
17 results
Relationship between chlorhexidine gluconate concentration and microbial colonization of patients’ skin
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 28 May 2024, pp. 1-6
-
- Article
- Export citation
Impact of universal chlorhexidine bathing with or without COVID-19 intensive training on staff and resident COVID-19 case rates in nursing homes
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 March 2024, pp. 1-4
-
- Article
- Export citation
Surveillance of healthcare-onset clinical cultures using whole-genome sequencing reveals hidden nosocomial transmission
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s83-s84
-
- Article
-
- You have access
- Open access
- Export citation
-
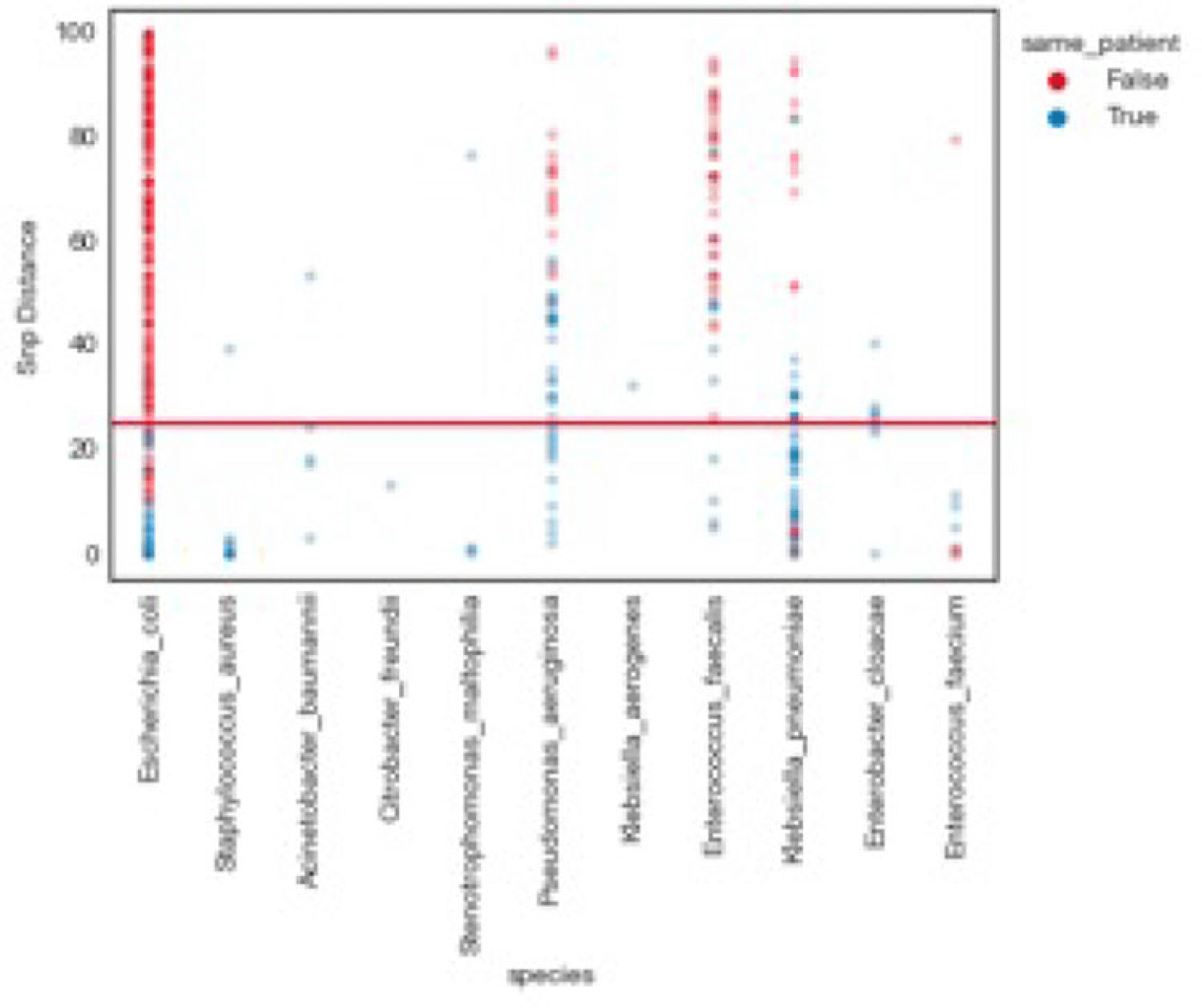
Background: Traditional hospital outbreak-detection methods are typically limited to select multidrug-resistant pathogens in a single unit, which can miss transmission of many medically important healthcare-transmissible pathogens. Whole-genome sequencing (WGS) enables comprehensive genomic resolution for accurate identification of clonal transmission. Previously, lack of scalability limited the use of WGS for hospital surveillance. Methods: We conducted prospective surveillance of select bacteria from all inpatient clinical cultures plus all bacteria from clinical cultures from ICUs and oncology units at the University of California Irvine (UCI) Clinical Microbiology Laboratory from September 2021 to February 2022. Due to pandemic stressors, this pilot test was a prelude to a real-time demonstration project. Its goal was to demonstrate the efficiency and scalability of the WGS platform when receiving samples monthly and analyzing results quarterly without the intent for real-time response. Bacterial isolates slated for discard were collected weekly and sent monthly to Day Zero Diagnostics for sequencing. In total, 1,036 samples from 926 patients were analyzed for genomic relatedness, a scalable and automated analysis pipeline already in use for rapid (days) characterization of genomic-relatedness in small and large sets of isolates. Mapping and SNP calling was performed against high-quality, best-match reference genomes. Sets of samples with pairwise distance of 2 persons with genomically related isolates and were denoted as “clusters.” Separately, we also investigated within-patient diversity by quantifying the genomic relatedness of isolates collected from individual patients. Results: Isolates represented 28 distinct species. We identified 10 Escherichia coli clusters (range, 2–4 patients; median, 2 patients), 2 Klebsiella pneumoniae clusters (range, 2–4 patients), and 1 Enterococcus faecium cluster (3 patients). All but 1 involved genomically matched isolates from multiple hospital locations. There were 4 Escherichia coli ST131 clusters spanning 4 months, including 1 with 4 patients across 3 different hospital locations. At a species level, there were distinct differences between the observed SNP distances between samples isolated from the same versus different patients (Fig. 1). All identified clusters had not been flagged by routine outbreak detection methods used by the UCI infection prevention program. Conclusions: Comprehensive WGS-based surveillance of hospital clinical isolates identified multiple potential transmission events between patients not in the same unit at the time cultures were taken. Combining WGS detection and real-time epidemiologic investigation may identify new avenues of transmission risk and could provide early warnings of clonal transmission to prevent larger outbreaks. High-volume surveillance of hospital isolates can also provide species- and context-specific clonality.
