


Widespread increases in overweight and obesity have raised the incidence of chronic disease, generating serious public health consequences for many countries. The rapid rise in obesity among young people is particularly alarming given that adolescent obesity tends to persist into adulthood(Reference Power, Lake and Cole1, Reference Kvaavik, Tell and Klepp2). Indeed, adolescence has been identified as a critical period for the establishment of lifelong health behaviours(Reference Must and Strauss3, Reference Berkey, Rockett and Field4) and is consequently a priority age group for initiatives that promote healthy lifestyles.
The physiological changes that characterise the adolescent years are often accompanied by a heightened awareness of peer approval and social norms. In adolescent girls, external pressures to be slim can raise the importance of body image and weight perceptions in the determination of self-concept, and can lead to the adoption of dieting and exercising for weight control(Reference McVey, Tweed and Blackmore5, Reference Field, Camargo and Taylor6). However, a number of studies suggest that discordance between perceptions of weight and actual weight status is common in young women(Reference Brener, Eaton and Lowry7–Reference Neumark-Sztainer, Croll and Story11). Misconceptions of body size are of concern given the potential for negative health outcomes: girls who incorrectly perceive themselves to be overweight may face an elevated risk of eating disorders such as anorexia nervosa(Reference Wakeling12). Conversely, overweight girls who are unable to recognise their condition are unlikely to initiate the lifestyle changes required to obtain a healthy body weight(Reference Strauss13). Although both situations are clearly undesirable, given the current prevalence of overweight and obesity the potential to underestimate a state of excessive body fat (BF) presents the greater public health risk.
Earlier efforts to quantify the prevalence and consequences of weight misclassification have been complicated by variation among ethnic groups. Desmond et al.(Reference Desmond, Price and Hallinan14) reported that while 100 % of overweight Caucasian girls correctly classified themselves, only 40 % of overweight African American girls recognised their weight status. Similarly, Neumark-Sztainer et al.(Reference Neumark-Sztainer, Croll and Story11) noted that African American adolescent girls were less likely than their Caucasian counterparts to perceive themselves as overweight despite a significantly higher prevalence of overweight. The tendency for adolescent girls of African American descent to misclassify their overweight status was further reinforced by Strauss(Reference Strauss13) and Brener et al.(Reference Brener, Eaton and Lowry7), the latter authors also observing high rates of misclassification among overweight Hispanic girls. In contrast, ethnic differences in the ability to recognise excess weight were not detected by Simeon et al.(Reference Simeon, Rattan and Panchoo9) in a study of South Asian, African and mixed ethnicity adolescent girls. It should be noted that the majority of literature in this area originates from the United States; issues surrounding weight perceptions in countries with different health-care systems and immigration patterns are poorly understood.
A potential shortcoming of earlier comparisons of weight perceptions and body size in adolescent girls from multiple ethnic groups was the use of universal BMI thresholds to define overweight. The existence of physiological differences in the body composition of girls from different ethnic groups has raised concerns over the appropriateness of existing BMI classification systems. For example, young people of East Asian(Reference Deurenberg, Deurenberg-Yap and Foo15, Reference Duncan, Duncan and Schofield16), South Asian(Reference Duncan, Duncan and Schofield16, Reference Mehta, Mahajan and Steinbeck17) and Hispanic(Reference Ellis18, Reference Ellis, Abrams and Wong19) descent tend to have more BF than Caucasians at an equivalent BMI. Conversely, Polynesian(Reference Duncan, Duncan and Schofield16, Reference Rush, Puniani and Valencia20) and African American(Reference Daniels, Khoury and Morrison21) children and adolescents average less BF than their Caucasian counterparts for the same BMI. It is therefore possible that the ethnic differences previously observed in the self-diagnosis of overweight may reflect differences in the accuracy of BMI standards for predicting BF status in diverse populations. Moreover, pubertal development and socio-economic status (SES) may also vary by ethnicity and contribute to the perceptions of overweight in adolescent girls.
