
21 results
The effectiveness of COVID-19 vaccine in the prevention of post-COVID conditions: a systematic literature review and meta-analysis of the latest research
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 13 October 2023, e168
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The effectiveness of coronavirus disease 2019 (COVID-19) vaccine in the prevention of post–COVID-19 conditions: A systematic literature review and meta-analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 06 December 2022, e192
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Coronavirus disease 2019 (COVID-19) among nonphysician healthcare personnel by work location at a tertiary-care center, Iowa, 2020–2021
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 02 June 2022, pp. 1351-1354
- Print publication:
- August 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The long-term effectiveness of coronavirus disease 2019 (COVID-19) vaccines: A systematic literature review and meta-analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 14 February 2022, e22
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The short-term effectiveness of coronavirus disease 2019 (COVID-19) vaccines among healthcare workers: a systematic literature review and meta-analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 21 October 2021, e33
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Bat intrusions at a tertiary care center in Iowa, 2018–2020
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 16 August 2021, pp. 1948-1950
- Print publication:
- December 2022
-
- Article
- Export citation
Molecular Epidemiology of Large COVID-19 Clusters at an Academic Medical Center, March–October 2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s10-s11
-
- Article
-
- You have access
- Open access
- Export citation
-
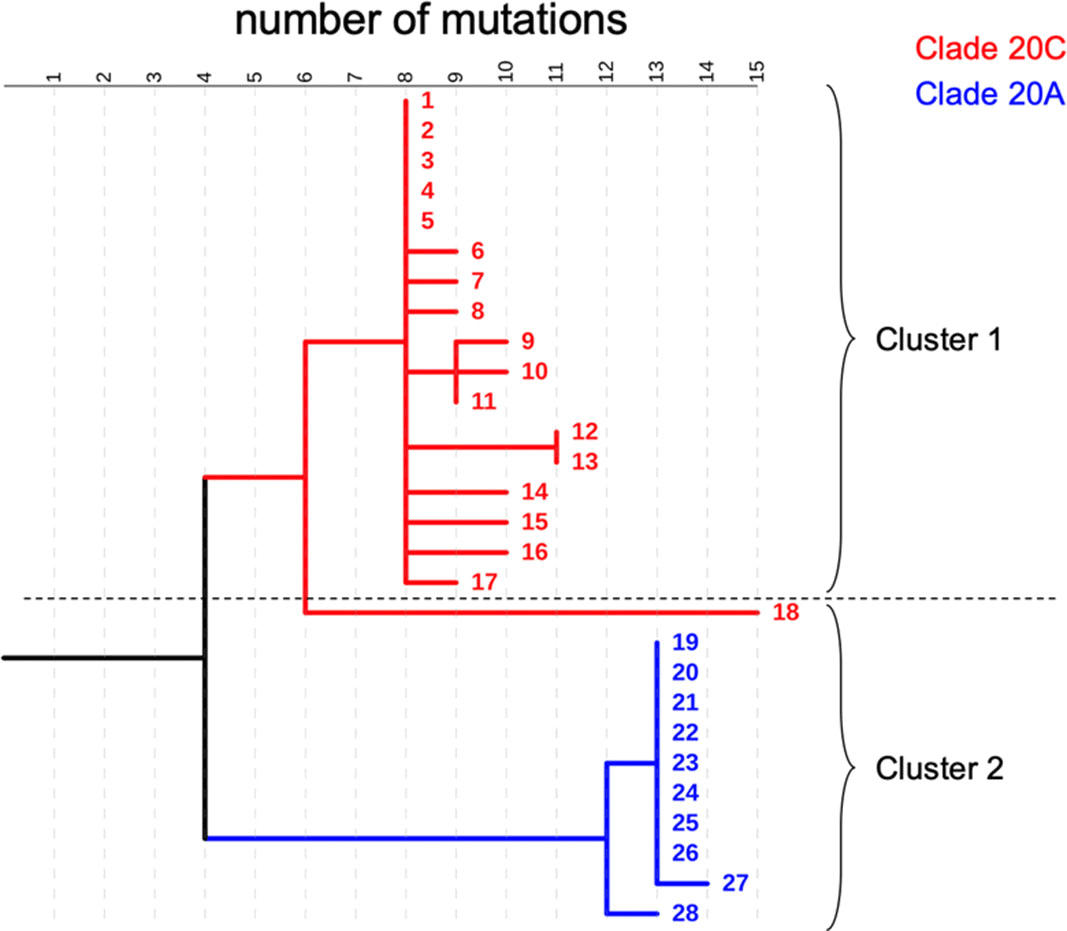
Background: COVID-19 in hospitalized patients may be the result of community acquisition or in-hospital transmission. Molecular epidemiology can help confirm hospital COVID-19 transmission and outbreaks. We describe large COVID-19 clusters identified in our hospital and apply molecular epidemiology to confirm outbreaks. Methods: The University of Iowa Hospitals and Clinics is an 811-bed academic