Financial support: This study was funded by Day Zero Diagnostics.
Disclosures: None

Bloodstream infection burden among cancer clinic patients with PICC Lines: A prospective, observational study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s49
-
- Article
-
- You have access
- Open access
- Export citation
-
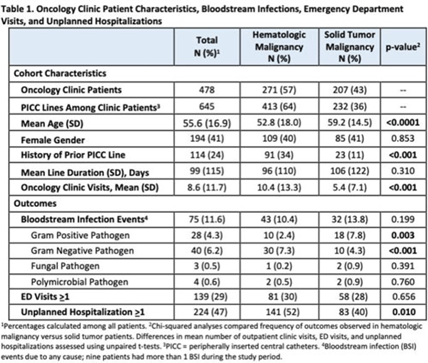
Background: Oncology patients are at high risk for bloodstream infection (BSI) due to immunosuppression and frequent use of central venous catheters. Surveillance in this population is largely relegated to inpatient settings and limited data are available describing community burden. We evaluated rates of BSI, clinic or emergency department (ED) visits, and hospitalizations in a large cohort of oncology outpatients with peripherally inserted central catheters (PICCs). Methods: In this prospective, observational study, we followed a convenience sample of adults (age>18) with PICCs at a large academic outpatient oncology clinic for 35 months between July 2015 and November 2018. We assessed demographics, malignancy type, PICC insertion and removal dates, history of prior PICC, and line duration. Outcomes included BSI events (defined as >1 positive blood cultures or >2 positive blood cultures if coagulase-negative Staphylococcus), ED visits (without hospitalization), and unplanned hospitalizations (excluding scheduled chemotherapy hospitalizations). We used χ2 analyses to compare the frequency of categorical outcomes, and we used unpaired t tests to assess differences in means of continuous variable in hematologic versus solid-tumor malignancy patients. We used generalized linear mixed-effects models to assess differences in BSI (clustered by patient) separately for gram-positive and gram-negative BSI outcomes. Results: Among 478 patients with 658 unique PICC lines and 64,190 line days, 271 patients (413 lines) had hematologic malignancy and 207 patients (232 lines) had solid-tumor malignancy. Cohort characteristics and outcomes stratified by malignancy type are shown in Table 1. Compared to those with hematologic malignancy, solid-tumor patients were older, had 47% fewer clinic visits, and had 32% lower frequency of prior PICC lines. Overall, there were 75 BSI events (12%; 1.2 per 1,000 catheter days). We detected no significant difference in BSI rates when comparing solid-tumor versus hematologic malignancies (P = 0.20); BSIs with gram-positive pathogen were 69% higher in patients with solid tumors. Gram-negative BSIs were 41% higher in patients with hematologic malignancy. Solid-tumor malignancy was associated with 4.5-fold higher odds of developing BSI with gram-positive pathogen (OR, 4.48; 95% CI, 1.60–12.60; P = .005) compared to those with hematologic malignancy, after adjusting for age, sex, history of prior PICC, and line duration. Differences in gram-negative BSI were not significant on multivariate analysis. Conclusions: The burden of all-cause BSIs in cancer clinic adults with PICC lines was 12% or 1.2 per 1,000 catheter days, as high as nationally reported inpatient BSI rates. Higher risk of gram-positive BSIs in solid-tumor patients suggests the need for targeted infection prevention activities in this population, such as improvements in central-line monitoring, outpatient care, and maintenance of lines and/or dressings, as well as chlorhexidine bathing to reduce skin bioburden.
