
8 results
Efficacy of noncarbapenem therapy for the treatment of ceftriaxone-resistant Enterobacterales outside the urinary tract
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 09 January 2024, e1
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Colonization with extended-spectrum cephalosporin-resistant Enterobacterales (ESCrE) in hospitalized patients in Botswana
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s81
-
- Article
-
- You have access
- Open access
- Export citation
-
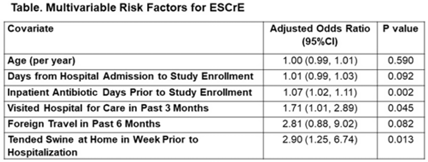
Background: The epidemiology of extended-spectrum cephalosporin-resistant Enterobacterales (ESCrE) in hospitalized patients in low- and middle-income countries (LMICs) is poorly described. Although risk factors for ESCrE clinical infection have been studied, little is known of the epidemiology of ESCrE colonization. Identifying risk factors for ESCrE colonization, which can predispose to infection, is therefore critical to inform antibiotic resistance reduction strategies. Methods: This study was conducted in 3 hospitals located in 3 districts in Botswana. In each hospital, we conducted ongoing surveillance in sequential units hospitalwide. All participants had rectal swabs collected which were inoculated onto chromogenic media followed by confirmatory testing using MALDI-TOF MS and VITEK-2. Data were collected via interview and review of the inpatient medical record on demographics, comorbidities, antibiotic use, healthcare exposures, invasive procedures, travel, animal contact, and food consumption. Participants with ESCrE colonization (cases) were compared to noncolonized participants (controls) using bivariable and multivariable analyses to identify risk factors for ESCrE colonization. Results: Enrollment occurred from January 15, 2020, to September 4, 2020, and 469 participants were enrolled. The median age was 42 years (IQR, 31–58) and 320 (68.2%) were female. The median time from hospital admission to date of sampling was 5 days (IQR, 3–12). There were 179 cases and 290 controls (ie, 38.2% of participants were ESCrE colonized). Independent risk factors for ESCrE colonization were a greater number of days on antibiotic, recent healthcare exposure, and tending swine prior to hospitalization. (Table). Conclusions: ESCrE colonization among hospitalized patients was common and was associated with several exposures. Our results suggest prior healthcare exposure may be important in driving ESCrE. The strong link to recent antibiotic use highlights the potential role of antibiotic stewardship interventions for prevention. The association with tending swine suggests that animal husbandry practices may play a role in community exposures, resulting in colonization detected at the time of hospital admission. These findings will help to inform future studies assessing strategies to curb further emergence of hospital ESCrE in LMICs.
Disclosures: None

Characterization of resistance to newer antimicrobials among carbapenem-resistant Klebsiella pneumoniae in the post–acute-care setting
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 28 July 2022, pp. 1159-1162
- Print publication:
- July 2023
-
- Article
- Export citation
Susceptibility reporting and antibiotic prescribing for UTIs in the inpatient setting: A nudge toward improved stewardship
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s17
-
- Article
-
- You have access
- Open access
- Export citation
-
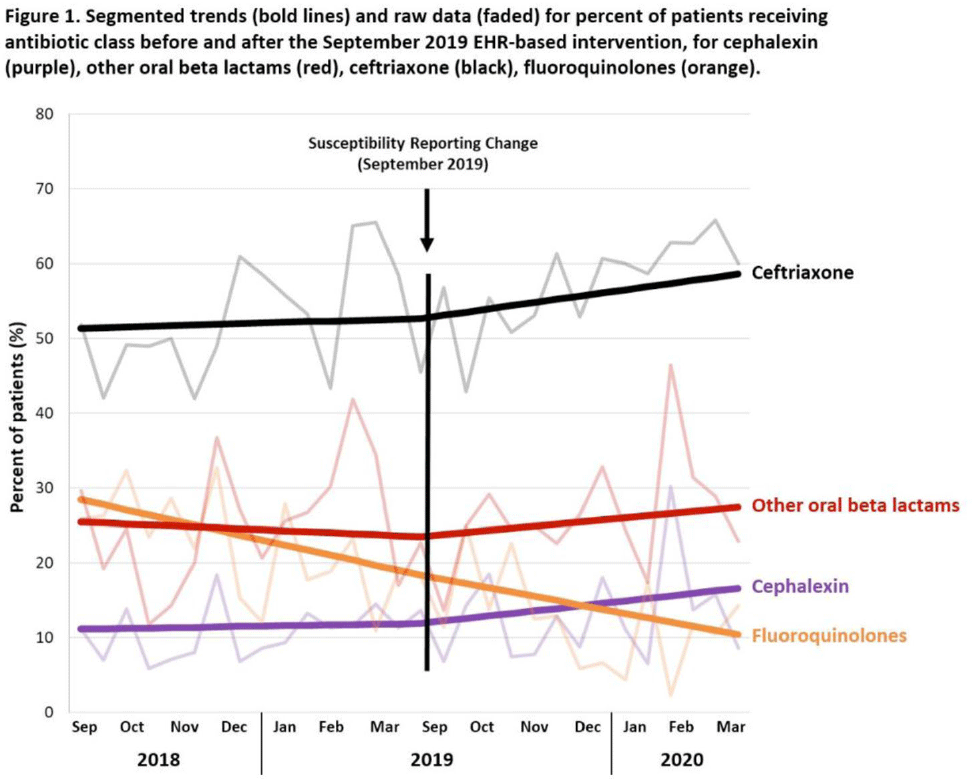
