



Refugee crisis
Approximately 79.5 million individuals worldwide have been forcibly displaced.1 Of these, 45.7 million have been displaced internally, 29.6 million have been externally displaced and 4.2 million are seeking asylum. Forced displacement typically follows human rights violations, conflict, persecution or events causing serious public disorder, with refugees and asylum seekers experiencing ‘complex traumas’.
Complex trauma
Complex traumas are characteristically interpersonal in nature (i.e. are perpetrated deliberately by other people) and involve repeated prolonged and often multiple traumatic exposures between victim and perpetrator(s). The victim has typically been held in conditions from which they are unable to escape, because of physical, maturational, social, family/environmental or psychological constraints.Reference Herman2 Refugees and asylum seekers often report experiencing direct exposure to multiple types of complex traumatic experiences,Reference Teodorescu, Heir, Hauff, Wentzel-Larsen and Lien3 including sexual violence, torture, imprisonment, enforced isolation, physical assault, and the murder of friends or family members.Reference Liddell, Nickerson, Felmingham, Malhi, Cheung and Den4 In addition to pre-migration traumas experienced in the individuals’ countries of origin, traumatic events can also be experienced during forced migration journeys,Reference Beiser5, Reference Phillimore6 for instance, at the hands of human smugglers or traffickers or in refugee camps. This can result in trauma-related mental health disorders.Reference Bogic, Njoku and Priebe7
Complex post-traumatic stress disorder
In response to the observation that complex trauma can lead to mental health sequalae not adequately captured by prevailing diagnostic formulations of post-traumatic stress disorder (PTSD), HermanReference Herman2 in 1992 proposed the term complex PTSD (CPTSD). PTSD typically follows single traumatic events that need not be interpersonally caused, such as natural disasters and accidents.Reference Breslau, Davis, Andreski and Peterson8 However, individuals with experiences of complex trauma (particularly in the context of coercive control) may experience symptoms more varied and severe than the intrusion, avoidance and hyper-arousal symptoms classically associated with PTSD.
Enduring personality change after catastrophic events (EPCACE) was included in the ICD-109 to capture the personality changes which can follow catastrophic stressors. Single traumatic events not interpersonal in nature are excluded as possible catastrophic stressors. A diagnosis of EPCACE requires personality changes attributed to trauma to last for a minimum of 2 years and can involve a mistrustful or hostile attitude towards the world, social withdrawal, persistently feeling hopeless or empty, estrangement and continuously feeling on edge.9 The criteria have been criticised for being overinclusive, with this diagnosis underutilised in both research and clinical settings.Reference Beltran and Silove10
The DSM-IV11 included an equivalent symptom group referred to as disorder of extreme stress not otherwise specified (DESNOS). Core features of DESNOS include changes in sustaining beliefs, impulse and affect regulation, somatisation, self-perception, relationships with others and dissociation. DESNOS was viewed only as a symptom group within PTSD, as field trials indicated that almost all participants meeting DESNOS criteria also met PTSD criteria.Reference Roth, Newman, Pelcovitz, van der Kolk and Mandel12
The diagnostic category of CPTSD has been incorporated into the ICD-1113 as a separate disorder to PTSD. It consists of symptom clusters involving disturbances in self-organisation (DSO) in addition to the classical PTSD clusters of intrusion, avoidance, and hyper-arousal. The DSO symptom clusters include affective dysregulation, disturbances in relational function and negative self-concept. In addition, CPTSD requires endorsing additional symptoms indicating functional impairment. CPTSD reflects the depletion of social, psychological and emotional resources resulting from protracted conditions of trauma,Reference Cloitre, Garvert, Brewin, Bryant and Maercker14 leading to greater functional impairment than PTSD.
CPTSD, EPCACE and DESNOS have some overlapping symptoms. All three attempt to capture the more varied mental health sequalae that follow complex trauma. However, the diagnostic conceptualisations are not identical (Fig. 1). Unlike DESNOS, ICD-11 CPTSD is a diagnostic category distinct from PTSD, and unlike EPCACE, CPTSD criteria do not include personality change.
