



The global use of advertising through digital media continues to increase, but it is virtually unregulated, especially as it affects children and adolescents(1–Reference Potvin Kent, Pauzé and Roy3) and is scarcely monitored(Reference Kelly, Vandevijvere and Freeman4–Reference Clarke and Svanaes6). Common social media platforms are Facebook, Instagram and Snapchat(Reference Kelly, Vandevijvere and Freeman4). These collect large amounts of personal use information and use specific algorithms to reach target audiences with customised messages(Reference Wind and Mahajan7). Young people as prolific users of digital media are very susceptible to this type of personalised marketing(2). It is an important, but major challenge for society to protect vulnerable groups like children and adolescents from commercial exploitation. In particular, food and beverage preferences and behaviours continue to develop through childhood and adolescence and can contribute to obesity and nutrition-related diseases(Reference Hastings, Stead and McDermott8–Reference Kelly, Baur and Bauman12). There is less opportunity for parents to influence exposure to marketing for unhealthy products through digital media than through broadcast media, and such marketing normalises the consumption of unhealthy food and beverages(Reference Kelly, Vandevijvere and Freeman4–Reference Clarke and Svanaes6,Reference Vandevijvere, Aitken and Swinburn13–Reference Halford, Gillespie and Brown15) .
Previous studies have shown that food and beverage advertising to children and young people through more traditional media such as television is overwhelmingly for unhealthy products(Reference Vandevijvere, Aitken and Swinburn13,Reference Kelly, Halford and Boyland16–Reference Jenkin, Signal and Smith20) . This is likely to be the case for marketing through digital media, as shown by a previous study of the Facebook pages of major food companies(Reference Vandevijvere, Aitken and Swinburn13). New Zealand teens engage with a range of digital media platforms, with four in ten currently using five or more digital media platforms(21). When asked which ones they use most often, 25 % mention YouTube, followed by those mentioning Facebook and Snapchat with 23 % each, and Messenger and Instagram (13 and 11 %, respectively). Facebook was selected for this study due to Facebook’s popularity among adolescents and the potential for industry to specifically target advertising to Facebook users based on a wide range of personal characteristics and preferences.
Research addressing this topic is difficult for multiple reasons such as a reduced ability to monitor online advertising because it is personalised, highly targeted and received through multiple personal devices. Currently in New Zealand, advertising is voluntarily regulated by the Advertising Standards Authority. Voluntary initiatives internationally poorly address digital media advertising and do not protect children and adolescents who are most vulnerable to marketing messages(5,22,23) .
The main aim of this study was to test the feasibility of monitoring the exposure of adolescents aged 16–18 years to food and beverage advertising through Facebook using a browser extension that identifies and retrieves advertising from the Facebook newsfeed of participants. The secondary aim was to examine adolescents’ exposure to unhealthy food advertising on Facebook and to evaluate the healthfulness of this advertising and the persuasive techniques used(24,25) .
Methods
The study was approved by the University of Auckland Human Participants Ethics Committee. Adolescents aged 16–18 years old were recruited as younger children were more difficult to recruit given the more onerous two-step consent process requiring parental consent. Previous protocols developed by the International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Support (INFORMAS) on food and beverage marketing to children on traditional media such as television and print advertisements, informed the approach and methods utilised in classifying the advertisements and the list of persuasive techniques(26).
Recruitment
The target study population of 16–18 year olds was recruited through convenience sampling using paid Facebook advertisements and field recruitment from schools, sports clubs and community groups. Promotional materials such as videos and posters were used to explain why the study was being conducted and the technical requirements for installing the browser extension, including having a personal device, running the desktop version of Google Chrome as solely operated by the adolescent, meaning that mobile devices and school devices were excluded.
Participants were recruited over a 5-month period. A koha (gift) of a $20 shopping voucher was provided to each participant who signed up during the field recruitment stage, while those who signed up during the online media recruitment stage entered a draw to win one of three $50 shopping vouchers.