Ethnic variation in weight loss practices has also been shown in female adolescents. For example, several studies have shown that African American girls are less likely to diet to lose weight than Caucasian girls(Reference Strauss13, Reference Desmond, Price and Hallinan14, Reference Field, Aneja and Austin22). In addition, Neumark-Sztainer et al.(Reference Neumark-Sztainer, Croll and Story11) reported that Asian American girls were more likely to diet than Caucasian girls. While only one study compared exercise as a weight control practice in different ethnic groups, similar variation was observed among ethnicities: African American girls were less likely to exercise for weight loss than Caucasian girls(Reference Desmond, Price and Hallinan14). Despite these differences, a positive association between BMI and weight loss behaviours appears to be a consistent theme across all adolescent girls(Reference Strauss13, Reference Desmond, Price and Hallinan14, Reference Field, Austin and Taylor23). Given the limitations of BMI-based weight classification in diverse ethnic groups, comparisons with BF levels may provide a more accurate measure. To our knowledge, the relationship between weight control practices and BF has yet to be investigated.
An investigation into the weight-related perceptions and practices of young people from different ethnicities is essential for understanding the barriers to initiating behavioural modifications to achieve a healthy body weight and developing targeted interventions. Thus, the purpose of the present study was to examine the interactions between weight perceptions, weight control and body fatness in a multiethnic sample of adolescent girls. The effects of pubertal development and SES on diet and exercise behaviours were also assessed.
Methods
Participants
A total of 954 girls aged 11–15 years were randomly selected from eleven intermediate and secondary schools in Auckland, New Zealand. Ethnicity was extracted from demographic information stored within school rolls (originally provided by the caregivers of the child upon enrolment). The ethnic composition of the sample was 37·7 % European, 21·6 % Pacific Island, 15·8 % East Asian, 10·2 % Maori, 9·6 % South Asian and 5·0 % other ethnicities. The East Asian ethnic group included 50·3 % Chinese, 31·1 % Korean, 9·9 % Filipino and 8·6 % other East Asian girls. The South Asian group included 91·3 % Indian, 7·6 % Sri Lankan and 1·1 % Nepalese. SES was estimated using the Ministry of Education decile classification system for New Zealand schools. Participants from schools with a decile rating of one to three were categorised into the ‘Low’ SES group, whereas those from schools rated four to seven and eight to ten were considered ‘Middle’ and ‘High’, respectively. Ethical approval for the present study was obtained from the Auckland University of Technology Ethics Committee. A written informed consent was provided by each participant and her legal guardian.
Instruments and procedures
The height of each participant was measured to the nearest millimetre with a portable stadiometer (Design no. 1013522; Surgical and Medical Products, Seven Hills, Australia). Weight in light clothing without shoes was measured to the nearest 0·1 kg on a digital scale (model Seca 770; Seca, Hamburg, Germany). BMI was calculated as weight divided by squared height (kg/m2). BF measurements were obtained using hand-to-foot bioelectrical impedance analysis (BIA). BIA is a rapid and non-invasive technique for estimating BF that is particularly well suited for use in children. Earlier research has shown that population-specific BIA prediction equations generate valid and reliable estimates of BF in paediatric populations(Reference Rush, Puniani and Valencia20, Reference Duncan, Rush and Duncan24). Resistance (R) was measured at 50 kHz using a bioimpedance analyser (model BIM4; Impedimed, Capalaba, Australia) with a tetrapolar arrangement of self-adhesive electrodes (Red Dot 2330; 3M Healthcare, St Paul, MN, USA). After swabbing the skin on the right hand and foot with alcohol, source electrodes were placed on the dorsal surface of the foot over the distal portion of the second metatarsal, and on the hand on the distal portion of the second metacarpal. Sensing electrodes were placed at the anterior ankle between the tibial and the fibular malleoli, and at the posterior wrist between the styloid processes of the radius and ulna. Testing was initiated after the participants emptied their bladder, and had been lying supine with their arms and legs abducted for at least 5 min. Testing was completed when repeated measurements of R were within 1 Ω of each other. Fat-free mass (FFM) was calculated from R, height and weight using two separate ethnic-specific equations previously validated with deuterium dilution in New Zealand children – one specifically for Maori, Pacific Island and European children (r 2 = 0·96, se = 2·44 kg, CV = 8·0 %)(Reference Ellis, Abrams and Wong19) and another for East and South Asian children (r 2 = 0·98, se = 1·49 kg, CV = 5·4 %)(Reference Field, Austin and Taylor24). The procedures used in the present study, including the BIA instrument, were identical to those used to develop the aforementioned FFM prediction equations. Fat mass (FM) was derived as the difference between FFM and body weight, and percentage BF (%BF) was calculated as 100 × FM/weight. Given that there are no generally accepted definitions of adolescent overweight or obesity based on %BF, age-specific percentiles were used to group the sample according to BF status. Overfat/overweight was defined as a %BF > 85th percentile in the current sample.