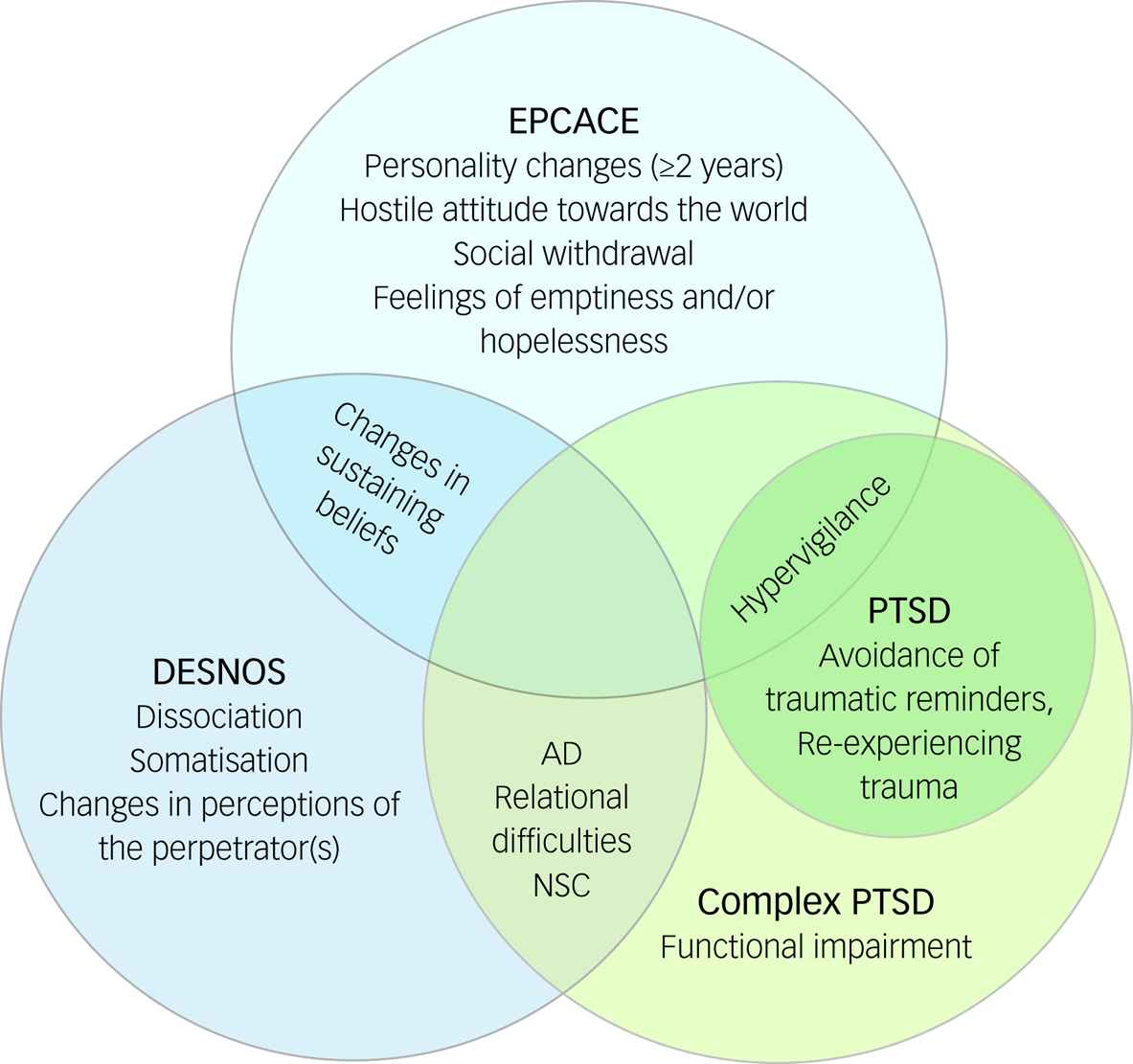
Fig. 1 Overlaps and differences among definitions of enduring personality change after catastrophic events (EPCACE), disorder of extreme stress not otherwise specified (DESNOS), complex post-traumatic stress disorder (PTSD) and ICD-11 PTSD. AD, affective dysregulation; NSC, negative self-concept.
The applicability of CPTSD symptomatology has been demonstrated in various trauma samples, including individuals who have suffered childhood physical or sexual abuse,Reference Cloitre, Garvert, Brewin, Bryant and Maercker14 former prisoners of warReference Zerach and Solomon15 and institutional abuse survivors.Reference Knefel, Garvert, Cloitre and Lueger-Schuster16 Although refugees and asylum seekers are a highly traumatised population, less is known about the prevalence of CPTSD in this population. The increase in the number of forcibly displaced people requiring resettlement in recent years requires physicians and health service providers to be aware of the mental disorders prevalent in this population. Treatment needs for PTSD and DSO symptoms may differ; research indicates that solely trauma-focused treatment can overwhelm those who have suffered complex trauma,Reference Herman17 with a phased treatment approach required instead.Reference ter Heide, Mooren and Kleber18 An understanding of the current prevalence of CPTSD in this population (and the associated treatment implications) is therefore highly important.