medical center. We identified large clusters involving patients with hospital onset COVID-19 detected during March–October 2020. Large clusters included ≥10 individuals (patients, visitors, or HCWs) with a laboratory confirmed COVID-19 diagnosis (RT-PCR) and an epidemiologic link. Epidemiologic links were defined as hospitalization, work, or visiting in the same unit during the incubation or infectious period for the index case. Hospital onset was defined as a COVID-19 diagnosis ≥14 days from admission date. Admission screening has been conducted since May 2020 and serial testing (every 5 days) since July 2020. Nasopharyngeal swab specimens were retrieved for viral whole-genome sequencing (WGS). Cluster patients with a pairwise difference in ≤5 mutations were considered part of an outbreak. WGS was performed using Oxford Nanopore Technology and protocols from the ARTIC network. Results: We identified 2 large clusters involving patients with hospital-onset COVID-19. Cluster 1: 2 hospital-onset cases were identified in a medical-surgical unit in June 2020. Source and contact tracing revealed 4 additional patients, 1 visitor, and 13 employees with COVID-19. Median age for patients was 62 (range, 38–79), and all were male. In total, 17 samples (6 patients, 1 visitor, and 10 HCWs) were available for WGS. Cluster 2: A hospital-onset case was identified via serial testing in a non–COVID-19 intensive care unit in September 2020. Source investigation, contact tracing, and serial testing revealed 3 additional patients, and 8 HCWs. One HCW also had a community exposure. Patient median age was 60 years (range, 48–68) and all were male. In total, 11 samples (4 patients and 7 HCWs) were sequenced. Using WGS, cluster 1 was confirmed to be an outbreak: WGS showed 0–5 mutations in between samples. Cluster 2 was also an outbreak: WGS showed less diversity (0–3 mutations) and ruled out the HCW with a community exposure (20 mutations of difference). Conclusion: Whole-genome sequencing confirmed the outbreaks identified using classic epidemiologic methods. Serial testing allowed for early outbreak detection. Early outbreak detection and implementation of control measures may decrease outbreak size and genetic diversity.
Funding: No
Disclosures: None
Figure 1.

