
166 results
4 Methamphetamine, cannabis, HIV, and their combined effects on neurocognition
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 797-798
-
- Article
-
- You have access
- Export citation
Cannabis use may attenuate neurocognitive performance deficits resulting from methamphetamine use disorder
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 30 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 09 August 2023, pp. 84-93
-
- Article
- Export citation
Emotional health and its association with neurocognition in Hispanic and non-Hispanic White people with HIV
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 30 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 20 April 2023, pp. 56-66
-
- Article
- Export citation
14 - In the Undergrowth: Llwyn a Pherth and Sexual Deviancy in Medieval Wales
-
-
- Book:
- Women's Literary Cultures in the Global Middle Ages
- Published by:
- Boydell & Brewer
- Published online:
- 09 January 2024
- Print publication:
- 04 April 2023, pp 261-276
-
- Chapter
- Export citation
Cannabis use and psychotic disorders in diverse settings in the Global South: findings from INTREPID II
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 23 March 2023, pp. 7062-7069
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Urbanicity and rates of untreated psychotic disorders in three diverse settings in the Global South
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 14 / October 2023
- Published online by Cambridge University Press:
- 16 January 2023, pp. 6459-6467
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Life events and psychosis: case–control study from India, Nigeria, and Trinidad and Tobago
-
- Journal:
- BJPsych Open / Volume 8 / Issue 5 / September 2022
- Published online by Cambridge University Press:
- 16 September 2022, e168
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association of antibiotics with veteran visit satisfaction and antibiotic expectations for upper respiratory tract infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 23 June 2022, e100
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
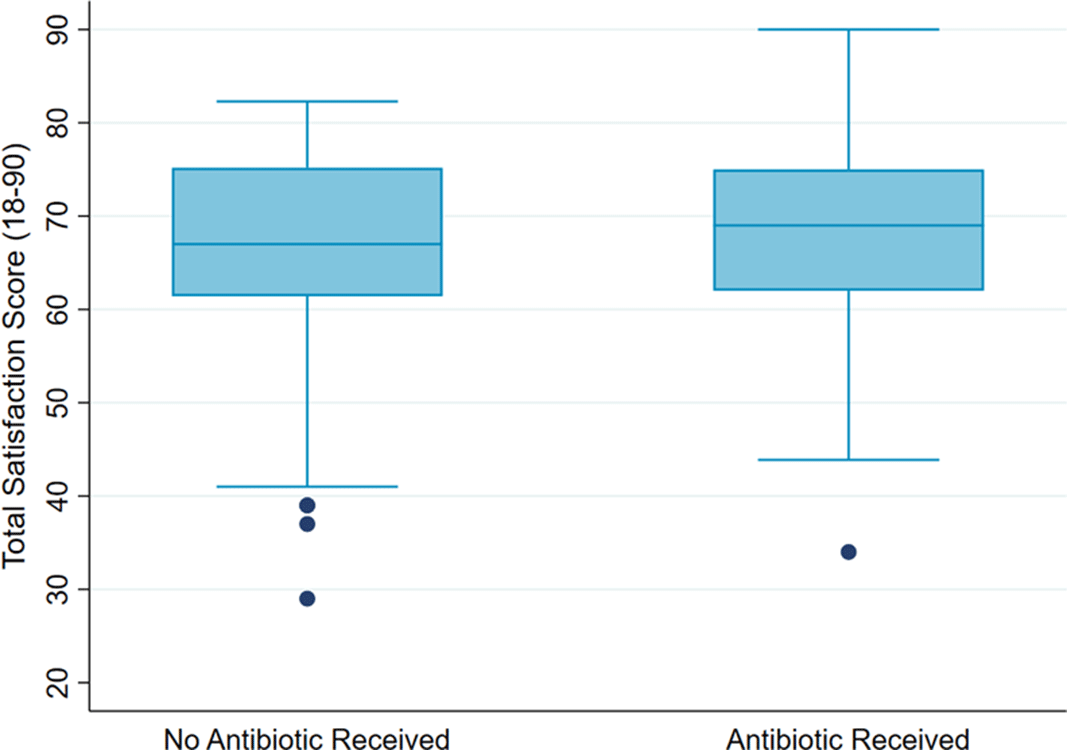
Veteran Satisfaction for Upper Respiratory-Tract Infection (URI) Visits Is Not Associated with Antibiotic Receipt But Is Associated with Antibiotic Expectation
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s33
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Antibiotics are not recommended but are often prescribed for upper respiratory-tract infections (URIs). Prescribers cite patient expectation as a driver of inappropriate antibiotic prescribing; prior literature has demonstrated higher satisfaction scores in patients who receive antibiotics compared to those who do not. We assessed whether veteran satisfaction at URI visits was associated with antibiotic receipt or with reported expectation for antibiotics. Methods: We surveyed veterans with documented URI encounters in the Veterans’ Affairs Tennessee Valley Healthcare System between January 1, 2018, and December 31, 2019. Patients not evaluated in person, with documented dementia, or who died prior to the study start date were excluded. Veterans were asked to recall their URI visit and to complete the Patient Safety Questionnaire (PSQ)-18 (Rand Corporation) and questions assessing antibiotic expectations. The PSQ-18, an 18-item survey that assesses patient satisfaction, uses a 5-point Likert scale (ie, strongly disagree, disagree, uncertain, agree, strongly agree), yielding a composite score of 18–90. Higher scores represent more satisfaction with care. Demographic and visit-specific information were extracted via chart review. We used multivariable linear regression to assess differences in composite PSQ-18 satisfaction scores between those who did and did not receive an antibiotic, adjusted for patient and visit characteristics, and to assess differences in satisfaction scores for those who did and did not report expecting antibiotics, adjusted for antibiotic receipt. Results: We identified 1,435 patients seen for URI at 17 sites. After exclusions, 1,343 veterans were eligible for chart abstraction. After excluding 42 responders who responded after study close or returned blank surveys, the final analytic cohort included 432 (32.2%) of 1,343 responders; 225 (52.1%) received an antibiotic and 207 (47.9%) did not. Mean total satisfaction for veterans who received an antibiotic was 67.8 (SD, ±9.4) compared to 66.7 (SD, ±9.7) for those who did not (Figure 1). Increased total satisfaction was not significantly associated with antibiotic receipt (0.65; 95% CI, −2.0 to 3.3). Most veterans (72.0%) disagreed that visit satisfaction depended on antibiotic receipt. However, only 30.8% reported that they would not expect an antibiotic for URI visits. A significant reduction in total satisfaction (−4.1; 95% CI, −6.3 to −1.9) was associated with expecting compared to not expecting an antibiotic. Conclusions: Our findings suggest that prescribing an antibiotic is not associated with increased veteran satisfaction for URI visits but is associated with expecting an antibiotic. Future work will evaluate methods to change veteran antibiotic expectations.
Funding: No
Disclosures: None
Figure 1.

Daily Cannabis Use is Associated With Lower CNS Inflammation in People With HIV
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 27 / Issue 6 / July 2021
- Published online by Cambridge University Press:
- 15 July 2021, pp. 661-672
-
- Article
- Export citation
Simulation and flow physics of a shocked and reshocked high-energy-density mixing layer
-
- Journal:
- Journal of Fluid Mechanics / Volume 915 / 25 May 2021
- Published online by Cambridge University Press:
- 22 March 2021, A84
-
- Article
- Export citation
Chapter 23 - Criminogenic Risk and Mental Health: A Complicated Relationship
- from Part IV - Nonpsychopharmacological Treatment Considerations
-
-
- Book:
- Decriminalizing Mental Illness
- Published online:
- 19 October 2021
- Print publication:
- 07 January 2021, pp 241-250
-
- Chapter
- Export citation
Chapter 22 - Examining Violence Among Not Guilty by Reason of Insanity State Hospital Inpatients Across Multiple Time Points: The Roles of Criminogenic Risk Factors and Psychiatric Symptoms
- from Part IV - Nonpsychopharmacological Treatment Considerations
-
-
- Book:
- Decriminalizing Mental Illness
- Published online:
- 19 October 2021
- Print publication:
- 07 January 2021, pp 231-240
-
- Chapter
- Export citation
The Qualitative Transparency Deliberations: Insights and Implications
-
- Journal:
- Perspectives on Politics / Volume 19 / Issue 1 / March 2021
- Published online by Cambridge University Press:
- 06 January 2021, pp. 171-208
- Print publication:
- March 2021
-
- Article
- Export citation
Placental adaptations in a nonhuman primate model of gestational protein restriction
-
- Journal:
- Journal of Developmental Origins of Health and Disease / Volume 12 / Issue 6 / December 2021
- Published online by Cambridge University Press:
- 14 December 2020, pp. 908-914
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Recreating the OSIRIS-REx slingshot manoeuvre from a network of ground-based sensors
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 37 / 2020
- Published online by Cambridge University Press:
- 27 November 2020, e049
-
- Article
-
- You have access
- HTML
- Export citation
A Guide for Caring for Patients Amidst the Novel Coronavirus Pandemic
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 15 / Issue 4 / August 2021
- Published online by Cambridge University Press:
- 13 October 2020, p. e19
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A theory limited in scope and evidence
-
- Journal:
- Behavioral and Brain Sciences / Volume 43 / 2020
- Published online by Cambridge University Press:
- 10 August 2020, e171
-
- Article
- Export citation
How do ethnicity and deprivation impact on life expectancy at birth in people with serious mental illness? Observational study in the UK
-
- Journal:
- Psychological Medicine / Volume 51 / Issue 15 / November 2021
- Published online by Cambridge University Press:
- 06 May 2020, pp. 2581-2589
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
23 - Implications of the Changing Nature of Work for Employee Health and Safety
- from Part III - Implications for Talent Management and Impact on Employees
-
-
- Book:
- The Cambridge Handbook of the Changing Nature of Work
- Published online:
- 02 April 2020
- Print publication:
- 23 April 2020, pp 489-508
-
- Chapter
- Export citation
