

No CrossRef data available.
Article contents
Change to hospitalist providers had a minimal influence on overall antibiotic use in a VA long-term care setting
Published online by Cambridge University Press: 29 September 2023
Abstract
Core share and HTML view are not available for this content. However, as you have access to this content, a full PDF is available via the ‘Save PDF’ action button.
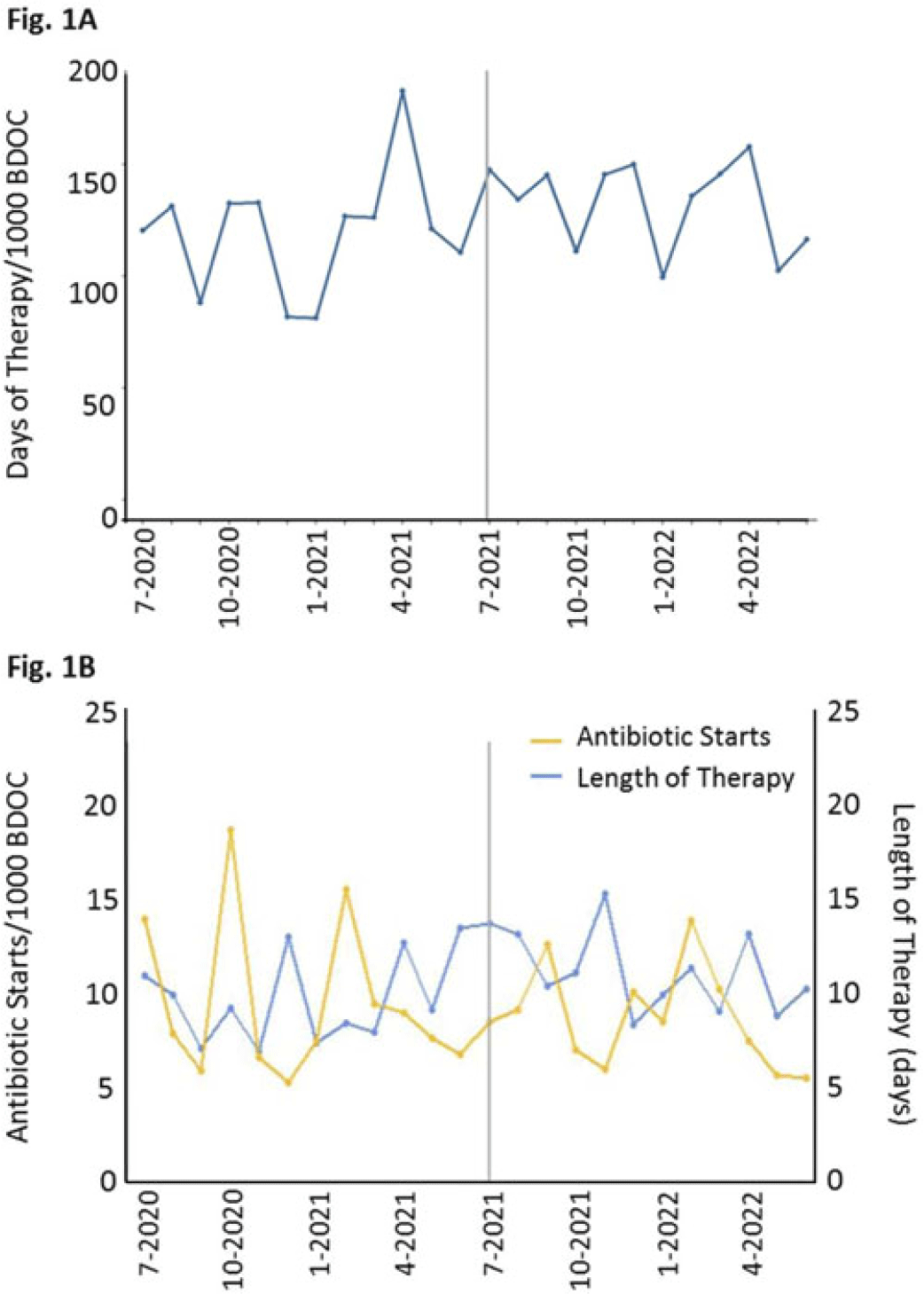
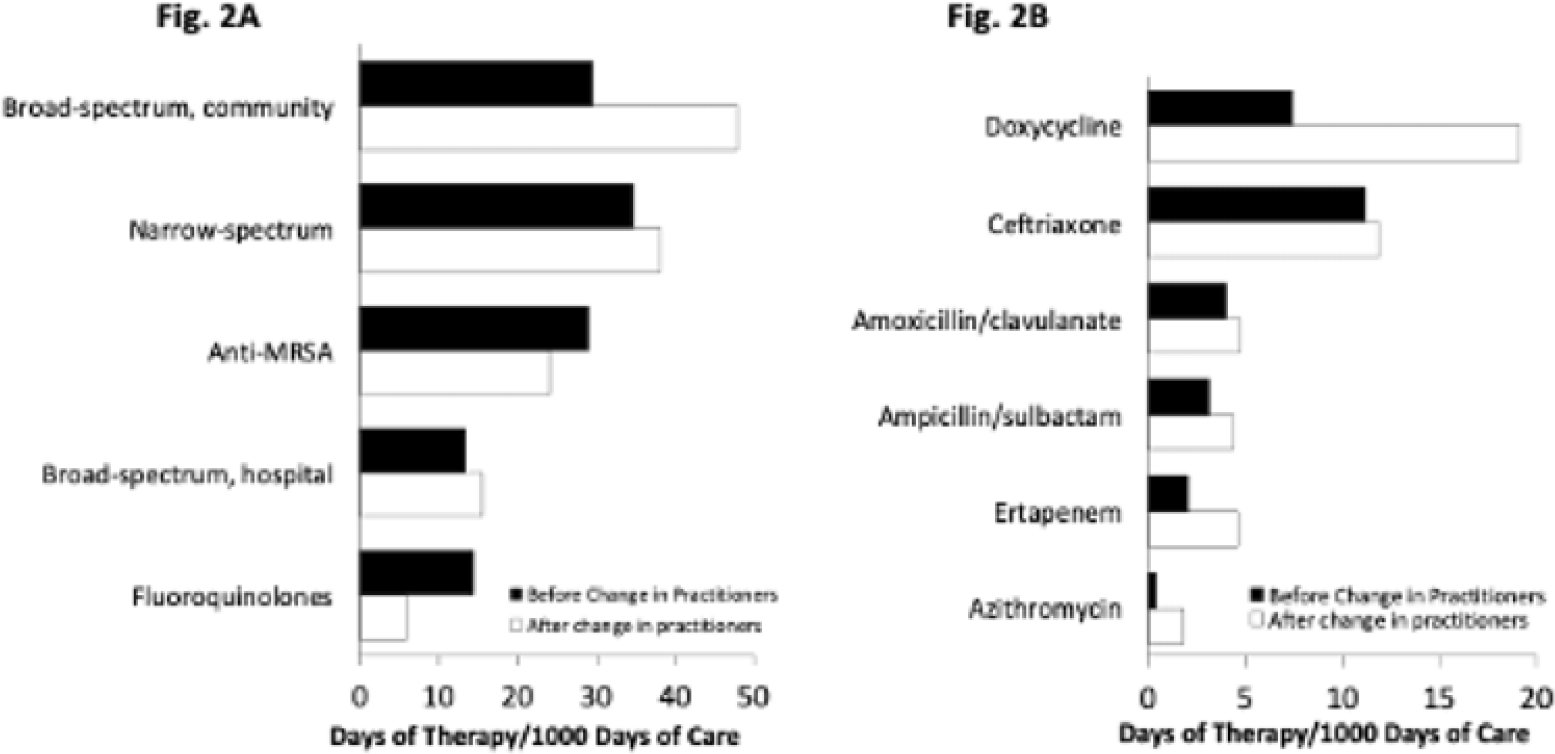
Background: In long-term care settings, practice patterns among practitioners are stronger determinants of antibiotic use than resident characteristics. In July 2021, hospitalists from the acute medicine service replaced geriatricians and assumed the care of residents in a 110-bed community living center (CLC) at a large academic Veterans Affairs (VA) medical center. We assessed changes in antibiotic use associated with that change of practitioners to guide stewardship efforts. We hypothesized that antibiotic use in the CLC would shift, reflecting the practice pattern of practitioners accustomed to treating patients in acute-care settings. Methods: We conducted a retrospective cohort study from July 1, 2020, through June 30, 2022, 1 year before and after the change of practitioners on July 1, 2021. We assessed resident characteristics and the following metrics of antibiotic use at monthly intervals: days of therapy (DOT) per 1,000 bed days of care (BDOC), antibiotic starts per 1,000 BDOC, and mean length of therapy (LOT) in days. We also compared the DOT per 1,000 BDOC for various antibiotics, in groups and individually. Results: In the years before