Bat Intrusions at a Tertiary Care Center, Iowa 2018–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s16
-
- Article
-
- You have access
- Open access
- Export citation
-
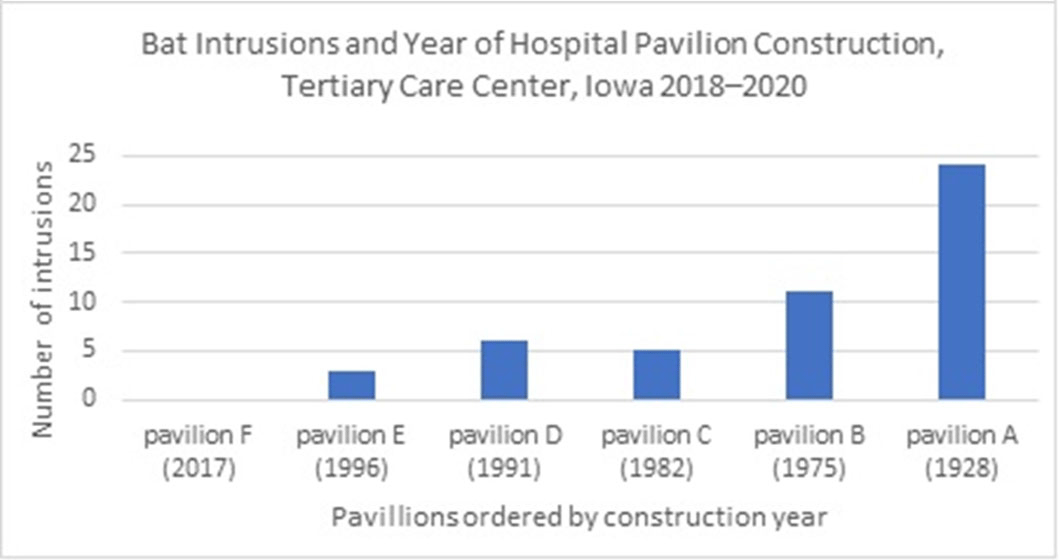
Background: Bats are recognized as important vectors in disease transmission. Frequently, bats intrude into homes and buildings, increasing the risk to human health. We describe bat intrusions and exposure incidents in our hospital over a 3-year period. Methods: The University of Iowa Hospitals and Clinics (UIHC) is an 811-bed academic medical center in Iowa City, Iowa. Established in 1928, UIHC currently covers 209,031.84 m2 (~2,250,000 ft2) and contains 6 pavilions built between 1928 and 2017. We retrospectively obtained bat intrusion calls from the infection prevention and control program call database at UIHC during 2018–2020. We have also described the event management for intrusions potentially associated with patient exposures. Results: In total, 67 bat intrusions occurred during 2018–2020. The most frequent locations were hallways or lounges 28 (42%), nonclinical office spaces 19 (14%), and stairwells 8 (12%). Most bat intrusions (65%) occurred during the summer and fall (June–November). The number of events were 15 in 2018, 28 in 2019, and 24 in 2020. We observed that the number of intrusions increased with the age of each pavilion (Figure 1). Of 67 intrusions, 2 incidents (3%) were associated with potential exposure to patients. In the first incident, reported in 2019, the bat was captured in a patient care area and released before an investigation of exposures was completed and no rabies testing was available. Also, 10 patients were identified as having had potential exposure to the bat. Among them, 9 patients (90%) received rabies postexposure prophylaxis. In response to this serious event, we provided facility-wide education on our bat control policy, which includes the capture and safe handling of the bat, assessment of potential exposures, and potential need for rabies testing. We also implemented a bat exclusion project focused on the exterior of the oldest hospital buildings. The second event, 1 patient was identified to have potential exposure to the bat. The bat was captured, tested negative for rabies, no further action was needed. Conclusions: Bat intrusions can be an infection prevention and control challenge in facilities with older buildings. Hospitals may need animal intrusion surveillance systems, management protocols, and remediation efforts.
Funding: No
Disclosures: None
Figure 1.