Chrome browser extension
The browser extension (AdHealth) used to collect the advertisements seen by participants when they scrolled through their Facebook newsfeed was developed in JavaScript by the University of Auckland’s Centre for eResearch(27,28) . The extension was made available on the Google Chrome Web Store to download. A promotional website marketed through Facebook itself was developed to enable participants to download the extension and, after their approval, link it to their Facebook account on their personal computer. The AdHealth extension went through numerous iterations of pre-testing by the Centre for eResearch prior to use for this study, to ensure confidence in the extensions’ duties in retrieving data from the advertisements. The extension was tested by a group of researchers at the University of Auckland where the ads captured were compared with what they saw in their Facebook newsfeeds to make sure all advertisements were captured. AdHealth detected when users were on Facebook through the URL and which advertisements were actually seen when scrolling through their newsfeed. The advertisements seen, including the duration of exposure (i.e., how long they were visible on the screen), were then recorded in an online database where each user and advertisement received a unique ID. The extension only worked when the user was online using a desktop or laptop computer, not a smart phone or tablet.
The installed extension could be deleted at any time, meaning participants were able to withdraw from the study. Information was extracted by parsing the Document Object Model tree representation of Facebook web pages. The Document Object Model tree contains all the information used by the browser to render a webpage on the screen, with tree elements closer to the root representing larger areas of the layout and elements further away from the root representing details such as text and images. Identifiers are associated with these elements, which the browser extension uses to retrieve the relevant information from Facebook. This information was sent to a web server with a database, which compiled this information from all the browsers of users with AdHealth installed.
The classification of advertisements by nutritional quality
Nutritional information of the advertised products, when required for classification, was collected using the University of Auckland Nutritrack database(29) or other online sources such as from food retailers. The information collected included key macronutrients, such as saturated fat and sugar, and Na as listed in the Nutrient Information Panels per serving and per 100 g. The advertisements in the online database were classified manually as permitted (healthy) or not permitted (unhealthy) to be advertised to children according to the WHO-EURO nutrient profile model. The WHO-EURO model was specifically designed for restricting the marketing of less healthy foods to children. It encompasses seventeen food categories, including fruit, vegetables and readymade meals. Certain food categories are not permitted to be marketed to children under any circumstances. These include chocolate and confectionery, cakes and sweet biscuits, juices and energy drinks. Conversely, unprocessed meat and fish and fresh/frozen fruit and vegetables can be marketed without restriction. Maximum nutrient level cut points are applied to determine the eligibility of foods in all other categories to be marketed to children.
Coding of advertisements
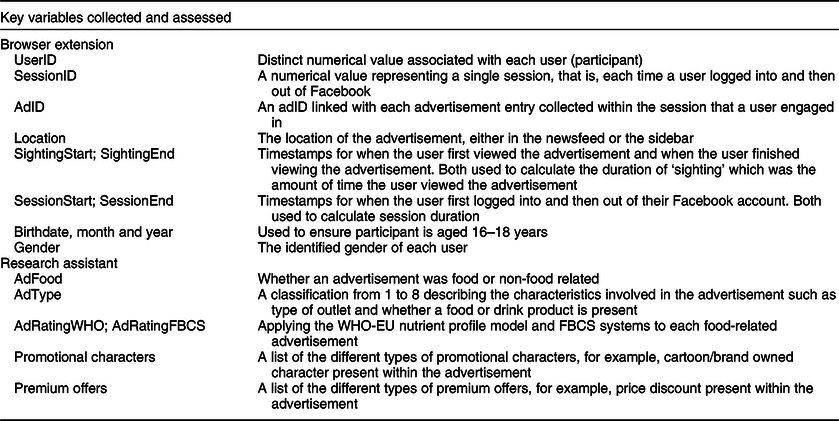
Variables of interest collected by the browser extension for each advertisement entry included userID, sessionID, adID and URL to view the advertisement. This information was then supplemented by a research assistant manually classifying whether: the advertisement was food or not food related; the healthiness of the foods advertised according to the WHO-EURO nutrient profile model and the display of promotional characters or premium offers within the advertisements. The key variables are described in Table 1. Birth date and gender were the only personal data collected from each participant. When the ad ID and/or text or image were the same, this meant the user saw the advertisement more than once. The advertisements appeared in either the sidebar (a panel on the right-hand side of Facebook’s user screen) or the newsfeed (information within the middle of the page).