Disclosures: None

Central-line team effort: Recognizing problematic central-line insertion sites in nursing homes
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s77-s78
-
- Article
-
- You have access
- Open access
- Export citation
-
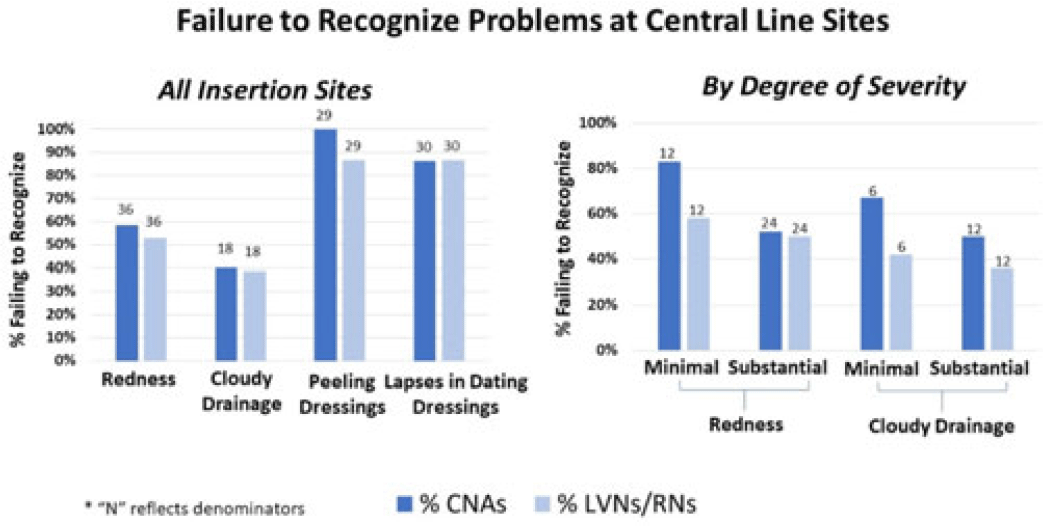
Background: Recognizing problematic central-line insertion sites is an important activity for CNAs, LVNs, and RNs in nursing homes (NHs). Although CNAs are not responsible for assessing central lines, they are often the first line of defense for noticing and relaying problems with a line because of the greater amount of time they spend with residents. We sought to assess how well CNAs, LVNs, and RNs could identify problematic insertion sites in NHs. Methods: We conducted a prospective observational study of central-line care in 8 NHs in Orange County, California. A convenience sample of central lines with a range of problematic elements was selected for quality improvement purposes. Research staff used standardized observation forms to evaluate presence of redness, cloudy drainage, and dressing integrity and change date. NH CNAs, LVNs, and RNs were asked to directly observe devices and to comment on problems or concerns. Participants were also asked open-ended questions about elements for a “picture-perfect line” and standard frequency of line checks and dressing changes. Failures to recognize existing problematic elements were tabulated for CNAs and LVNs or RNs separately. Results: In total, 50 CNAs (nursing home range, 3–6) and 50 LVNs and RNs (NH range, 4–6) directly observed lines with 131 problematic elements, including redness (N = 36), cloudy drainage (N = 30), peeling dressings (N = 29), and inappropriately dated dressing (N = 36). Failure to identify problematic elements involved redness [CNAs (50%) and LVNs or RNs (53%)], cloudy drainage [CNAs (40%) and LVNs or RNs (39%)], peeling dressings [CNAs (100%) and LVNs or RNs (87%)], and inappropriately dated dressing [CNAs (71%) and LVNs or RNs (68%)]. For both CNAs and LVNs and RNs, recognition of redness and cloudy drainage improved with severity. Failure to recognize minimal erythema [CNAs (83%) and LVNs or RNs (58%)] was higher than substantial erythema [CNAs (54%) and LVNs or RNs (50%)]. Similarly, failure to recognize minimal cloudy drainage [(CNAs (67%) and LVNs or RNs (50%)] was higher than substantial cloudy drainage [CNAs (42%) and LVNs or RNs (36%)]. Overall, identification of problematic elements did not vary by whether the staff member was assigned to care for that resident. Descriptions of “picture-perfect lines” were uniformly poor, with respondents not knowing what elements to mention. Conclusions: Failure to recognize redness, cloudy drainage, peeling dressings, and lapses in dressing change dates was common for CNAs and LVNs and RNs in nursing homes. This lack of recognition could prevent proper response to early and late signs of localized infection at central-line sites. Dedicated training regarding key elements of a “picture-perfect line” is needed, including changing the threshold for concern for both small and large amounts of redness and pus.
Disclosures: None

Assessing past versus present severe acute respiratory coronavirus virus 2 (SARS-CoV-2) infection: A survey of criteria for discontinuing precautions in asymptomatic patients testing positive on admission