ter Heide et alReference ter Heide, Mooren and Kleber18 have reported findings of an unpublished systematic review of five studies that used validated measures to assess the prevalence of DESNOS among refugees. The review incorporated two non-treatment-seeking and three treatment-seeking refugee populations displaced internally and externally. Relative to a diagnosis of DESNOS, no diagnosis or a PTSD diagnosis was more likely. They concluded that the more severe DESNOS symptoms should not be assumed to occur in a population because of the presence of complex traumatic experiences. However, the authors acknowledged that their conclusions were based on the limited evidence available at the time.Reference ter Heide, Mooren and Kleber18 This review also pre-dated the introduction of ICD-11 CPTSD, and there has since been an expansion in the literature examining this disorder among refugee and asylum-seeking populations.
A recent systematic review by Mellor et alReference Mellor, Werner, Moussa, Mohsin, Jayasuriya and Tay19 also reported the prevalence of CPTSD, DESNOS and EPCACE in samples of refugees and displaced individuals, and further examined predictors of CPTSD and the associations between CPTSD and common mental disorders. The results demonstrated a wide range of CPTSD prevalence among studies, with authors positing this to reflect geographic and contextual factors.Reference Mellor, Werner, Moussa, Mohsin, Jayasuriya and Tay19 However, not all of the included studies examining CPTSD followed ICD-11 CPTSD diagnostic criteria or used diagnostic tools specific to ICD-11 CPTSD to diagnose participants. Furthermore, not all studies consisted of forcibly displaced samples. There remains the need for further synthesis of data on the prevalence of CPTSD, EPCACE and DESNOS among refugees and asylum seekers in treatment-seeking and population samples. An updated systematic review examining this is therefore timely.
Aims and method
This systematic review provides an estimate of the prevalence of CPTSD among adult refugee and asylum-seeking samples. The term ‘refugees’ refers to individuals forcibly displaced internally within their country of origin or externally displaced in a foreign country.
The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42020188422, https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=188422). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was followedReference Moher, Liberati, Tetzlaff and Altman20 (see Supplementary Appendix 3 available at https://doi.org/10.1192/bjo.2021.1013).
Criteria for study inclusion
Eligible studies were required to include samples of refugees and/or asylum seekers of any ethnicity who were over 18 years of age at the time measures were administered. The use of validated or standardised diagnostic methods specific to the diagnoses of ICD-11 CPTSD, ICD-10 EPCACE or DSM-4 DESNOS to provide the corresponding diagnoses was also required, as was reporting of the prevalence of CPTSD, EPCACE or DESNOS within the refugee and/or asylum-seeking samples. As sampling biases are more likely in smaller samples,Reference Fazel, Wheeler and Danesh21 only studies with a sample size greater than 50 were considered eligible. When numerous articles reported the same data from the same sample, the earliest publication was used.
Search strategy
The electronic databases PsychINFO, Embase, Medline, EBSCO and ProQuest PTSDpubs, a database specifically for PTSD and trauma literature, were searched from the time of their inception to 25 March 2020. A final search of these databases was conducted on 8 Jan 2021 to capture any studies published after the first search.
The search terms consisted of terms relating to refugees, asylum seekers, CPTSD, DESNOS and EPCACE. Full search strategies for all databases are provided in Supplementary Appendix 1. The reference lists of studies eligible for inclusion in the review were manually searched by the first author for further relevant studies not captured by the systematic searches. None were found.
Study selection
The identification of studies followed procedures outlined by PRISMA.Reference Liberati, Altman, Tetzlaff, Mulrow, Gøtzsche and Ioannidis22 Titles and abstracts were initially screened by U.D.S. for articles deemed potentially relevant. Following this, all authors independently reviewed the full texts of each study to establish whether they were eligible for inclusion. All authors then discussed the final studies to be included.
Data extraction
Data were first extracted on 3 July 2020 and recorded in a tabular form including sample setting; time spent in host country; mean age and age range; measurement tools used to assess CPTSD, EPCACE and DESNOS; measurement tools used to assess additional diagnoses; diagnostic criteria used for diagnosing CPTSD, EPCACE and DESNOS, and additional disorders assessed; and the prevalence of CPTSD, EPCACE and DESNOS, and other diagnoses assessed. Additional study characteristics extracted were gender breakdown, age statistics and duration spent in the host country.
