



Introduction
The national burden of Clostridioides difficile infection (CDI) is approximately 460,000 cases per year in the United States with approximately half of cases attributed to healthcare-associated infection. Reference Guh, Mu and Winston1 Worldwide, CDI is the leading cause of infectious gastroenteritis in hospitalized patients. Reference Olsen, Stwalley, Demont and Dubberke2–Reference Feuerstadt, Theriault and Tillotson4 In addition to significant morbidity and mortality, the high disease incidence increases healthcare costs especially in hospitalized patients with cost estimates ranging from 1 billion to several billion dollars annually. Reference Ghantoji, Sail, Lairson, DuPont and Garey5 Healthcare costs, especially hospital readmissions, are increased by a high CDI recurrence rate that occurs in 15%–25% of patients given vancomycin, the most commonly used guideline-recommended antibiotic. Reference Dubberke, Gerding and Kelly6 However, no national healthcare policies are in use to reduce CDI-associated readmissions. A 30-day readmission rate has been used since the 1980s to inform hospital reimbursement models using the US Medicare inpatient prospective payment system. Reference Guterman and Dobson7 In this model, hospitals received a predefined payment rate based on diagnosis-related groups which persists to this day. Thirty-day readmissions have also been shown to increase mortality rates measured at 2 years postdischarge. Reference Shaw, Stiliannoudakis, Qaiser, Layman, Sima and Ali8 The Centers for Medicare and Medicaid Services also apply financial penalties to reduce hospital readmissions for select conditions to incentivize hospitals to use strategies that minimize the risk of hospital readmissions due to the disease state. Reference Rinne, Castaneda, Lindenauer, Cleary, Paz and Gomez9 These same incentives could be applied to CDI-associated readmissions. Infection control and pharmacologic strategies exist to minimize the risk of recurrent CDI; however, no policy incentives encourage using anti-CDI recurrence strategies. CDI in hospitalized patients is associated with a higher risk of hospital readmission, but a systematic review of the literature has not been performed. The purpose of this systematic review is to summarize 30-day CDI-associated readmission rates and discuss potential interventions utilized.
Methods
Literature search strategy and study selection
A literature search was conducted in PubMed, ScienceDirect, and EMBASE from their inception date through May 2023. Search terms utilized were “Clostridium difficile” or “Clostridioides difficile” and “hospital readmissions.” A filter for the English language was applied. Included studies reported CDI-associated 30-day readmission or rehospitalization. Articles categorized as case reports, case series, letters, editorials, meta-analyses, commentaries, review articles, and conference abstracts were excluded. The title and abstract were screened for eligibility and data extraction was done by 2 researchers by methods previously reported according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidance. Reference Page, McKenzie and Bossuyt10 Identified manuscripts were further subdivided as observational or interventional to assess prevention efforts for CDI-related readmissions.
Patient consent statement
This study does not include factors necessitating patient consent.
Data analysis
Studies on data of patients with CDI-associated 30-day readmission rates were evaluated. The perspective of 30-day readmissions was categorized as readmission evaluation to the same hospital only, the hospital health system only, or any readmission. Summary estimates of 30-day readmission rates were extracted and verified by a second reviewer. Study quality was assessed using the Newcastle-Ottawa Assessment Scale (NOS). Reference Lo, Mertz and Loeb11 The meta-analysis was done using the metaprop program in R version 4.3.1 and RStudio 2023.09.0. 12 Summary estimates were calculated using a random effects model.
Results
Two thousand five hundred and twenty-one articles were identified from the 3 search engines with 448 excluded due to duplication. After screening full-text articles, 9 eligible articles met the inclusion criteria. Reference Brumley, Malani, Kabara, Pisani and Collins13–Reference Verheyen, Dalapathi and Arora21 Seven articles reported data from the United States, 1 was Canadian, and the remaining was an international study that recruited patients from 30 countries. Most studies were observational (n = 6) or quasi-experimental (n = 2). Studies were either single site (n = 4) or multicenter (n = 5). The publication date range was 2002–2023. In total, 132,862 CDI patients were evaluated. The PRISMA flowchart is shown in Figure 1. Study quality NOS scores ranged from 5 to 8 (median: 6). Most (n = 7) studied both community- or healthcare-onset CDI with either primary or recurrent CDI being evaluated for all studies. Patients with CDI were either identified by ICD9/10 codes (n = 4) or a CDI diagnostic test with signs and symptoms (n = 5). In meta-analysis, high heterogeneity was observed in interventional (I2 = 84%) and observational (I2 = 94%) studies (P < .01, each).

