



Protein-energy wasting (PEW) is a frequent complication in chronic kidney disease (CKD) patients, especially in those with end-stage renal disease. Previous studies have reported a prevalence of PEW ranging from 17 % to 85 %(Reference Carrero, Thomas and Nagy1). PEW attenuates treatment response and increases poor prognosis in patients with CKD(Reference Kalantar-Zadeh, Ikizler and Block2,Reference Obi, Qader and Kovesdy3) . Nutritional assessment scale to detect and manage PEW is suggested(Reference Obi, Qader and Kovesdy3,Reference Ikizler, Burrowes and Byham-Gray4) . Subjective global assessment (SGA) is a simple, inexpensive and widely used nutritional scale that can be used by trained medical professionals. The utility of SGA in CKD has been recognised by researchers(Reference Cuppari, Meireles and Ramos5–Reference Vero, Byham-Gray and Parrott8).
Insufficient food intake caused by loss of appetite and dietary restriction is the direct adverse factor for PEW in CKD patients(Reference Carrero, Stenvinkel and Cuppari9). In a cross-sectional study, 56·6 % of CKD patients did not reach the recommended energy intake(Reference Huang, Chen and Hung10). Inadequate energy intake was correlated with renal progression and nutritional status(Reference Huang, Chen and Hung10–Reference Burrowes, Cockram and Dwyer12). The dietary energy intake (DEI) for CKD 1–5 patients, as recommended by KDOQI, is 25–35 kcal/kg/d(Reference Ikizler, Burrowes and Byham-Gray4). The International Society for Renal Nutrition and Metabolism recommends a daily energy intake of 30–35 kcal/kg/d for non-dialysis CKD patients(Reference Ikizler, Cano and Franch13). Kopple JD et al. observed the maintenance of negative nitrogen balance with energy intake below 30 kcal/kg/d in non-dialysis patients who consumed protein 0·55–0·60 g/kg/d(Reference Kopple, Monteon and Shaib14). No studies have investigated the minimum energy intake to prevent PEW in non-dialysis CKD.
A low-protein diet combined with keto acids can delay the progression of kidney disease and is therefore considered one of the strategies for the treatment of CKD(Reference Ikizler, Burrowes and Byham-Gray4,Reference Rhee, Ahmadi and Kovesdy15) . However, previous studies have different opinions on the effects of a low-protein diet on nutritional indicators, and whether a low-protein diet increases the risk of PEW in patients is inconsistent in current studies(Reference Burrowes, Cockram and Dwyer12,Reference Hahn, Hodson and Fouque16–Reference Lee, Kim and Kim19) . In addition, no studies have considered energy intake when investigating the relationship between dietary protein intake (DPI) and PEW. Moreover, nutritional status in those studies were from biochemical or body-composition analysers, which were insufficiently comprehensive.
In this study, we aimed to identify the association between DEI, DPI and PEW as assessed by SGA and to evaluate dose–response relationship between DEI and PEW in CKD. In addition, we further investigated the relationship between DPI and PEW in different DEI subgroups.
Methods
Participants
This was a cross-sectional study conducted in nephrology department of Sun Yat-Sen Memorial Hospital, and CKD stages 1–5 inpatients ≥ 14 years from September 2019 to July 2022 were enrolled. Those undergoing dialysis and renal transplantation were excluded. Besides, patients with acute or severe illnesses (e.g. acute gastroenteritis, acute heart failure, active infection or respiratory failure), patients with conditions that increase catabolism (e.g. cancer or thyroid dysfunction) and patients who were unable to complete the 3-d dietary survey were also excluded. The study was approved by the Ethics Committee of Sun Yat-sen Memorial Hospital and the approval number was SYSKY-2022–491–01.
Measurement and data collection
The data collected included gender, age, comorbidities, laboratory indicators, anthropometric indicators, SGA score and dietary indicators. Comorbidities included a history of hypertension and diabetes mellitus. Fasting blood samples were collected from patients on the second day of admission and were tested using automated instruments. Anthropometric measurements, SGA score and dietary intake assessment were conducted during hospitalisation by a trained dietitian in the department of clinical nutrition.