Background: Urinary tract infections (UTIs) are common in the inpatient, observation, and emergency department settings. Although many UTI-causing pathogens are susceptible to oral β-lactams, these agents are not tested directly, and susceptibility is extrapolated from other agents. To improve the use of these agents, the University of North Carolina Medical Center (UNCMC) added cephalexin to the susceptibility profile generated with urine culture results in the electronic health record (EHR). We evaluated prescribing trends of cephalexin, other oral β-lactams, fluoroquinolones, and other antibiotics for UTIs in the inpatient setting, before and after the susceptibility reporting change. Methods: An interrupted time-series analysis was conducted. Among 1,491 patients who had positive urine cultures with susceptibilities and received at least 1 antibiotic with a listed UTI indication during their inpatient stay at UNCMC, we measured the weekly prevalence (%) of patients who received each antibiotic group: cephalexin, other oral β-lactams (amoxicillin-clavulanate, cefdinir, cefuroxime), fluoroquinolones (levofloxacin, ciprofloxacin), and ceftriaxone. The study comprised a preintervention period (September 2018–March 2019) and a postintervention period (September 2019–March 2020). The prevalence of each antibiotic or group was plotted over time, and segmented linear regression was used to estimate the impact of the intervention on each antibiotic groups’ time trend. Results: At study baseline in September 2018, the weekly prevalence of antibiotic use was 11% for cephalexin, 26% for other oral β-lactams, 51% for ceftriaxone, and 29% for fluoroquinolones. Fluoroquinolone use decreased steadily throughout the study period, by 11% during the 7-month preintervention period (95% CI, −17% to −5%) and by 8% (95% CI, −13% to −3%) after the intervention (P for trend deflection, .70). In contrast, during the preintervention period, trends were flat for cephalexin, ceftriaxone, and other oral β-lactams (all P for nonzero preintervention slope were >.40). During the postintervention period, use increased for ceftriaxone (6%; 95% CI, 3%–9%). Post-intervention use also increased for cephalexin (5%; 95% CI, −3% to 12%) and other oral β-lactams (4%; 95% CI, −8%, 15%), but these trends were imprecise and not statistically significant at α = .05. Fig. 1 displays trends and raw data for each antibiotic group. Conclusions: The urine culture susceptibility reporting change was associated with small increases in cephalexin and ceftriaxone use, coincident with continued decreasing use of fluoroquinolones, for hospitalized patients with positive urine cultures and a listed UTI indication. Low-resource EHR-based interventions may confer considerable benefit for antimicrobial stewardship efforts in this clinical setting, and larger real-world studies are needed to replicate and contextualize these findings.
Funding: None
Disclosures: None

The Great Masquerade: Identification of Clinically Relevant Clostridioides difficile Infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s405
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Clinical Characteristics and Outcomes of Hematologic Malignancy Patients With Positive Clostridium difficile Toxin Immunoassay Versus Polymerase Chain Reaction Test Results
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 39 / Issue 7 / July 2018
- Published online by Cambridge University Press:
- 25 April 2018, pp. 863-866
- Print publication:
- July 2018
-
- Article
- Export citation
Impact of Organism Identification Method on Central Line-Associated Bloodstream Infection Designation
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 38 / Issue 8 / August 2017
- Published online by Cambridge University Press:
- 21 June 2017, pp. 1007-1009
- Print publication:
- August 2017
-
- Article
- Export citation
The Epidemiology of Carbapenem-Resistant Klebsiella pneumoniae Colonization and Infection among Long-Term Acute Care Hospital Residents
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 37 / Issue 1 / January 2016
- Published online by Cambridge University Press:
- 12 October 2015, pp. 55-60
- Print publication:
- January 2016
-
- Article
- Export citation