COVID-19 Conversion after Exposure in a Semiprivate Room at a Tertiary Care Center in Iowa, July–December 2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s20-s21
-
- Article
-
- You have access
- Open access
- Export citation
Coronavirus Disease 2019 (COVID-19) Admission Screening at a Tertiary-Care Center, Iowa 2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s1
-
- Article
-
- You have access
- Open access
- Export citation
Suspected COVID-19 Reinfections at a Tertiary Care Center, Iowa 2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s19
-
- Article
-
- You have access
- Open access
- Export citation
Impact of COVID-19 on Volume of Infection Prevention and Control Calls at a Tertiary-Care Center in Iowa, 2018–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s53-s54
-
- Article
-
- You have access
- Open access
- Export citation
-
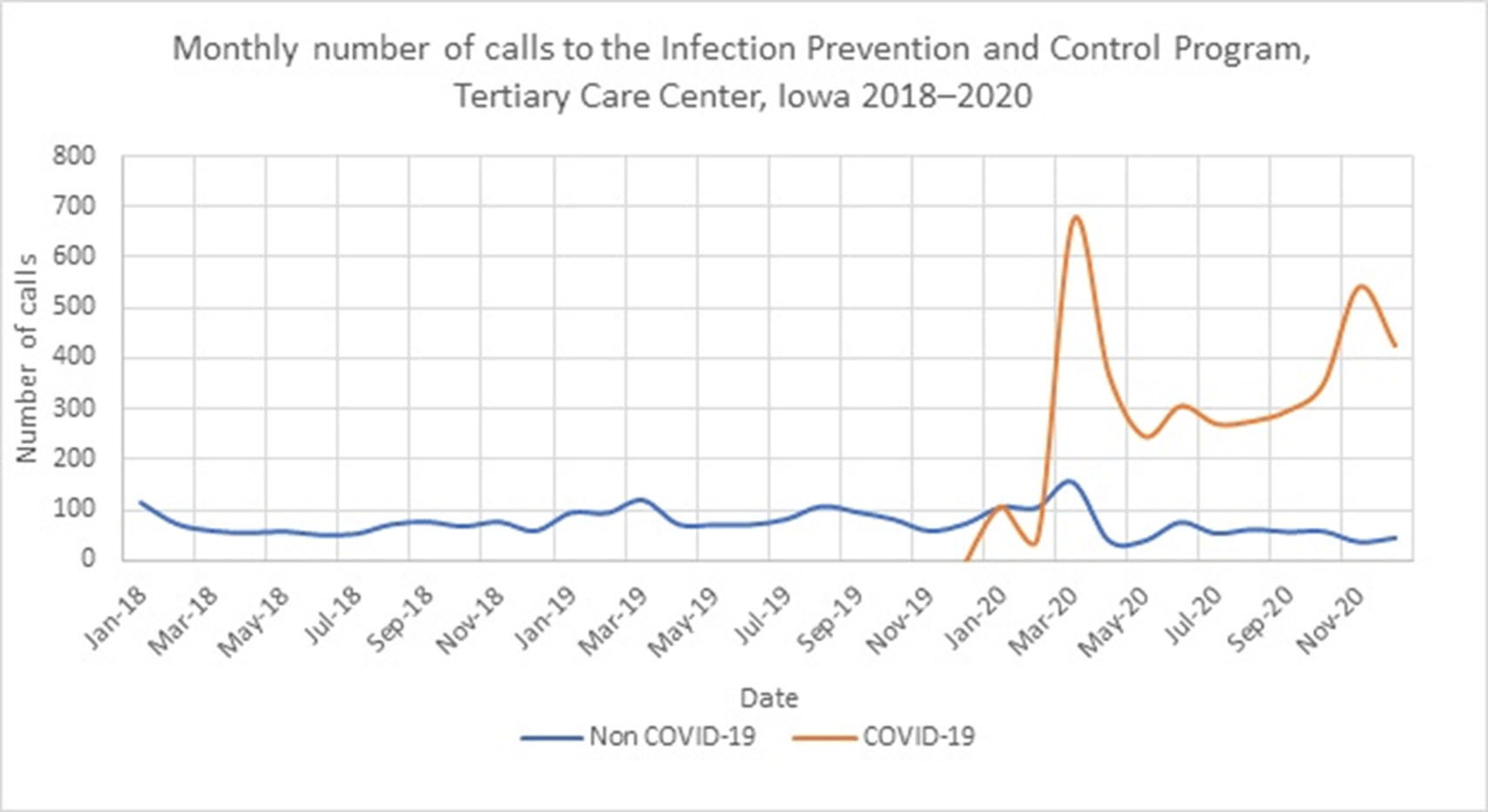
Background: The COVID-19 pandemic has affected healthcare systems worldwide, but the impact on infection prevention and control (IPC) programs has not been fully evaluated. We assessed the impact of the COVID-19 pandemic on IPC consultation requests. Methods: The University of Iowa Hospitals & Clinics comprises an 811-bed hospital that admits >36,000 patients yearly and >200 outpatient clinics. Questions about IPC can be addressed to the Program of Hospital Epidemiology via e-mail, in person, or through our phone line. We routinely record date and time, call source, reason for the call, and estimated time to resolve questions for all phone line requests. We defined calls during 2018–2019 as the pre–COVID-19 period and calls from January to December 2020 as the COVID-19 period. Results: In total, 6,564 calls were recorded from 2018 to 2020. In the pre–COVID-19 period (2018–2019), we received a median of 71 calls per month (range, 50–119). The most frequent call sources were inpatient units (n = 902; 50%), department of public health (n = 357; 20%), laboratory (n = 171; 9%), and outpatient clinics (n = 120; 7%) (Figure 1). The most common call topics were isolation and precautions (n = 606; 42%), outside institutions requests (n = 324; 22%), environmental and construction (n = 148; 10%), and infection exposures (n = 149; 10%). The most frequent infection-related calls were about tuberculosis (17%), gram-negative organisms (14%), and influenza (9%). During the COVID-19 period, the median monthly call volume increased 500% to 368 per month (range, 149–829). Most (83%) were COVID-19 related. The median monthly number of COVID-19 calls was 302 (range, 45–674). The median monthly number of non–COVID-19 calls decreased to 56 (range, 36–155). The most frequent call sources were inpatient units (57%), outpatient clinics (16%), and the department of public health (5%). Most calls concerned isolation and precautions (50%) and COVID-19 testing (20%). The mean time required to respond to each question was 10 minutes (range, 2–720). The biggest surges in calls during the COVID-19 period were at the beginning of the pandemic (March 2020) and during the hospital peak COVID-19 census (November 2020). Conclusions: In addition to supporting a proactive COVID-19 response, our IPC program experienced a 500% increase in consultation requests. Planning for future bioemergencies should include creative strategies to provide additional resources to increase response capacity within IPC programs.
Funding: No
Disclosures: None
Figure 1.

Coronavirus disease 2019 (COVID-19) incidence after exposures in shared patient rooms in a tertiary-care center in Iowa, July 2020–May 2021
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 12 July 2021, pp. 1910-1913
- Print publication:
- December 2022
-
- Article
- Export citation
Coronavirus disease 2019 (COVID-19) admission screening and assessment of infectiousness at an academic medical center in Iowa, 2020
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 8 / August 2022
- Published online by Cambridge University Press:
- 24 June 2021, pp. 974-978
- Print publication:
- August 2022
-
- Article
- Export citation
Molecular epidemiology of large coronavirus disease 2019 (COVID-19) clusters before and after the implementation of routine serial testing at an academic medical center in Iowa, 2020
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 12 / December 2021
- Published online by Cambridge University Press:
- 24 June 2021, pp. 1514-1516
- Print publication:
- December 2021
-
- Article
- Export citation
Positive deviance in infection prevention and control: A systematic literature review
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 3 / March 2022
- Published online by Cambridge University Press:
- 11 November 2020, pp. 358-365
- Print publication:
- March 2022
-
- Article
- Export citation
Risk Factors and Mortality in Pediatric Patients with Stenotrophomonas maltophilia Bacteremia
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s374-s375
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Administrative Coding Methods Impact Surgical Site Infection Rates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s111-s112
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Tuberculosis Exposure and Conversion Rates Can Guide Deimplementation of Annual Tuberculosis Screening
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s419
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Administrative coding methods impact surgical site infection rates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 12 / December 2020
- Published online by Cambridge University Press:
- 10 August 2020, pp. 1461-1463
- Print publication:
- December 2020
-
- Article
- Export citation