Table 1 Key variables collected for each advertisement entry
Classification of ads on nutrition information
The healthiness of each food product was classified using the WHO-EURO Nutrient Profile Model, which is suitable to assessing packaged food products marketed to young people in New Zealand(25,Reference Mhurchu, Mackenzie and Vandevijvere30) . Advertisements consisting of a product that was not specific enough to be classified (i.e., lacking required nutritional information) were deemed ‘non-specified’ such as advertisements for some bakery items where the picture was unclear to identify specific products. Advertisements that did not include a specific product and instead promoted a food or beverage brand were classified as ‘brand advertisements’. Products advertised, where the products’ food category is omitted from the WHO nutrient profile guidelines, were classified as ‘non-applicable’. This included products such as protein shakes and powders. If multiple products were in one advertisement, then all the included products had to meet the nutrient profile thresholds to be deemed permitted. If at least one product was not permitted, then the overall advertisement would be classified as not permitted. A protocol was developed based on prior work by INFORMAS, to document and explain the decisions made during data analysis, including classifying the healthiness of the food and drink advertisements(26,Reference Kelly, King and Baur31) .
Assessment of persuasive techniques
The data were analysed using IBM SPSS Statistics 25 for key indicators to describe the users and advertisements: the number of users and their total exposure time, the number and proportion of permitted and not permitted food advertisements, the exposure time to permitted and not permitted food advertisements, the proportion of not permitted and permitted food advertisements with promotional characters and/or premium offers, and the proportion of advertisements seen by more than one user. The persuasive techniques involved two categories of (1) promotion characters and/or (2) premium offers. Promotional characters are techniques used to directly promote the associated products, including cartoon/company-owned characters, licensed characters, amateur sportspersons, non-sports celebrities, movie tie-ins, famous sportspersons and ‘for kids’ messaging. Premium offers included game and app downloads, contests, ‘Pay 2 take 3’ or other, ‘20 % extra’ or other, limited edition offers/products, social charities, gifts or collectibles, price discounts or loyalty programmes.
Duplicates and advertisements seen by only one user were included to ensure the total exposure of advertisements seen by users was analysed. All results, such as exposure duration, were analysed by userID and sessionID. The advertisements for products that were other than foods or beverages were used to calculate the proportion of all advertisements that were for food and beverages. The frequency of food advertisements was used to calculate the number of advertisements seen by more than one user. Advertisement entries with the same adID and/or text and image of the advertisement that had a different userID were counted. If the same advertisement entry was seen more than once, it was counted according to the number of entries associated with that particular advertisement. A small number of advertisement entries (n 38) did not have any data for the variables ‘sessionend’ and ‘sightingend’, which means the duration of sessions and/or exposure was unable to be determined. This occurred when participants either did not officially log out of their Facebook account or the computer screen of participants was abruptly turned off.
Results
Exposure to advertisements
A total of thirty-four adolescents aged 16–18 years participated in the study, with the total number of days of participation of 1535 d, with a range of 1–200 d. The total time spent by users on Facebook across sessions was 164·1 h, with 34·4 (17 %) h of this time being allocated to users viewing and being exposed to advertisements. Four percentage of the total advertisements (n 4973) seen were food-related (204 advertisements). Two-thirds (139, 68·1 %) of food-related advertisements were located within the newsfeed and the remaining (65, 31·9 %) were located in the sidebar. The mean exposure to food advertisements was 5·9 (sd = 2·5) and 4·8 (sd = 2·5) for not permitted food advertisements per hour of Facebook use. The most frequent brands/companies targeting users across all food-related advertisements were Burger King (18 %), Nutri-Grain (10·8 %), Dominos (9·4 %), Coca-Cola NZ (7·9 %) and Japan Crate (7·2 %) (Fig. 1).