Participants completed a brief survey that included four questions for assessing weight loss practices and weight perceptions: (i) What are you currently trying to do about your weight (Lose weight, Gain weight, Nothing)? (ii) In the last 7 d, did you diet to lose weight (Yes, No)? (iii) In the last 7 d, did you exercise to lose weight (Yes, No)? (iv) What do you currently think about your weight (Underweight, Normal Weight, Overweight)? To determine pubertal stage, participants were presented with a series of Tanner illustrations and asked to identify their level of pubic hair development. This method of pubertal self-assessment shows an acceptable level of agreement with physician assessment in female adolescents from multiple ethnic groups (r = 0·86)(Reference Neinstein25). Participants were also asked to provide the date of their first period (if menstruating). On the basis of these data, participants were grouped into four stages of pubertal development: Pre-pubertal (no pubic hair, not menstruating), Early puberty (pubic hair, not menstruating), Late puberty (pubic hair, menstruating for <24 months) and Post-pubertal (pubic hair, menstruating for > 24 months)(Reference Murdey, Cameron and Biddle26).
Statistical analyses
Data were analysed using Statistical Package for the Social Sciences statistical software package version 14·0 for Windows (SPSS Inc., Chicago, IL, USA). Differences in participant characteristics (age, height, weight, BMI and %BF) among ethnic groups were assessed by two-way ANOVA, with significant associations examined by pairwise comparisons using Bonferroni post hoc tests. Logistic regression analysis was used to investigate associations between the frequency of diet and exercise practices and age, ethnicity, SES, pubertal status, weight status and BF perception. Odds ratios for each category were adjusted for all six factors concurrently. Ethnic differences in the frequencies of age and SES categories were examined using χ 2 tests.
Results
Table 1 shows the physical characteristics of the study sample. South Asian girls were slightly younger than the other ethnicities (P < 0·05). Body size varied across the ethnic groups: Pacific Island girls were the tallest (P < 0·05), heaviest (P < 0·01) and had the highest BMI (P < 0·01), while East and South Asian girls were shorter (P < 0·05) and lighter (P < 0·05) than the four remaining ethnic groups, and had a lower BMI than Maori and Pacific Island girls (P < 0·01). South Asian and Pacific Island girls had significantly more BF than European and East Asian (P < 0·01), and European, East Asian and Maori girls (P < 0·05), respectively.
Table 1 Participant characteristics

Table 2 shows the perceptions of weight status for the selected BMI and %BF percentile categories. BMI percentile groups were used instead of other BMI-based definitions of childhood overweight and obesity to enable direct comparisons with the %BF percentile groups. Overall, the majority of participants considered themselves to be a normal weight. While few differences in weight perceptions were observed between BMI and %BF percentile groups, there was a relatively high degree of weight misclassification across the distribution. For example, the percentage of girls with a %BF > 85th percentile who incorrectly perceived themselves to be normal weight or underweight was 39·7 % and 4·4 %, respectively. On the other hand, 17·9 % of girls with a %BF < 85th percentile believed that they were overweight.