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 13 September 2023, pp. 237-240
- Print publication:
- February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of measurement and feedback on chlorhexidine gluconate bathing among intensive care unit patients: A multicenter study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 13 September 2023, pp. 1375-1380
- Print publication:
- September 2023
-
- Article
- Export citation
Central-line team effort: Recognizing insertion-site concerns in nursing homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 04 August 2023, pp. 1887-1889
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Coronavirus disease 2019 (COVID-19) infection prevention practices that exceed Centers for Disease Control and Prevention (CDC) guidance: Balancing extra caution against impediments to care
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 01 June 2023, pp. 2074-2077
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of Alzheimer’s disease and related dementias (ADRD) on the quality of room cleaning in nursing homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1508-1510
- Print publication:
- September 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Epidemiology and genomics of a slow outbreak of methicillin-resistant Staphyloccus aureus (MRSA) in a neonatal intensive care unit: Successful chronic decolonization of MRSA-positive healthcare personnel
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 16 June 2022, pp. 589-596
- Print publication:
- April 2023
-
- Article
- Export citation
Finding a needle in a haystack: The hidden costs of asymptomatic testing in a low incidence setting
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 24 June 2021, pp. 1525-1526
- Print publication:
- October 2022
-
- Article
-
- You have access
- HTML
- Export citation
Coronavirus disease 2019 (COVID-19) research agenda for healthcare epidemiology
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 2 / February 2022
- Published online by Cambridge University Press:
- 25 January 2021, pp. 156-166
- Print publication:
- February 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Decreased Hospitalizations and Costs From Infection in Sixteen Nursing Homes in the SHIELD OC Regional Decolonization Initiative
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s7-s8
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Policies and practices of SHEA Research Network hospitals during the COVID-19 pandemic
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 10 / October 2020
- Published online by Cambridge University Press:
- 23 June 2020, pp. 1127-1135
- Print publication:
- October 2020
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of a Central-Line Insertion Site Assessment (CLISA) score on localized insertion site infection to prevent central-line–associated bloodstream infection (CLABSI)
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 1 / January 2020
- Published online by Cambridge University Press:
- 08 November 2019, pp. 59-66
- Print publication:
- January 2020
-
- Article
- Export citation
Reductions in Clostridium difficile Infection (CDI) Rates Using Real-Time Automated Clinical Criteria Verification to Enforce Appropriate Testing
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 39 / Issue 5 / May 2018
- Published online by Cambridge University Press:
- 19 March 2018, pp. 625-627
- Print publication:
- May 2018
-
- Article
- Export citation