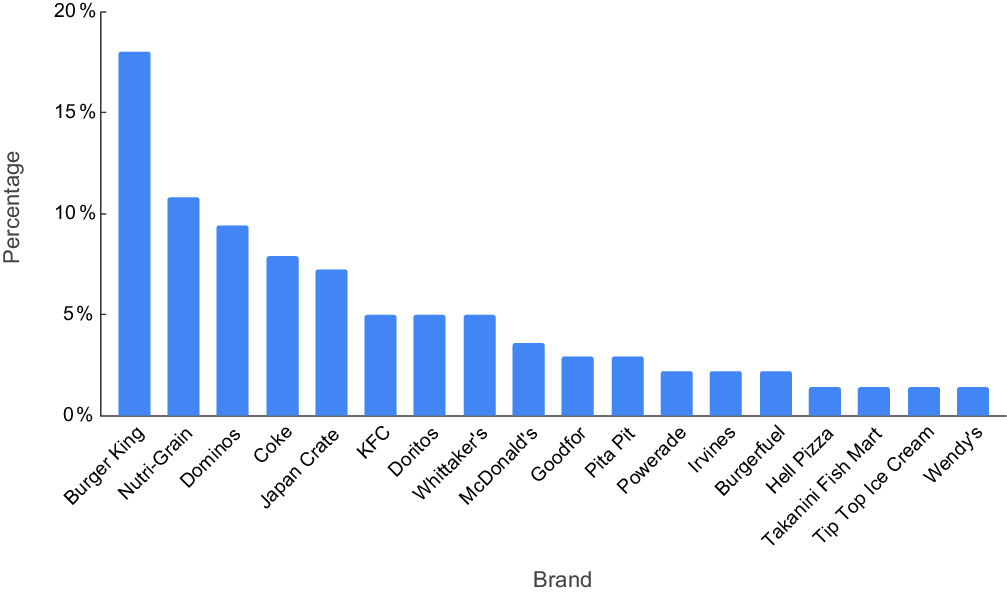
Fig. 1 Most frequent food brands exposing their advertising to New Zealand adolescents on Facebook
According to WHO-EURO nutrient profile model, 166 (81·4 %) were for not permitted foods, three for 224 (1·5 %) permitted foods and 20 (9·8 %) were brand related over the study period (Fig. 2). Once excluding the brand-related advertisements, 98·22 and 1·78 % of food-related advertisements had a not permitted food advertisement and permitted food advertisement, respectively. The product details were not specified in twelve (5·9 %) advertisements and three (1·5 %) were non-applicable (coffee, tea, protein powder, protein shakes, etc.). The mean exposure time to unhealthy (not permitted) food advertisements on the users’ screen was 32 s on average.