Table 2 Number of adolescent girls in each BMI and %BF percentile category and their self-diagnosis of weight status
BF, body fat.
Subsequent analyses revealed that overweight perceptions also differed by ethnicity (European, 20·0 %; Maori, 29·7 %; Pacific Island, 30·1 %; East Asian, 17·3 %; South Asian, 20·0 %; P < 0·01). Similarly, ethnic variation was observed in the number of girls participating in weight control practices (European, 37·8 %; Maori, 50·0 %; Pacific Island, 65·0 %; East Asian, 43·6 %; South Asian, 37·4 %; P < 0·01). Figure 1 presents the differences in overweight perceptions and weight control practices across a range of %BF percentile groups. The proportion of girls who consider themselves to be overweight ranged from 0 % to 25 % in the <15th percentile group, and from 48 % to 60 % in the >85th percentile group; the latter finding indicates that many girls who are overweight do not recognise their condition. It is also clear that the number of girls actively trying to lose weight exceeds the number of girls self-diagnosed as overweight, with the extent of the divergence dependent on ethnicity. For example, the proportion of Pacific Island girls who engaged in weight control behaviours was consistently higher than the proportion self-perceived as overweight. In contrast, there was greater agreement between perceptions of overweight and weight-loss practices in South Asian girls (with the exception of those in the >50–85th percentile group).
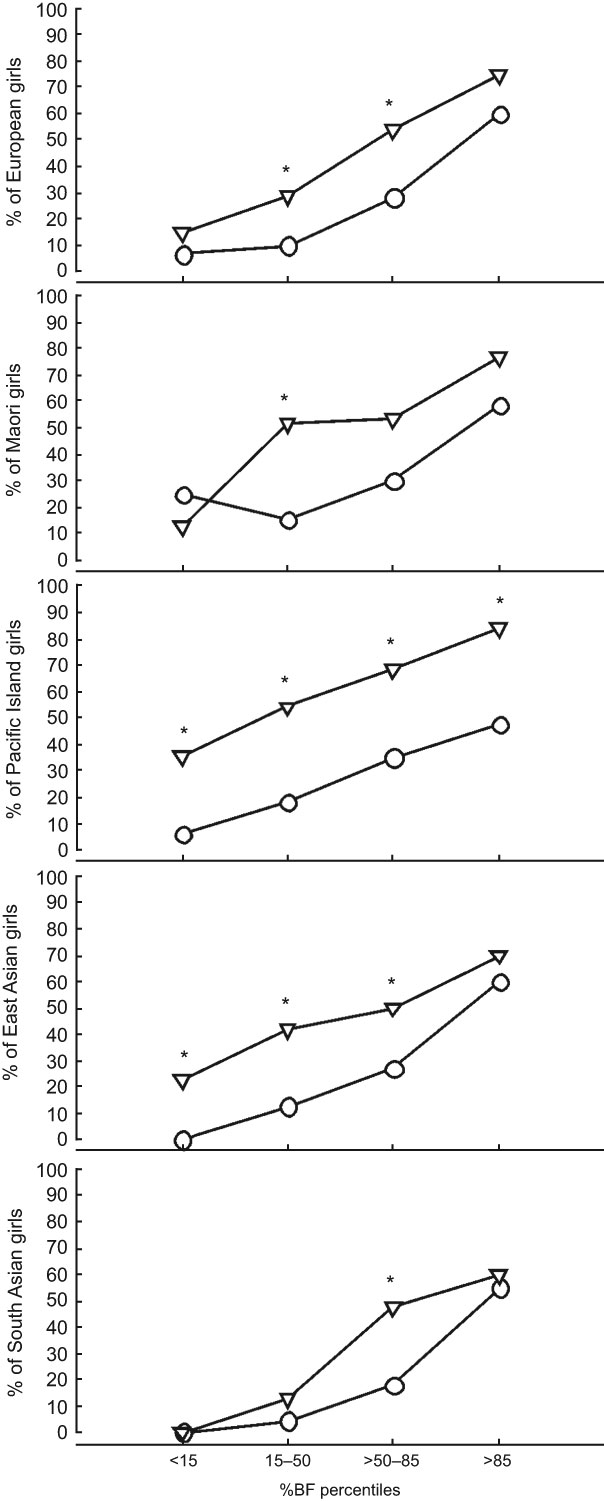
Fig. 1 Perceptions of overweight and the prevalence of weight control practices in adolescent girls (–○–, self-dignosed as overweight; –▿–, trying to lose weight). *Significantly different from self-diagnosis of overweight (P < 0·05)
To further investigate weight control practices in this sample, the frequency of dieting and exercising behaviours were compared in girls who were trying to lose weight (Fig. 2). The combination of both dieting and exercise was the most common weight loss practice reported, although a substantial proportion also relied solely on exercise. Interestingly, 16·4 % of girls who claimed they were trying to lose weight were neither dieting nor participating in exercise. Ethnic variation was also observed, with Maori girls most likely to combine dieting with exercise and South Asian girls most likely to do neither.