Figure 1. Flow diagram of study selection.
CDI-associated readmission
Thirty-day CDI-associated readmissions were defined as either an ICD9/10 code indicating a CDI admission with a prior admission and CDI diagnosis within the past 30 days (n = 4) or a medical chart evaluation of signs and symptoms consistent with CDI (diarrhea) along with a positive diagnostic test (n = 5) with a prior hospitalization for CDI within the past 30 days. All studies were done in adults with 1 study studying only adults greater than or equal to 65 years. Thirty-day CDI-associated readmission rates ranged from 5.4% to 12.7% (Table 1). Meta-analysis of observational studies (Figure 2) estimated 30-day CDI-associated readmissions were 6% (95% CI, 5%–7%).
Table 1. Characteristics of included studies
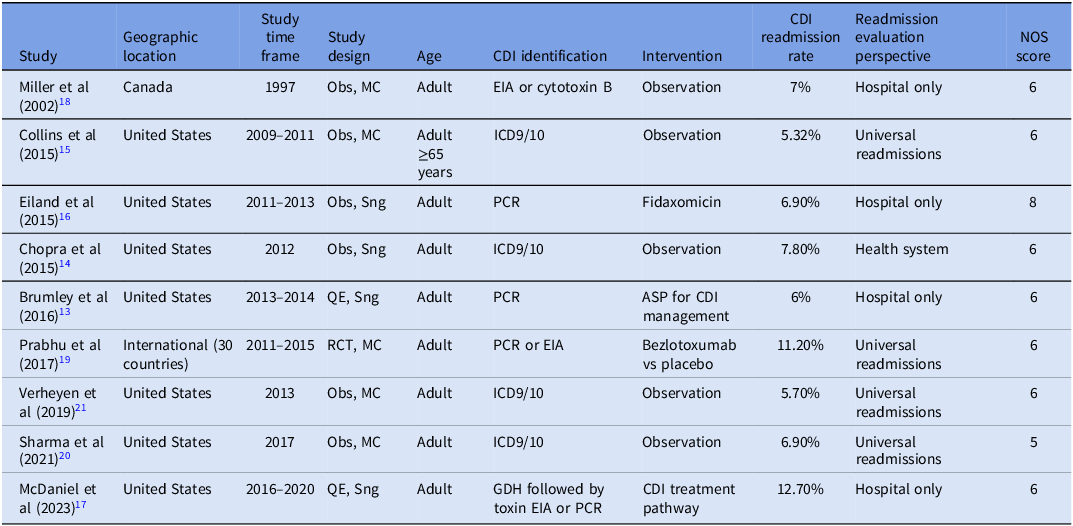
Obs, observational study; MC, multicenter study; Sng, single-site study; RCT, randomized controlled trial; PCR, polymerase chain reaction; GDH, glutamate dehydrogenase; EIA, enzyme immunoassay; ASP, antimicrobial stewardship program; NOS, Newcastle-Ottawa Assessment Scale.

Figure 2. Forest plot for 30-day CDI-associated hospital readmission. Note: CDI, Clostridioides difficile infection.