Synthesis and analysis of data
The heterogeneity among the study designs, methods, populations and the reported effect estimates in the eligible studies did not allow for meta-analysis. Consequently, a narrative synthesis was conducted to synthesise findings. The point prevalence of CPTSD, EPCACE and DESNOS among study samples was described and compared. Owing to the expected disparity in the prevalence estimates between treatment-seeking and population samples, these groupings are presented separately. Studies were also grouped by diagnostic system used. Where possible, the prevalence rates of the disorders of interest among refugee and asylum-seeking samples were compared with the prevalence of other diagnoses assessed within the same samples.
Risk of bias assessments
The Joanna Briggs Institute Critical Appraisal Checklist for Prevalence Data23 was used to assess the methodological quality of each individual study. This considers nine domains: suitability of the sample frame; appropriateness of participant recruitment; sample size sufficiency; adequacy of the setting and participant description; adequacy in reporting the sample; validity of the diagnostic measures; suitability of the statistical analyses; and adequacy of the response rates. The majority view among all authors for each criterion was used.
Results
Overview of study selection
A flowchart of the study selection process is shown in Fig. 2. The systematic searches of the six electronic databases identified 2355 results, from which the titles and abstracts of 1402 studies were assessed for eligibility. Of these, 40 records were considered eligible for full-text screening. In the second stage of screening, 25 records were excluded. Fifteen studies were found to be eligible and were included in the review, 14 of which were found in the searches conducted on 25 March 2020, with the remaining study found in the second search on 8 January 2021. Of the included studies, ten assessed CPTSD, three assessed DESNOS and two assessed EPCACE.

Fig. 2 PRISMA flowchart depicting study selection based on searches conducted on 25 March 2020 and 8 January 2021. PTSD, post-traumatic stress disorder.
Study characteristics are detailed in Supplementary Appendix 2. The mean sample size per study was 258.4 (range 61–1200), with a total sample size of 3876 measuring CPTSD. All studies were conducted in the countries hosting the refugees. Eight were conducted in Europe, two in the Middle East, three in Oceania, one in Africa and one in the USA. The time spent in the host country at the time measures were administered varied within and between samples, with means ranging from 11.1 months to 27 years across studies. Data for time spent in the host country were unavailable for seven studies.
Prevalence of CPTSD in treatment-seeking samples
Ten studies used treatment-seeking samples, with the prevalence of CPTSD, DESNOS or EPCACE ranging from 16 to 66.9% (Fig. 3). The point prevalence of CPTSD was measured in six studies (Table 1). A CPTSD prevalence of 21.3% was reported in a culturally diverse refugee sample resettled in Switzerland.Reference Hecker, Huber, Maier and Maercker28 In a sample of Syrian refugees living in Lebanon, a CPTSD prevalence of 36.1% was found,Reference Hyland, Ceannt, Daccache, Abou Daher, Sleiman and Gilmore29 and a prevalence estimate of 66.9% was reported in a culturally diverse refugee sample in Denmark.Reference Vang, Nielsen, Auning-Hansen and Elklit36 One studyReference Liddell, Nickerson, Felmingham, Malhi, Cheung and Den4 investigating a culturally diverse sample of refugees resettled in Sydney, Australia, reported a CPTSD prevalence estimate of 29.5%. In a study investigating a sample of African refugees residing in Italy, a prevalence of 30% was reported.Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24 Nickerson et alReference Nickerson, Cloitre, Bryant, Schnyder, Morina and Schick31 reported a prevalence of 32.8% in a culturally diverse refugee and asylum-seeking sample in Switzerland.

Fig. 3 Prevalence of complex post-traumatic stress disorder (PTSD), enduring personality change after catastrophic events (EPCACE) and disorder of extreme stress not otherwise specified (DESNOS) in treatment-seeking and population samples.
Table 1 Point prevalence of complex post-traumatic stress disorder (CPTSD) in included studies

PCL-5, PTSD Checklist for DSM-5 (PCL-5); DSO, disturbances in self-organisation; ITQ, International Trauma Questionnaire; AD, affective dysregulation; NSC, negative self-concept; DR, disturbances in relational function; SIDES, Structured Interview for Disorders of Extreme Stress; AUDADIS-IV, Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV; EPCACE, enduring personality change after catastrophic events; DERS, Difficulties in Emotion Regulation Scale; ECR, Experiences in Close Relationships Scale; PDS, Posttraumatic Diagnostic Scale; SIDES-SR, Self-Report Inventory for Disorders of Extreme Stress; R-MHAP, Refugee-Mental Health Assessment Package.