and after the change of practitioners on July 1, 2021, the characteristics of CLC residents were comparable. Before and after July 1, 2021, monthly DOT per 1,000 BDOC (Fig. 1A), antibiotic starts per 1,000 BDOC, and mean LOT (Fig. 1B) were similar. After July 1, 2021, the use of fluoroquinolones decreased (14.31 vs 5.83 DOT per 1,000 BDOC; P < .01), and variations in anti-MRSA, narrow-spectrum, and broad-spectrum hospital agents were small, whereas the use of broad-spectrum community agents increased (29.42 vs 47.81 DOT per 1,000 BDOC; P < .01) (Fig. 2A). Within this group, there was increased use of doxycycline (7.42 vs 19.13 DOT per 1,000 BDOC; P < .01), ertapenem (2.03 vs 4.58 DOT per 1,000 BDOC; P < .01), and, modestly, azithromycin (0.40 vs 1.80 DOT per 1,000 BDOC) (Fig. 2B). Conclusions: The overall use of antibiotics, as measured by DOT, antibiotic starts, and LOT did not change after hospitalists assumed care of CLC residents. However, a notable decrease was observed in the use of fluoroquinolones, and an increase was observed in the use of doxycycline and ertapenem. Stewardship that is tailored to the type of provider and incorporates their practice patterns is needed to reinforce the prudent use of antibiotics.
Disclosures: None
- Type
- Long-term Care
- Information
- Antimicrobial Stewardship & Healthcare Epidemiology , Volume 3 , Issue S2: SHEA Spring 2023 Abstracts , June 2023 , pp. s79 - s80
- Creative Commons

 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.- Copyright
- © The Author(s), 2023. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
 You have
Access
You have
Access
 Open access
Open access