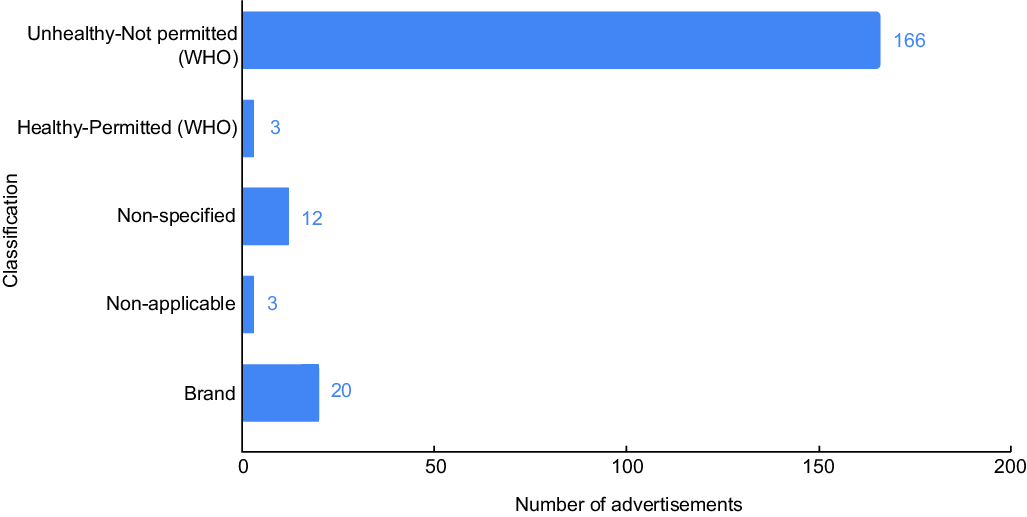
Fig. 2 Classification across all advertisement entries by WHO-EURO nutrient profiling model
For persuasive techniques, there were promotional characters for 56 (56/166, 33·7 %) of the non-permitted food advertisements with a cartoon/brand-owned character (26/56, 46·5 %) and/or non-sports/historical event/festival (18/56, 32·2 %) being the most common promotional character types. Less common promotional characters were characters for kids, movie tie-ins, sports events and a famous person. There were 53 (53/166, 31·9 %) instances of premium offers: price discount (23/53, 43·4 %), gift or collectable (12/53, 22·6 %), limited edition (12/53, 22·6 %) and Buy 2 Get 1 Free or similar (6/53, 11·3 %). Within the permitted food advertisements (n 3), there was only one instance of a promotional character and none of the premium offers.
Exposure per user
In total, users engaged in 3645 Facebook sessions (mean per user = 107; range from 1 to 1185; sd = 266), with a total Facebook time for all users across sessions of 9848 min (mean per user = 290; range from 0·09 to 2471·76; sd = 668). The total exposure time for all users across advertisement exposures within these sessions was 2061 min (mean per user = 61; range = from 0·008 to 682·15; sd = 152). Of the exposure time to advertisements among users, 98·9 and 1·1 % were for non-food and food related advertisements, respectively. For food-related advertisements, this translates to 23 min and, of this, 18 min (99·8 % of the total food-related exposure time) was for unhealthy (not permitted) advertisements. This contrasts to 0·04 min (0·2 % of total food-related exposure time) for healthy (permitted) advertisements in exposures across all users. Overall, of the 23 min, the remainder was 2·9 min for brand advertisements, and 0·7 min for non-applicable and non-specified advertisements each.
Discussion
Despite a small overall percentage of advertisements seen by adolescents through Facebook being food-related, the vast majority of these advertisements were for unhealthy food and beverages. The absolute number of 166 not permitted advertisements is also important to consider, with users exposed to an average of 4·8 (sd = 2·5) not permitted food advertisements per hour of Facebook use. This is one of the first studies to test a method of electronically collecting exposure of unhealthy food advertisements as experienced by adolescents through a social media platform (Facebook). While a minority of advertisements were food related, those advertisements were overwhelmingly for food and beverage products classified as unhealthy by WHO-EURO nutrient profile model. There was a high use of persuasive techniques in promotional characters (33·7 %) and premium offers (31·9 %) within the unhealthy food advertisements. The mean exposure time to unhealthy food advertisements on the users’ screen was 32 s per user or 1 % of the total Facebook time. Key policy recommendations include strengthening international options to address food marketing on social media, ensuring that food brands and companies are unable to target young people on social media with not permitted food advertising and educating young people and parents about the harmful effects of unhealthy food marketing.