Two studies reported prevalence estimates of DESNOS. In a culturally diverse sample of refugees in Norway, a point prevalence of 16% was reported.Reference Teodorescu, Heir, Hauff, Wentzel-Larsen and Lien3 Another study looked at a sample of Bosnian former refugees in Denmark, finding a prevalence of 34%.Reference Palic and Elklit32
Two studies measured EPCACE in samples of culturally diverse refugees resettled in Denmark, reporting point prevalence estimates of 49.5Reference Rathke, Poulsen, Carlsson and Palic33 and 24.2%.Reference Mundy, Foss, Poulsen, Hjorthoj and Carlsson30
Prevalence of CPTSD in population samples
Five studies used population samples, with prevalence ranging from 2.2 to 50.9%. Four measured CPTSD. Grossman et alReference Grossman, Hoffman, Shrira, Kedar, Ben-Ezra and Dinnayi27 reported a prevalence of 50.9% in recently liberated female Yazidi captives resettled in camps in Kurdistan. In separate samples of West Papuan refugees residing in settlements in Papua New Guinea, prevalence rates of 9.3Reference Silove, Rees, Mohsin, Tam, Kareth and Tay34 and 3%Reference Tay, Rees, Chen, Kareth and Silove35 were reported. One studyReference Frost, Hyland, McCarthy, Halpin, Shevlin and Murphy26 investigated a culturally diverse sample of refugees in the USA, reporting a prevalence of 4.9%.
One study measured the prevalence of DESNOS in a sample of Ethiopian refugees in Eritrean refugee shelters and found it to be 2.2%.Reference de Jong, Komproe, Spinazzola, van der Kolk and Van Ommeren25
EPCACE was not measured in any population sample of refugees and/or asylum seekers.
Prevalence of additionally measured diagnoses relative to CPTSD, DESNOS and EPCACE
Treatment-seeking samples
ICD-11 PTSD prevalence was measured in six studies (Fig. 4). Two reported higher ICD-11 PTSD prevalence (38 and 32.9%, respectively) compared with CPTSD (30 and 21.3%, respectively).Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24, Reference Hecker, Huber, Maier and Maercker28 Four studies reported lower ICD-11 PTSD prevalence estimates compared with CPTSD.Reference Liddell, Nickerson, Felmingham, Malhi, Cheung and Den4, Reference Hyland, Ceannt, Daccache, Abou Daher, Sleiman and Gilmore29, Reference Nickerson, Cloitre, Bryant, Schnyder, Morina and Schick31, Reference Vang, Nielsen, Auning-Hansen and Elklit36

Fig. 4 Prevalence of the most frequently measured additional diagnoses of DSM-5 post-traumatic stress disorder (PTSD) and ICD-11 PTSD compared with complex PTSD in treatment-seeking and population samples.
One study measured DSM-5 PTSD, reporting a higher prevalence estimate of 79% compared with a CPTSD prevalence of 30%Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24. One study reported prevalence estimates of 82% for DSM-IV PTSD, 71% for major depressive disorder (MDD), 31% for generalised anxiety disorder (GAD), 41% for panic disorder, 49% for dysthymia, 0% for hypomania, 49% for agoraphobia, 49% for social phobia, 44% for obsessive–compulsive disorder, 10% for alcohol abuse disorder, 36% for nicotine dependence and 5% for bulimia, compared with 16% for DESNOS.Reference Teodorescu, Heir, Hauff, Wentzel-Larsen and Lien3 Rathke et al reported prevalence estimates of 2.6% for ICD-10 PTSD, 49.5% for ICD-10 PTSD and comorbid EPCACE, 43.9% for ICD-10 PTSD with secondary psychotic features (PTSD-SP) and comorbid EPCACE, 25.8% for ICD-10 and comorbid depression, and 4.2% for ICD-10 PTSD-SP without comorbid depression, relative to 49.5% for EPCACE.Reference Rathke, Poulsen, Carlsson and Palic33
One studyReference Mundy, Foss, Poulsen, Hjorthoj and Carlsson30 reported a prevalence estimate of 93.8% for ICD-10 depression and 33.2% for other diagnoses, relative to a lower EPCACE prevalence estimate of 24.2%, in a sample of refugees with existing diagnoses of ICD-10 PTSD.