Laboratory indicators
Routine laboratory data were obtained, including Hb, total lymphocyte count (TLC), serum creatinine (Scr), urine acid, serum bicarbonate, glucose (Glu), total cholesterol, TAG, HDL-cholesterol, LDL-cholesterol, albumin (Alb), serum ferritin. We calculated estimated glomerular filtration rate (eGFR) using the CKD Epidemiology Collaboration equation and CKD stages were defined according to the KDIGO 2012 clinical practice guideline for evaluation and management of CKD(Reference Inker, Astor and Fox20).
Subjective global assessment score
SGA scale consists of five historical components and three physical examinations. Historical components included weight change in the last 6 months and the last 2 weeks, changes in dietary intake, symptoms of gastrointestinal, functional capacity and comorbidities affecting nutritional requirements. Physical examinations contained subcutaneous fat (orbital fat pads, triceps, biceps and chest), muscle wasting (temporal, clavicle, shoulder, interosseus, scapula, interosseus, quadriceps and gastrocnemius) and edema/ascites. According to the subjective and objective nutritional status, SGA was scored and patients were divided into well nourished (A) group, moderate malnutrition (B) group and severe malnutrition (C) group. Patients with scores B and C were defined as PEW(Reference Detsky, McLaughlin and Baker21).
Anthropometric indicators
BMI was calculated by dividing weight (kilograms, kg) by the square of the height (meters, m). Waist:hip ratio refers to waist circumference in centimeter (cm) divided by hip in cm and circumferences measured by the authors of the study.
Dietary intake assessment
Three-day dietary recalls were performed to obtain DEI and DPI for patients. The dietitian asked patients in detail about their diet for the 3 days before enrollment, including the type and amount of food, oil and salt in each meal and snacks. Daily total dietary energy and protein was calculated according to Chinese Food Composition Table (6th edition). DEI and DPI were equal to the daily energy and protein intake divided by ideal body weight. Ideal body weight for male (kg) = (height (cm)–100) × 0·9; ideal body weight for female (kg) = ideal body weight (male) – 2·5. Patients with DEI < 30 kcal/kg/d and ≥ 30 kcal/kg/d were considered as inadequate DEI group and adequate DEI group, respectively.
Statistical analysis
Data were presented as mean ± sd for normally distributed variables median (interquartile range) for non-normally distributed variables and n(%) for categorical variables. Continuous variables were compared between the two groups with the use of student’s t test or one-way ANOVA. The comparison of proportion of male, hypertension, diabetes mellitus and PEW between DEI adequate and inadequate groups was tested with χ2. A multivariate logistic regression model was performed to identify independent relationships between DEI, DPI and PEW. Models between DPI and PEW in different DEI groups were also analysed to explore whether the relationship between DPI and PEW was affected by energy intake. Adjusted factors in multivariate model were indicators with P less than 0·05 in univariate analysis, including eGFR, Hb, Lym, Alb and serum ferritin. Restricted cubic spline analysis with four knots was performed using R language (version 6.2.0) to explore dose–response relationship between DEI and PEW. Differences were considered statistically significant if a P value < 0·05. All statistical analysis, unless restricted cubic spline analysis, was performed using SPSS (version 25.0). In addition, to identify the reliability of our results, we set alpha to 0·5 and calculated the power of this study by PASS (version 11) based on the sample size and the proportion of PEW in both groups.
Results
Study patients and comparison of groups
The median age of 409 participants was 46·0 (33·0, 57·0) years, with 50·1 % male, 53·8 % had hypertension and 18·6 % had diabetes mellitus. The median eGFR was 48·92 (15·09, 94·46) ml/min/1·73 m2. The stages 1–5 of CKD were 28·9 %, 16·9 %, 15·4 %, 14·9 % and 24·0 %, respectively. The aetiologies of CKD include primary glomerular disease (72·4 %), diabetic nephropathy (10·0 %), hereditary nephropathy (2·7 %), hypertensive nephropathy (2·2 %), lupus nephritis (2·0 %), gouty nephropathy (1·0 %) and others (9·7 %). DEI and DPI were 27·63 (sd 5·79) kcal/kg/d and 1·00 (0·90, 1·20) g/kg/d, respectively. Of the total sample, 69·2 % (n 283) were classified as belonging to the inadequate DEI group, while the remaining 30·8 % (n 126) were categorised as having sufficient DEI. The prevalence of malnutrition, as assessed by SGA, was found to be 18·6 %, comprising of 9·5 % in the adequate DEI group and 22·6 % in the inadequate DEI group. Additionally, the study demonstrated a high statistical power of 0·91, indicating that the sample size was sufficient.