Other studies using a range of methods to investigate food and beverage marketing on various digital media platforms also found the majority of ads to be for unhealthy foods. A 2019 study assessed the frequency and healthiness of food marketing seen by children and adolescents aged 7–16 years on digital media apps including Facebook, Instagram, Snapchat, Twitter and YouTube(Reference Potvin Kent, Pauzé and Roy3). Of the 108 participants, 72 % were exposed to food marketing, with adolescents being particularly targeted. The highest promoted products were unhealthy products including fast food(Reference Potvin Kent, Pauzé and Roy3). A New Zealand study(Reference Jenkin, Signal and Smith20) found food marketing on Facebook to be comprehensive with some marketing techniques unique to Facebook. Two researchers became ‘fans’ of twenty major food brands and products, monitoring their ‘newsfeed’ and ‘posts’. A New Zealand study of websites of food brands popular with children and adolescents, rather than digital media pages, found a variety of marketing techniques and features were used similar to the current study(Reference Vandevijvere, Sagar and Kelly32). The overall mean exposure to unhealthy food advertisements of 4·8 was slightly lower compared with literature on food advertising in traditional media such as television advertising(Reference Vandevijvere, Soupen and Swinburn18). Vandevijvere et al.(Reference Vandevijvere, Soupen and Swinburn18) reported 9·1 as the mean hourly rate of unhealthy food advertising.
The experience of implementation
This relatively low exposure to food advertisements could be due to the adolescents within the study interacting more with non-food advertisements. There is an absence of literature on how stimulating adolescents and children find food advertisements compared with non-food advertisements to validate this conclusion. There is therefore a gap in the literature requiring attention among researchers. Overall, the Google Chrome browser extension was simple to use and suitable as this was the most commonly used web browser by the target audience. Despite some inconsistencies in the data collected by the extension, it was comprehensive and simple to interpret. This extension can further be applied to other web browsers such as Mozilla Firefox and Microsoft Edge using the Google Application Programming Interface.
This pilot uncovered significant lessons to be considered for larger studies. Firstly, the recruitment process for participants proved challenging and would be more so for recruiting younger participants. Online advertising for study participants was largely ineffective and more successful recruitment involved visiting schools to recruit participants in-person. The AdHealth web extension was not available for mobile devices or tablets, which required individuals to bring their own laptops to the recruitment session. This did not commonly occur, so an alternative was for the individual to send a screenshot to the research assistant showing that the extension was installed on their computer and linked to their Facebook account for verification purposes.
The ability of the browser extension to provide the quantitative data required for this study was mixed in the developmental stages before the pilot started. A substantial number of advertisements did not have a userID or sessionID because Facebook’s code structure was constantly changing, meaning that the browser extension needed to be consistently altered to ensure that the extension functioned to retrieve the required information. Therefore, the browser extension or tool needs to be constantly monitored and changed where necessary. Obtaining the participant’s age was not always possible due to the settings some users have on their Facebook accounts. It is critical to know the participant’s age for monitoring food marketing to children. This could be obtained during the consent process.
Limitations
A limitation of this study is that the age bracket of 16–18 year olds was too narrow, as research has shown that food and digital marketing is more pervasive among younger adolescents and children(5,Reference Vandevijvere, Sagar and Kelly32,Reference Tatlow-Golden, Tracey and Dolphin33) , although this might be due to the dominance of literature assessing food marketing that predominately involves children, not teenagers. Younger children are more vulnerable to online advertising and companies use users’ personal data to target them(5,Reference Vandevijvere, Aitken and Swinburn13,Reference Moore and Rideout34,Reference Lascu, Manrai and Manrai35) . This personal data is not available to researchers to expose this problem, shown by the difficulty of obtaining ethics approval for this pilot when involving a younger target audience. For future research, this means different recruitment and consent processes will be needed to study the exposures in these younger populations. Additionally, the previously mentioned challenge in the relatively narrow scope of social media coverage (only Facebook through a computer) is an additional limitation. These limitations are important to consider as the previous literature has reported higher exposure rates than within this study, which is likely due to these limitations.