Population samples
ICD-11 PTSD was measured in three studies, with the prevalence ranging between 6 and 21.3%. Two studies reported greater ICD-11 PTSD prevalence estimates (20.9 and 13%) relative to CPTSD (4.9 and 3%),Reference Frost, Hyland, McCarthy, Halpin, Shevlin and Murphy26, Reference Tay, Rees, Chen, Kareth and Silove35 with the remaining study reporting a lower PTSD prevalence estimate (21.3%) compared with CPTSD (50.9%).Reference Grossman, Hoffman, Shrira, Kedar, Ben-Ezra and Dinnayi27 DSM-5 PTSD was assessed in two studies, with prevalence estimates of 12Reference Tay, Rees, Chen, Kareth and Silove35 and 12.1%Reference Silove, Rees, Mohsin, Tam, Kareth and Tay34 reported; DSM-5 PTSD prevalence estimates were higher than CPTSD prevalence in both studies. One studyReference Tay, Rees, Chen, Kareth and Silove35 reported prevalence estimates of 13% for DSM-IV PTSD and 13% for ICD-10 PTSD, whereas the CPTSD prevalence was 3%. Another studyReference Silove, Rees, Mohsin, Tam, Kareth and Tay34 reported prevalence estimates of 56.2% for MDD, 26.5% for GAD, 8% for panic disorder, 9.9% for persistent complex bereavement, 9.9% for separation anxiety disorder and 5.6% for intermittent explosive disorder, compared with 9.3% for CPTSD.
Methodological quality
Risk of bias assessments for all studies are presented in Table 2. Two studies used samples drawn through random selection.Reference de Jong, Komproe, Spinazzola, van der Kolk and Van Ommeren25, Reference Frost, Hyland, McCarthy, Halpin, Shevlin and Murphy26 Two studies attempted to sample the entire population of eligible refugees.Reference Silove, Rees, Mohsin, Tam, Kareth and Tay34, Reference Tay, Rees, Chen, Kareth and Silove35 One study used a consecutively drawn sample.Reference Vang, Nielsen, Auning-Hansen and Elklit36 The sampling methods in the remaining ten studies were unclear or non-random.
Table 2 Methodological quality of included studies assessed using the Joanna Briggs Institute Critical Appraisal Checklist for Prevalence Studies23

Y, Yes; N, No; U, Unclear.
The samples used in two studies were drawn from census data of refugees living in selected settlements.Reference Silove, Rees, Mohsin, Tam, Kareth and Tay34, Reference Tay, Rees, Chen, Kareth and Silove35 One studyReference de Jong, Komproe, Spinazzola, van der Kolk and Van Ommeren25 drew its sample from a list of registered displaced individuals, one studyReference Frost, Hyland, McCarthy, Halpin, Shevlin and Murphy26 used a subsample selected from a randomly drawn and nationally representative sample of US non-institutionalised adults, and one studyReference Grossman, Hoffman, Shrira, Kedar, Ben-Ezra and Dinnayi27 drew its sample from post-liberation camps. The remaining ten studies drew samples from treatment centres.Reference Teodorescu, Heir, Hauff, Wentzel-Larsen and Lien3, Reference Liddell, Nickerson, Felmingham, Malhi, Cheung and Den4, Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24, Reference Hecker, Huber, Maier and Maercker28–Reference Rathke, Poulsen, Carlsson and Palic33, Reference Vang, Nielsen, Auning-Hansen and Elklit36
As they were not stated in any of the included studies, the required sample sizes for prevalence estimates for treatment-seeking and population samples were calculated using the following formulaReference Naing, Winn and Rusli37: $n = {{Z^2P( {1-P} ) } \over {d^2}}$ , where n is the sample size, Z is the level of confidence statistic, P is the anticipated prevalence and d is the precision. Expected CPTSD prevalence estimates of 31.4% in treatment-seeking samples and 4.9% in population samples were assumed by calculating the median values of the reported prevalence estimates within these two sample types. Median values were used owing to the variability in prevalence estimates among studies, so as to reduce sensitivity to outliers. In addition, 95% confidence intervals and 5% precision were used in sample size calculations for both treatment-seeking and population samples. Required sample sizes for treatment-seeking and population samples were 331 and 72, respectively. Thus, sample sizes were insufficient in all ten studies with treatment-seeking samples but were sufficient for studies with population samples.
, where n is the sample size, Z is the level of confidence statistic, P is the anticipated prevalence and d is the precision. Expected CPTSD prevalence estimates of 31.4% in treatment-seeking samples and 4.9% in population samples were assumed by calculating the median values of the reported prevalence estimates within these two sample types. Median values were used owing to the variability in prevalence estimates among studies, so as to reduce sensitivity to outliers. In addition, 95% confidence intervals and 5% precision were used in sample size calculations for both treatment-seeking and population samples. Required sample sizes for treatment-seeking and population samples were 331 and 72, respectively. Thus, sample sizes were insufficient in all ten studies with treatment-seeking samples but were sufficient for studies with population samples.