As can been be seen in Table 1, patients with lower DEI had significantly lower TLC and higher prevalence of PEW. The levels of serum cholesterol and LDL were significantly increased in the adequate DEI group. Other indicators, including age, gender, rates of hypertension and diabetes mellitus, BMI, waist:hip ratio, MAMC, Hb, eGFR, urine acid, serum bicarbonate, Glu, TAG, Alb and serum ferritin, were not different between the two groups.
Table 1. Clinical characteristics of individuals and comparisons between subgroups (numbers and percentages; median values and interquartile ranges; mean values and standard deviations)
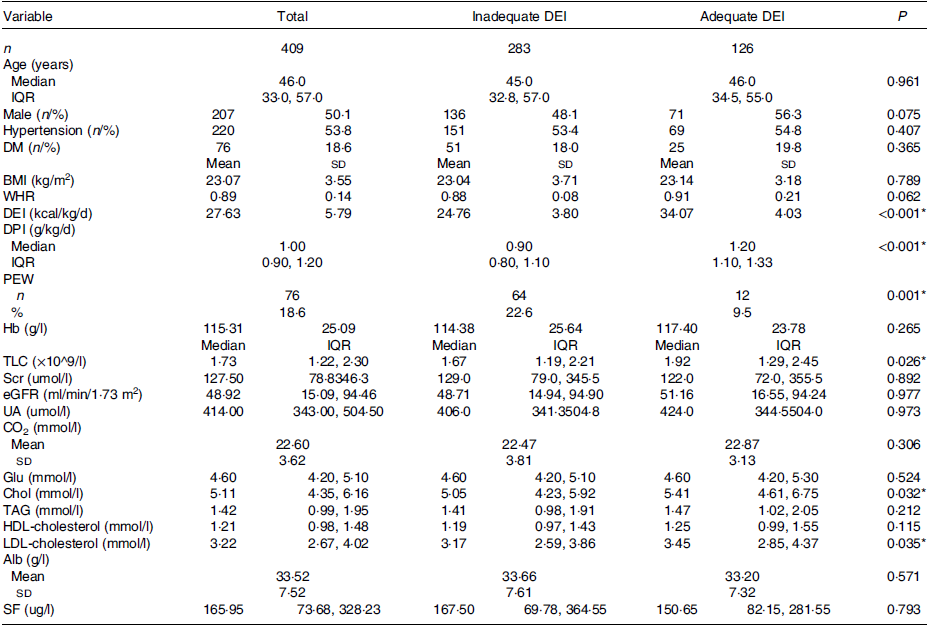
DEI, dietary energy intake; IQR, interquartile range; DM, diabetes mellitus; WHR, waist:hip ratio; DPI, dietary protein intake; PEW, protein-energy wasting; TLC, total lymphocyte count; Scr, serum creatinine; eGFR, estimated protein-energy wasting glomerular filtration rate; UA, urine acid; Glu, glucose; Chol, total cholesterol; Alb, albumin; SF, serum ferritin.
* P < 0·05 was considered statistically significant.
Relationship between dietary energy intake, dietary protein intake and protein-energy wasting
After adjustment for eGFR, Hb, TLC, Alb and serum ferritin, multivariate logistic regression model showed that DEI was an independent factor of PEW (Table 2). For every 1 kcal/kg/d increase in DEI, the incidence of PEW decreased by 12·0 % (OR = 0·880, 95 % CI = 0·830, 0·933, P < 0·001). As for DPI, it was also significantly related to PEW, and the incidence of PEW reduced by 9·69 % for every 0·1 g/kg/d increase in DPI (OR = 0·031, 95 % CI = 0·008, 0·119, P < 0·001). However, the effect of DPI on PEW disappeared in the subgroup with adequate DEI (P > 0·05) and remained in the inadequate DEI subgroup (OR = 0·006, 95 % CI = 0·001, 0·043, P < 0·001).
Table 2. Multivariable logistic regression analysis of DEI, DPI to PEW (odds ratios and 95 % confidence intervals)

DEI, dietary energy intake; DPI, dietary protein intake; PEW, protein-energy wasting; Hb, hemoglobin; TLC, total lymphocyte count; Alb, albumin; SF, serum ferritin.