The extension provided limited information for the sidebar location compared with the newsfeed location of advertisements, which is vital as one in three food-related advertisements was found in the sidebar. This impacted the ability to classify the healthiness of sidebar advertisements, for example, finding the nutritional information for a product in a sidebar advertisement was more difficult than for a newsfeed advertisement. The ability to extract this information is likely to be under the control of the programmers at Facebook. The web links to the advertisement entries’ pictures or videos expired, so entries needed to be captured immediately by downloading or saving the pictures or videos of the advertisements and inserting detailed comments within the database to describe the nature of the advertisement.
Implications for future research
Assessing advertisements only on Facebook feeds provides a limited snapshot of exposure. Young people also use other digital media platforms such as Snapchat and Instagram(2). Broadening the AdHealth extension to these additional digital media platforms is potentially feasible. However, platforms, such as Snapchat, require access through a mobile application, which does not allow people to add extensions. To mitigate this, a separate mobile application would need to be developed that accesses people’s accounts on their digital media application and gives permissions for the application to collect information on the advertisements seen by the user. These components would be added to the tracking technology used in the AdHealth extension. Enabling these higher privileges demands a high degree of trust between participants and researchers and safeguards for personal data security. A potential option is for participants to install an alternative digital media app to use in place of the original digital media application for the duration of the study to enable the study to be conducted with a mobile device on which this age group is likely to spend more time on digital media.
The WHO CLICK tool was recently developed to assist the monitoring of digital marketing of unhealthy products to children and proposes screen recording of smartphone activity over several days. It could be considered for future research. This will be useful given the amount of time 16–18 year olds spend on digital devices such as smartphones and tablets compared with computers, and other digital media platforms such as Instagram(2). Smartphone ownership for teenagers has been found to be nearly universal regardless of gender, ethnicity or socioeconomic background(36). Access to computers is less universal and varies by income. It is likely that the results significantly underestimate our samples’ and potentially adolescents’ overall exposure to digital food marketing.
Conclusion
Almost all the food advertisements viewed by adolescents in this study were for unhealthy products and a high number of persuasive techniques were used, despite the minority of advertisements being food related compared with non-food advertising. Still, on average, five advertisements for unhealthy foods were seen per hour spent on Facebook. This is substantial and requires action. Governments have a responsibility not only to protect children from commercial exploitation but also to monitor the compliance of companies with government regulations and policies for marketing to children. Key policy recommendations involve ensuring that food brands and companies are unable to target young people on social media with not permitted food advertising, strengthening international options to address food marketing on social media and educating young people and parents about the harmful effects of unhealthy food marketing.
Acknowledgements
Acknowledgements: The authors thank the number of people who helped during the recruitment stages of the study to obtain our sample size. This includes Kathryn Moore (Tamaki College), Gordon Robertson (Glendowie College), Nicole Stevens (Manurewa High School), Keith Denne (Papatoetoe High School), Selah Hart and Lineti Latu (Hāpai Te Hauora) and the Massey Raise Up Crew. The authors thank Bianca Haux at the Centre for eResearch who helped supervise the implementation of the AdHealth browser extension during the data collection stage. Financial support: This research was funded by a University of Auckland, School of Population Health, Performance-based Research Fund. Conflict of interest: None. Authorship: B.K. contributed to the study conception and design, and led the data collection, analysis and writing of the manuscript. S.M. contributed to the study conception and design, data analysis and assisted with writing and critically revised the manuscript. B.S. contributed to the study conception and design and critically revised the manuscript. C.L. contributed to the study conception and critically revised the manuscript. S.V. led the study conception and design, and assisted with data collection, analysis and critically revised the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the University of Auckland Human Participants Ethics Committee. Written informed consent was obtained from all subjects/patients.



