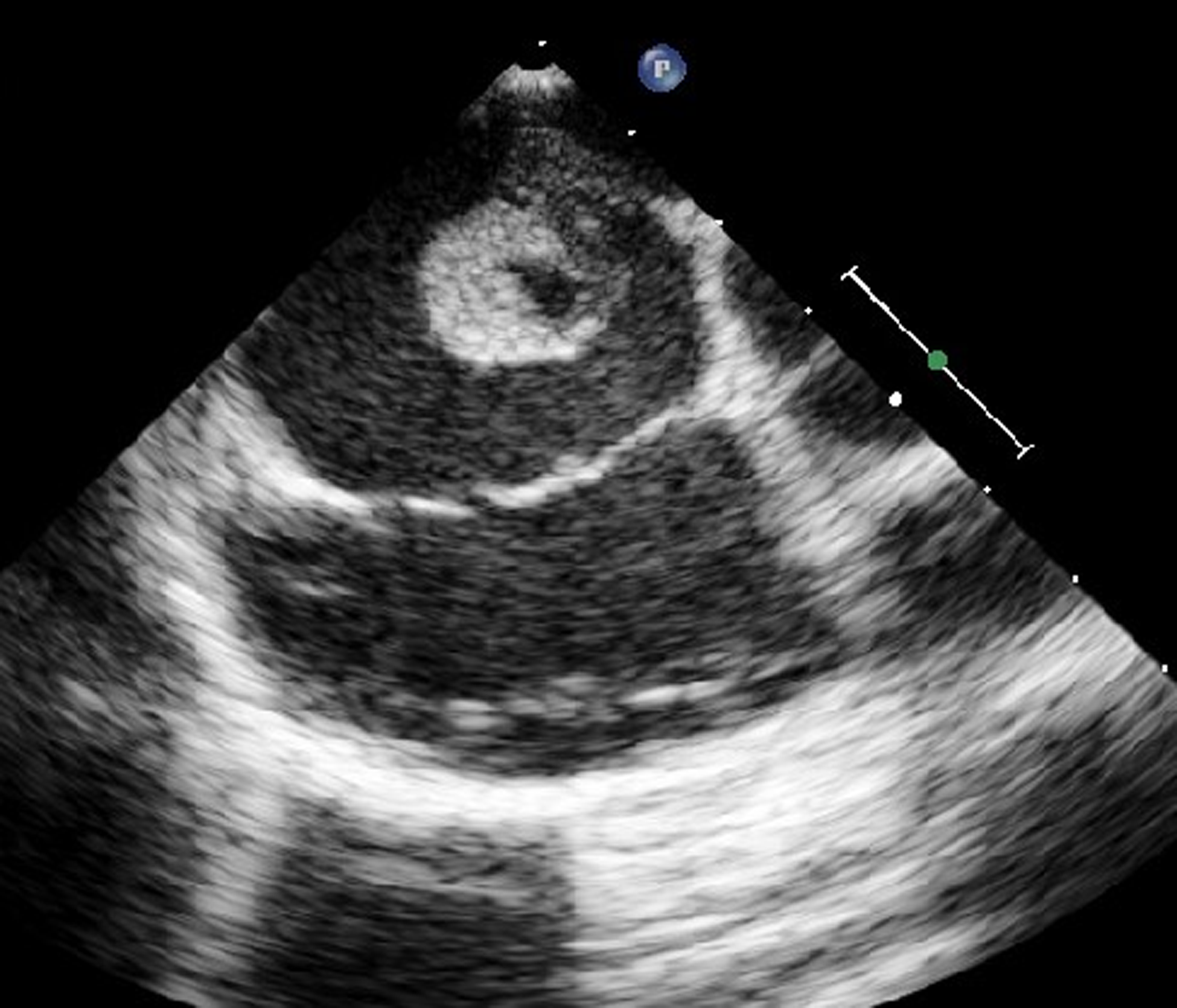
Figure 1. Transesophageal echocardiography showing an echo-dense pedunculated mass attached to the atrial septum.

Figure 2. Cardiac MRI showed a 16 × 11 mm pedunculated mobile mass attached to the right side of the atrial septum.
The patient underwent total atrial septectomy and atrial septal patch closure. Transesophageal echocardiography in the operating room showed the mass to be pedunculated and attached to the atrial septum on the right side of the septum. Flow cytometry was negative for malignancy. Pathology revealed 2 cm atrial myxoma. He was admitted to the cardiac ICU for monitoring and discharged home on post-operative day 2. He was prescribed 2 weeks of prophylactic dose enoxaparin at discharge given the association between thrombosis and myxoma.
Follow-up surface echocardiogram 2 weeks after discharge was without evidence of atrial mass or residual shunting lesion.
Discussion
Primary cardiac tumours in and of themselves are exceedingly rare with autopsy frequency reportedly ranging from 0.001 to 0.03%. Reference Yesodharan1 In the paediatric population, myxomas account for only 2–4% of cardiac tumours. Reference McAllister2 There is also a tendency for the cardiac myxoma to be most located in the left atrium in up to 75% of cases, close to 18% of cases in the right atrium, and 7% within the ventricles. Reference Yesodharan1 Familial cases are less common, occurring in up to 10% of cases (Carney syndrome). Reference Yesodharan1 Myxomas are usually pedunculated and attached to the atrial septum. Symptoms could be due to atrioventricular valve obstruction or embolic events. Myxomas typically are visualised by surface echocardiography, however further imaging with CT chest and cardiac MRI can be utilised to locate the lesion with more specific characteristics if needed. Surgical resection is curative and the treatment of choice. Sudden death in untreated patients can occur in up to 15% of the patients due to embolisation or atrioventricular valve obstruction. It is important to know that recurrence is relatively common, reported in 5% of sporadic cases and in up to 20% of familial cases in the first six years following surgical resection. Reference Yesodharan1 Some report at least annual surveillance surface echocardiogram and others every 6 months to monitor recurrence. Reference Grant, Rhee and Tracy4
Exposure to chemotherapy and radiation increases risk for second malignant neoplasms in childhood cancer survivors. Reference Cohen, Curtis, Inskip and Fraumeni5 Hence, the finding of a lesion in the heart raises concern for secondary neoplasm or metastases necessitating detailed oncology and cardiac workup as described in our young patient. Hill et al reported an incidental case of cardiac myxoma in a child with neuroblastoma as well but after 5.5 years of being off therapy who also survived after complete resection of the tumour. Reference Hill, Castellino and Williams6
Due to the possibility of cardiac myxoma embolism and the risk of sudden death, surgery should be performed as soon as possible once cardiac myxoma is diagnosed to remove as much of the tissue surrounding the tumour as possible and reduce the recurrence rate. Reference Tao, Yahyavi-Firouz-Abadi, Singh and Bhalla7
In conclusion, our case describes incidental finding of cardiac lesion in a child with neuroblastoma that mimicked a cardiac thrombus at initial finding. Subsequent follow-up revealed enlarged lesion raising concern for cardiac tumour triggering detailed cardiac and oncology workup. Multidisciplinary involvement and vigilance are crucial for management of rare cases such as our patients.
Acknowledgements
We would like to thank the patient and family for allowing us to publish his case.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
None.
Ethical standards
None.



 Open access
Open access