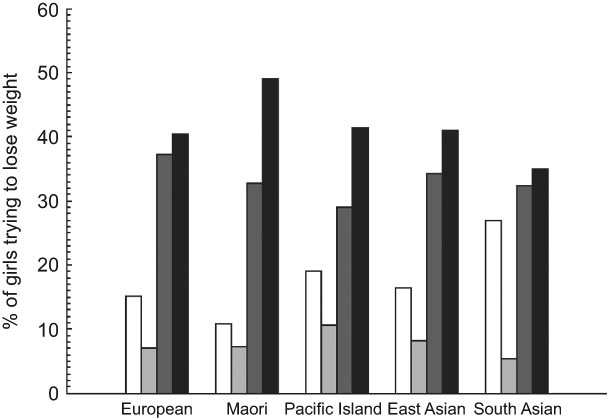
Fig. 2 Prevalence of dieting and exercising in adolescent girls who are trying to lose weight (![]() , neither dieting nor exercising;
, neither dieting nor exercising; ![]() , dieting only;
, dieting only; ![]() , exercise only;
, exercise only; ![]() , dieting and exercising)
, dieting and exercising)
Table 3 displays the unadjusted and adjusted OR for dieting to lose weight within each of the variables assessed in the present study. Unadjusted analyses revealed significant associations between dieting and age, ethnicity, SES, pubertal status, BF status and weight perception. However, ethnicity, BF status and weight perception were the only variables that remained significant after controlling for variation in all other factors. The adjusted data indicate that Pacific Island girls were 1·8 times more likely to diet than European girls, with no significant differences between European girls and any other ethnic group. In addition, participants were more than two times more likely to diet if they had a %BF > 85th percentile. Perception of weight status had the greatest effect on the odds of dieting in this sample, with girls self-diagnosed as overweight more than three times as likely to diet than those who perceived themselves to be underweight.
Table 3 Correlates of dieting to lose weight in adolescent girls
SES, socio-economic status.
*Adjusted for all other factors.
†Significantly different from reference group (P < 0·05).
‡Significantly different from reference group (P < 0·01).
The odds ratios associated with exercising to lose weight were also calculated (Table 4). The effects of age, ethnicity, pubertal status, BF status and weight perception were significant in the unadjusted model. Age, ethnicity and weight perception remained significant in the fully adjusted model. Older girls were more than twice as likely to participate in exercise as younger girls, and South Asian girls were less likely to exercise than European girls. As with dieting, weight perception showed the strongest association with exercising practices. Girls classified as overfat were also more likely to exercise, although this association was just outside the threshold of statistical significance.