Prevention of CDI-associated readmission
Three studies evaluated the effect of active interventions to reduce CDI-associated 30-day readmission rates (Figure 2). Studies were either quasi-experimental (n = 2) or as part of a randomized controlled trial comparing bezlotoxumab to placebo (n = 1). Baseline or placebo rates ranged from 6% to 13%, and 2 of 3 interventions reduced the likelihood of CDI-associated 30-day readmissions (range: 2%–5%)
Conclusion
CDI affects patient mortality and morbidity and increases hospitalization costs. Reference Ghantoji, Sail, Lairson, DuPont and Garey5,Reference Hengel, Schroeder and Jo22 The 2017 estimates for CDI were approximately 462,000 cases of which 235,000 were healthcare-associated making rehospitalizations a significant CDI healthcare cost. Reference Guh, Mu and Winston1 Despite studies investigating CDI-associated readmission rates, a systematic review and meta-analysis have not been performed to calculate estimated rates or investigate prevention strategies. Our study identified an overall rate of 30-day CDI-associated readmission of 7% (95% CI, 5%–8%). These results were consistent between differing study designs, locations, years, and other study characteristics. This study was unable to distinguish between polymerase chain reaction (PCR)-based and other testing for C. difficile infection. PCR testing does not differentiate colonization from infection, and thus, it is quite possible that a portion of CDI readmission cases may have been colonized with C. difficile and admitted for other reasons. A critical review of hospitalization and CDI costs estimated attributable costs for CDI that ranged from $6,774 to $12,212 (2014 USD) for CDI requiring hospital admission. Reference Gabriel and Beriot-Mathiot23 Readmission rates have been shown to affect hospital financial performance in other disease states. Reference Upadhyay, Stephenson and Smith24 In addition to cost containment, readmissions are often considered an easily available measure of quality of care. Reference Fischer, Lingsma, Marang-van de Mheen, Kringos, Klazinga and Steyerberg25 However, distinguishing between planned and unplanned readmissions can be difficult, and accurate data coding can be problematic. This is especially important for CDI in which antibiotics given after hospital discharge can also precipitate dysbiosis of the gut microbiome increasing the risk of CDI. A comprehensive case for economic cost benefits to develop strategies to prevent recurrences was not identified in our review. Nonetheless, in this systematic review, both antimicrobial stewardship strategies in general and the use of therapies known to reduce the likelihood of CDI recurrence (bezlotoxumab) were effective at reducing hospital readmissions. Reference Brumley, Malani, Kabara, Pisani and Collins13,Reference Prabhu, Cornely and Golan19 The interventional studies had above-average readmission rates at baseline. Whether interventions in hospitals with an average rate of 6% would be as effective will require further study. Study quality for identified manuscripts was adequate although we did not personally contact authors for NOS scores but rather judged based on information provided. The 2 nationwide studies were conducted during overlapping periods leaving a small possibility of duplication of patients. Patients in these studies were identified by ICD9/10 codes which may not be entirely reliable. The antimicrobial stewardship bundle included appropriate CDI antimicrobial therapy based on local guidelines, discontinuation of acid suppressive therapy if not indicated, and discontinuation of other unneeded antimicrobials. Reference Brumley, Malani, Kabara, Pisani and Collins13 These data demonstrate that 30-day CDI-associated readmissions are common and modifiable. With a high incidence of disease and the costs of hospitalization, hospital budget holders should invest in strategies that can prevent CDI or recurrent CDI and scale it to invest globally to reduce rates. This would help allocate hospital beds for patients in most need and help allocate resources to CDI patients identified with a high risk of hospital readmission.
In conclusion, this systematic review identified a 6% rate of 30-day CDI-associated hospital readmission. Interventions including antimicrobial stewardship efforts and the use of bezlotoxumab were shown to reduce these rates.
Author contributions
Conceptualization: K. W. G., T. A. E., K. J., and J. J.
Methodology: K. W. G., T. A. E., K. J., and J. J.
Investigation: K. W. G., T. A. E., K. J., and J. J.
Visualization: K. W. G., T. A. E., K. J., and J. J.
Funding acquisition: K. W. G.
Project administration: K. W. G.
Supervision: K. W. G.
Writing—original draft: T. A. E., K. J., and J. J.
Writing—review and editing: K. W. G., T. A. E., K. J., and J. J.
Financial support
This work was supported, in part, by the National Institute of Allergy and Infectious Diseases (NIAID), T32 AI141349 and R01AI139261.
Competing interests
K. W. G. received research grant support from Acurx Pharmaceuticals and Paratek Pharmaceuticals. All other authors report no conflicts of interest relevant to this article.