Two studies developed measures consisting of items from several scalesReference Frost, Hyland, McCarthy, Halpin, Shevlin and Murphy26, Reference Nickerson, Cloitre, Bryant, Schnyder, Morina and Schick31 but did not validate them. One used items representing DSO clusters from a PTSD scale but reported good internal consistency (Cronbach's α = 0.81).Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24 Another used unvalidated precursors to the International Trauma Questionnaire but reported good and high internal consistency for both within the sample (Cronbach's α = 0.75 and 0.92).Reference Liddell, Nickerson, Felmingham, Malhi, Cheung and Den4
Discussion
Interpretation of findings
Considering the sizeable and increasing population of refugees and asylum-seekers, studies reporting the prevalence of CPTSD, and previously EPCACE and DESNOS, are surprisingly scarce. Nevertheless, important conclusions can still be drawn from the studies identified in this review. Consistent with previous systematic reviews of studies examining the prevalence of CPTSD, EPCACE and DESNOS in refugees and asylum seekers,Reference ter Heide, Mooren and Kleber18, Reference Mellor, Werner, Moussa, Mohsin, Jayasuriya and Tay19 the results demonstrate that treatment-seeking samples generally report higher prevalence estimates of CPTSD, EPCACE and DESNOS relative to population samples. Individuals who have more severe symptoms may be more likely to seek treatment. However, one study with a population sample of recently liberated Yazidi womenReference Grossman, Hoffman, Shrira, Kedar, Ben-Ezra and Dinnayi27 was an outlier, with the second highest prevalence estimate reported of all the included studies. Although determining the reason for this was not within the scope of this review, it may have been due to the high severity of the traumas experienced by this sample. The Yazidi women in this sample experienced repeated torture, sexual assault and sexual slavery during prolonged captivity; these experiences are closely associated with the specified risk factors of complex trauma. The homogeneity of this sample and the severity of trauma may contribute to a higher CPTSD prevalence.
Wide variations exist in the prevalence of CPTSD, EPCACE and DESNOS in the included studies. Potential contributing factors may include the geographic location of study implementation and culturally heterogenous study samples,Reference Teodorescu, Heir, Hauff, Wentzel-Larsen and Lien3, Reference Liddell, Nickerson, Felmingham, Malhi, Cheung and Den4, Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24, Reference Frost, Hyland, McCarthy, Halpin, Shevlin and Murphy26, Reference Hecker, Huber, Maier and Maercker28, Reference Mundy, Foss, Poulsen, Hjorthoj and Carlsson30, Reference Nickerson, Cloitre, Bryant, Schnyder, Morina and Schick31, Reference Rathke, Poulsen, Carlsson and Palic33, Reference Vang, Nielsen, Auning-Hansen and Elklit36 as hypothesised by Mellor et al.Reference Mellor, Werner, Moussa, Mohsin, Jayasuriya and Tay19 Cultural heterogeneity within samples may be associated with differences in traumatic exposure, with greater experiences of CPTSD risk factors leading to a higher prevalence of CPTSD. However, heterogeneity in the reporting of sample demographics, risk factors and trauma exposure meant that a closer examination of this was beyond the scope of the current review.
The higher prevalence of CPTSD compared with PTSD in six of 13 studies reporting PTSD data highlights that the diagnostic criteria for PTSD may not capture the complex psychological responses that follow complex trauma. However, the data suggest that only a minority of refugees develop CPTSD.
Although self-report measures may overestimate prevalence,Reference Richardson, Frueh and Acierno38 they were not consistently associated with higher prevalence estimates compared with observer- or clinician-rated measures. However, only three studies used observer-rated measures.
Differences in demographic characteristics may underpin the diversity in CPTSD prevalence. For instance, the length of time refugees spent in the host country, which is a predictor of the severity of CPTSD symptoms,Reference Barbieri, Visco-Comandini, Fegatelli, Schepisi, Russo and Calo24 varied greatly across studies. However, owing to inconsistencies in or the absence of reported post-migration stressors, it is unclear how prevalence estimates in the studies were affected.
Strengths and limitations
This review is the first to examine the prevalence of CPTSD, EPCACE and DESNOS in refugees and asylum seekers. Independent screening of full-text studies by all three authors ensured consistency and the appropriateness of included studies. Risk of bias was assessed systematically.