Table 4 Correlates of exercising to lose weight in adolescent girls
SES, socio-economic status.
*Adjusted for all other factors.
†Significantly different from reference group (P < 0·05).
‡Significantly different from reference group (P < 0·01).
Discussion
Given the escalating prevalence of youth obesity around the world and the severity of related complications, it is essential that young people are able to recognise a state of excess BF. Indeed, an underestimation of weight status will likely prevent overweight adolescents seeking advice and initiating behavioural changes. The results presented in the present study provide an indication of a mismatch between perceived weight status and actual BF levels in a large proportion of adolescent girls. This builds upon earlier work that investigated such relationships with BMI and/or weight in limited ethnic groups(Reference Brener, Eaton and Lowry7–Reference Neumark-Sztainer, Croll and Story11). Nearly half of the girls with high BF thought that they were normal or underweight, and a reasonable proportion who did not have excess BF thought that they were overweight. In addition, there were noticeable differences among ethnicities; the frequency of girls with high BF who did not recognise their condition ranged from 40 % in European and East Asian girls to 52·3 % in Pacific Island girls. Such variation in the perception of excess BF may reflect fundamental differences in cultural norms; a large body size can be considered a sign of wealth and prestige in traditional Pacific Island families (although this custom has become diluted in Westernised societies)(Reference Craig, Swinburn and Matenga-Smith27). Thus, being large may not carry the same negative implications in Pacific Island communities than in those from other ethnicities(Reference Brewis, McGarvey and Jones28). Pacific Island children also have the highest prevalence of BMI-determined obesity of all major ethnic groups in New Zealand(29), which may result in the normalisation of excess BF in Pacific populations. The identification of ethnic differences in the ability to classify overweight status will assist in prioritising groups for initiatives to improve self-awareness; however, qualitative research into the underlying cultural norms that influence perceptions of body size may be necessary to ensure that such interventions are appropriate for each ethnicity.
The ethnic variation we observed in the underestimation of excess BF is consistent with earlier research using universal BMI standards to define obesity in adolescent girls from multiple ethnic groups(Reference Brener, Eaton and Lowry7, Reference Neumark-Sztainer, Croll and Story11, Reference Strauss13, Reference Desmond, Price and Hallinan14). Furthermore, the degree of divergence between perceived and measured body size was similar regardless of whether BMI or %BF percentiles were used. These findings were unexpected given the evidence that BMI is not an equivalent predictor of BF across multiple ethnicities(Reference Deurenberg, Deurenberg-Yap and Foo15–Reference Daniels, Khoury and Morrison21). We suggest that these results may reflect the use of weight-related terminology (under-, normal- and overweight) for describing BF status and the closer relationship between these terms and a weight-related index such as BMI when compared with %BF. Nevertheless, the potential diagnostic error associated with the use of BMI in multiethnic populations does not appear to be a major factor when assessing the perceptions of overweight in adolescent girls.
The results from the present study also revealed that a relatively large proportion of girls who did not perceive themselves as overweight were actively trying to lose weight. This trend may be symptomatic of the firmly established societal desire to be slim, a pressure that tends to assume particular importance in adolescent girls(Reference Stice, Spangler and Agras30). With continuous exposure to images and expectations of unrealistic body shapes that promote weight loss regardless of body size(Reference McVey, Tweed and Blackmore5, Reference Field, Camargo and Taylor6), engaging in unnecessary weight loss practices is perceived as acceptable and even desirable in some adolescent peer groups(Reference Neumark-Sztainer and Hannan31). Another potential explanation is that some non-overweight girls may be persisting with weight loss practices from a period when they were overweight. Our data also clearly indicated that the extent of the divergence between weight perceptions and weight loss practices across the different %BF percentiles was dependent on ethnicity. The number of Pacific Island girls trying to lose weight, for example, was consistently higher across all BF categories than the number who considered themselves overweight. This points to an embedded cultural expectation that Pacific Island girls should be trying to lose weight, regardless of their personal perceptions. In contrast, South Asian girls had a high level of agreement between perception and practice in all but the >50–85th percentile group. Together, these findings reinforce the need to communicate weight-related issues with care in adolescent girls, and the importance of tailored approaches for populations with diverse ethnicities and cultures.