Model 1: Unadjusted.
Model 2: Adjusted by model 1 + age + gender + Scr.
Model 3: Adjusted by model 2 + Hb + TLC + Alb + SF.
* P < 0·05 was considered statistically significant.
Dose–response relationship between dietary energy intake and protein-energy wasting
Unadjusted restricted cubic spline analysis showed a nonlinear decreasing relationship between DEI and the risk of PEW (overall P < 0·001; Fig. 1(a)). Multivariable restricted cubic spline model showed that the curve between DEI and risk of malnutrition was similar to the curve in unadjusted model (overall P < 0·001, Fig. 1(b)). DEI > 27·6 kcal/kg/d significantly lowered the risk of PEW.

Fig. 1. Dose–response analysis showed a nonlinear decreasing curve relationship between DEI and PEW, DEI ≥ 27·6 kcal/kg/d may reduce the risk of PEW in CKD: (a) unadjusted analysis (overall P < 0·001); (b) multivariate adjusted for age, gender, Scr, Hb, total lymphocyte count, albumin and serum ferritin (overall P < 0·001). CKD, chronic kidney disease; DEI, dietary energy intake; PEW, protein-energy wasting.
Discussion
In this cross-sectional study, the prevalence of malnutrition was 18·6 % and patients with DEI < 30 kcal/kg/d accounted for 69·2 %. Low DEI was a significant predictor of PEW, and DEI > 27·6 kcal/kg/d may prevent PEW in non-dialysis CKD patients. Low DPI was also significantly related to PEW, but the effect missed in patients with DEI ≥ 30 kcal/kg/d.
Mechanisms in decreased energy and protein intake are integrated, including anorexia, dietary restrictions, alterations in organs involved in nutrient intake, depression and inability to obtain or prepare food(Reference Carrero, Stenvinkel and Cuppari9). It is common for patients with CKD to have actual DEI lower than dietitian recommendations. Huang et al. defined recommended energy according to KDOQI guideline(Reference Beto and Bansal22) and founded that 56·6 % of CKD patients had energy intakes less than 90 % of recommended levels(Reference Huang, Chen and Hung10). In another study involving 100 patients with CKD, only three patients met the recommended daily energy intake(Reference Gebretsadik, Mengistu and Molla23). A significant proportion of patients in this study also had inadequate energy intake, potentially attributed to the tendency among Chinese individuals to prioritise dietary control upon discovering a disease, while neglecting timely access to scientific diet guidance. More attention should be paid to the importance of scientific dietary guidance in clinical practice, with an emphasis on initiating such guidance as early as possible.
We observed that Lym counts were significantly decreased in the insufficient energy intake group. TLC is a traditional and frequently used nutritional indicator, which decreases in malnourished patients(Reference Omran and Morley24). It has been shown that CKD patients with nutritional risk had significantly lower TLC compared with CKD patients without nutritional risk(Reference Tan, Long and Fang25). The present study also found that TLC was significantly decreased in patients with PEW than in those without PEW (1·39 (0·97, 2·01) v. 1·80 (1·28, 2·37), P < 0·001). There was no significant difference in Alb between the DEI sufficient group and the DEI insufficient group in our study. Patients with low DPI may experience decreased albumin(Reference Noce, Vidiri and Marrone18,Reference Hsu, Yen and Wu26) . However, the results of the KNOW-CKD study found no difference in Alb between the two non-low-protein groups(Reference Lee, Kim and Kim19). Table 1 shows that although there was a clear difference in DPI between the two groups, DPI was greater than 0·8 g/kg/d in both groups. This may account for the lack of difference in albumin between the two groups in this study.