The evidence presented is limited by the methodological constraints of the studies included. Although the studies reported data relevant to the review question, they were primarily aiming to examine the validity and structure of the ICD-11 CPTSD construct in refugee samples rather than to measure prevalence. The sampling frames were often inappropriate, with few studies using census data. Most samples were also non-randomly drawn. Based on calculations in this review, sample sizes were inadequate in all studies with treatment-seeking samples; this was further emphasised by the wide confidence interval for prevalence estimates. There is also a risk of non-response bias, as response rates and information regarding differences between respondents and non-respondents were infrequently reported.
Several studies developed their own measures from scales not designed to identify CPTSD. This may have resulted in measurement bias.
Although the terms CPTSD, EPCACE and DESNOS are often used interchangeably when discussing the sequelae of complex trauma, conceptual issues may exist in the use of all three diagnoses in this review. However, considering the scarcity of research on the prevalence of each of these three diagnoses among refugees and asylum seekers, including all three diagnoses can be considered useful in understanding the proportion of this population experiencing complex psychological responses to trauma.
Implications
This systematic review has implications for treatment planning, highlighting the need to consider treatment needs among refugees and asylum seekers. Given that complex psychological responses are present in this population, awareness of prevalence estimates would facilitate the planning and provision of appropriate treatments targeting symptoms and encourage research to find safe treatment approaches that do not further traumatise these individuals. The addition of CPTSD as a diagnosis and the awareness of its prevalence among treatment-seeking refugees and asylum seekers may facilitate recognition of this disorder and ensure that adequate treatment is provided. Policy planners should also aim to promote mental health in this population, for instance, by addressing post-migration needs that may further prevent recovery from complex traumas.
Future directions
This review highlights the gaps in the existing literature, demonstrating the clear need for methodologically robust epidemiological studies seeking to better understand the prevalence of CPTSD among refugees and asylum seekers. Studies should be representative of diverse refugee and asylum-seeking populations and include a range of cultures and trauma experiences. This would enable a more detailed explanation of factors underlying the variability of CPTSD prevalence estimates across the studies identified in this review, without any potential methodological issues influencing the results and conclusions drawn. Such studies would allow for more precise and generalisable estimates of the prevalence of this disabling disorder. This review could be used as a platform to encourage the planning of research to address this treatment gap.
This review highlighted several key methodological issues that should be considered in the design and implementation of future studies to ensure data reliability. There is a clear need for future studies examining treatment-seeking samples to satisfy sample size requirements. Furthermore, heterogeneity exists in the CPTSD measurement tools used in studies, both validated and unvalidated. Future studies should consider the validity of tools administered to facilitate a CPTSD diagnosis, and whether tools measure all CPTSD domains. This is particularly relevant when measuring CPTSD cross-culturally, where translated tools and instruments created specifically for a study, whether validated or not, may lack sufficient construct equivalence. Cultural nuances must be reflected in measurement tools to capture CPTSD within communities. The cultural salience of CPTSD cross-culturally should also be considered. It would be of interest for future studies to further examine risk and protective factors experienced prior to, during and following forced migration that can predict the development of CPTSD. This may also relate to diversity in sample demographics, where heterogeneity in factors such as the country of origin or resettlement potentially affect the type, severity and number of traumas experienced, which in turn may influence CPTSD prevalence.
Studies are also needed to measure the prevalence in this population of disorders with features overlapping with those of CPTSD. These include, for instance, borderline personality disorder, which shares the core feature of emotional dysregulation in a comparable way.Reference Jowett, Karatzias, Shevlin and Albert39 Although patterns of response differ between CPTSD and these disorders, knowledge of the prevalence estimates of similar disorders occurring in this population would aid differential diagnosis and facilitate the provision of appropriate interventions and treatments to improve the mental health of refugees and asylum seekers suffering from disabling disorders such as CPTSD.
Future research should also examine the types of trauma which may be associated with CPTSD and the influence of post-migration factors, in order to aid diagnosis and appropriate treatment of traumatised asylum seekers and refugees and thereby promote their sustained recovery.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2021.1013
Data availability
The data supporting the findings of this review are available upon request from the corresponding author, U.D.S.
Author contributions
U.D.S., N.G. and C.K. were involved in the design of this systematic review. U.D.S. executed the searches, screened and retrieved relevant studies for inclusion, carried out data extraction and synthesis, assessed risk of bias in all included studies, and wrote the first draft. N.G. and C.K. screened full texts of articles, assessed risk of bias in included studies, contributed to the planning of the writing of the manuscript, and revised the draft. All authors approved the final version of the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
C.K. is a member of the editorial board of BJPsych Open.
ICMJE forms are in the supplementary material, available online at http://dx.doi.org/10.1192/bjo.2021.1013.









 Open access
Open access
eLetters
No eLetters have been published for this article.