An understanding of the behavioural responses to a perception of overweight is valuable for determining acceptable approaches to promote weight loss and achieve a healthy body weight. Of the girls who were attempting to lose weight, the combination of dieting and exercising was the most common weight loss practice reported across all ethnic groups, followed by exercising. This finding suggests that dieting and exercising are both acceptable methods of weight control for adolescent girls from multiple ethnic groups. Interestingly, the number of girls who were trying to lose weight but reported neither dieting nor exercise to do so exceeded those that reported dieting alone. It is also possible that some of the girls who were dieting and or exercising for weight loss may not have done so in the previous 7 d, and thus these behaviours were not picked up in the assessments. Whether this subset of girls are participating in other weight control behaviours or simply recognise their condition but are not motivated to make behavioural changes cannot be determined from the present study. Additional research focusing on the qualitative aspects of approaches to weight loss would be helpful for understanding why a particular behaviour was initiated.
A potential limitation of the present study was the self-assessment of pubertal status. Clearly, the criterion method is assessment by a trained physician; however, the ethical issues surrounding the undressing of adolescent girls precludes the use of this technique in population research. We suggest that the use of Tanner illustrations – validated previously in a multiethnic sample of female adolescents(Reference Neinstein25) – is the most suitable alternative to physical assessment, providing participants with standardised visual cues with which to judge their pubertal development. It should also be noted that the questions used to determine weight perceptions in the present study were not validated due to the lack of practical criterion measures for determining weight control practices and perceptions.
The present study is the first to investigate both dieting and exercise practices for weight loss and to compare these with measurements of BF and weight perceptions in multiple ethnic groups. Although participants were more likely to be exercising or dieting to lose weight if they were classified as overfat, our results indicate that an individual’s weight status perception was a stronger predictor of weight loss intent than actual BF, when controlling for all other factors. This finding shows that self-diagnostic inaccuracies in classifying weight status would be likely to flow on to weight control behaviours, and thus, the importance of educating girls about how to correctly classify their body size. While ethnic and age variation in the frequency of dieting and exercise was also observed, the effects of SES and pubertal status were only significant when analysed separately.
Conclusions
Overall, adolescent girls from a diverse range of ethnic groups tended to be poor at accurately classifying their weight status. The presence of weight misclassification across the range of BF categories (normal weight girls perceiving themselves as overweight and girls with high BF perceiving themselves as normal or underweight) shows the conflicting issues of body size perceptions that exist in this group. Thus, interventions in this subgroup of the population should focus on delivering clear, consistent messages that promote a healthy weight rather than simply weight loss. With regard to weight loss practices, evidence of strong positive relationships between measured BF status and the frequency of weight loss practices across all ethnic groups was promising. However, given that perceived weight status was more strongly associated with dieting and exercising behaviours, and that a substantial proportion of girls were unable to correctly classify themselves as overweight, educational programmes that assist girls in recognising a state of excess BF are a priority to increase the likelihood that behavioural changes necessary to combat widespread overweight and obesity are adopted.
Acknowledgements
The present study was supported by project grants from Sport and Recreation New Zealand and the School of Sport and Recreation, Auckland University of Technology. All authors were involved in the conception and design of the study. J.S.D. and E.K.D. were responsible for data collection and statistical analyses. All authors contributed to writing and approved the final manuscript. The authors have no conflicts of interest to declare.