Serum lipids, including serum cholesterol and LDL, were significantly elevated in the adequate DEI group. Similarly, Yang et al. reported that patients with higher DEI had higher serum serum cholesterol levels in haemodialysis patients(Reference Yang, Qin and Li27). Dietary cholesterol intake was higher in the DEI sufficient group than in the DEI insufficient group (310·7(199·4450·6) mg/d v. 293·7(156·3, 436·8) mg/d, P = 0·047, not shown in Tables). Dietary cholesterol could lead to elevated serum cholesterol, which had been demonstrated in animal model(Reference Liang, Jiang and Cheng28). Human metabolic studies have also found a positive correlation between dietary cholesterol and serum cholesterol(Reference Grundy29,Reference Stellaard30) . However, other confounding factors that affect blood lipids, such as lipid-lowering drugs and exercise, were not considered in our study. Lipids metabolism is impaired due to inflammation and oxidative stress, and dyslipidaemia is prevalent in CKD(Reference Hager, Narla and Tannock31,Reference Bulbul, Dagel and Afsar32) . The relationship between DEI, dietary lipid intake and blood lipids in CKD patients deserves further investigation. It also reminds us to consider possible lipid effects when formulating the recommended energy intake for patients.
Patients with CKD often suffer from PEW. There are various scales used to identify malnutrition. The simple and widely used SGA scale was performed in this study. The prevalence of PEW in our study was slightly higher than the 11–18 % reported in previous studies using SGA scale(Reference Carrero, Thomas and Nagy1). Moreover, we observed patients in inadequate energy group were more likely to develop PEW. DEI is identified as a crucial determinant of nutritional status. However, the detailed relationship between DEI and PEW was not explored in CKD, the DEI threshold capable of predicting PEW is unknown. In this study, multivariate logistic regression analysis found that higher DEI intake was associated with greater protection against PEW. Moreover, we observed that the lowest DEI to prevent PEW was 27·6 kcal/kg/d. The identified cut-off value in our study was found to be below the recommended range of dietary energy intake as per previous guidelines(Reference Ikizler, Burrowes and Byham-Gray4,Reference Ikizler, Cano and Franch13) , prompting us to question whether our population necessitates adherence to the current energetic intake recommendations. We believe that more studies with larger sample size are needed in the future to establish nutritional guidelines suitable for Chinese CKD patients.
Nutrition guidelines for CKD suggest low DPI for preventing from renal progression(Reference Ikizler, Burrowes and Byham-Gray4). Studies are limited as to whether low-protein diets lead to malnutrition. Hahn et al. systematically reviewed the RCT studies of a low-protein diet in patients with CKD and found that only fifteen studies focused on the effect of DPI on PEW, of which twelve had no evidence of PEW, and three studies had a small number of patients with PEW in DPI and non-DPI groups. Therefore, there were insufficient data to compare the risk of PEW between low-protein and non-low-protein groups(Reference Hahn, Hodson and Fouque16). This may be due to the good baseline nutritional status and methods of evaluating PEW in the previous study. Lee et al. found that the risk of PEW significantly increased as DPI decreased, especially in those with DPI < 0·94 g/kg/d(Reference Lee, Kim and Kim19). We also demonstrated that low DPI was a predictor of malnutrition. Nevertheless, lower DPI did not increase the risk of PEW in group with adequate energy intake.
Our results suggest that adequate energy intake rather than protein intake is more vital for the prevention of PEW, which confirms the nutritional safety of a low-protein diet to a certain extent. Some limitations existed in this study. There may be recall bias in dietary assessment using the 3-day recall method. We used 30 kcal/kg/d as the energy intake standard for grouping, without considering age, BMI, diabetes, CKD stage and other factors. The study was cross-sectional, and the causal relationship between DEI, DPI and PEW cannot be explored.
Conclusion
In CKD patients, energy intake had a greater effect on PEW than protein intake, and dietary energy intake ≥ 27·6 kcal/kg/d may prevent malnutrition.
Acknowledgements
The authors thank the support from National Natural Science Foundation of China (82270743), National Key R&D Program of China (No. 2021YFC2009400) and Natural Science Foundation of Guangdong Province (2021A1515010801).
The authors declare no conflict of interest.
Participants enrollment and data collection, Q. H., R. Z., F. Q. and W. L.; data analysis and manuscript writing, Q. H., R. Z. and J. W.; anthropometric and dietary intake assessment, F. H. and C. C.; study design and guidance and manuscript revision, Q. Y. and C. C. All authors contributed significantly to the conduct of the study and approved the final manuscript.
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the ethics committee of Sun Yat-Sen Memorial hospital (Approval Number: SYSKY-2022-491-01), exempt from informed consent was agreed from the ethics committee.
The datasets generated or analysed during this study are available from the corresponding author upon reasonable request.



