
34 results
Improving shared decision-making around antimicrobial-prescribing during the end-of-life period: a qualitative study of Veterans, their support caregivers and their providers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 17 May 2024, e89
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Research agenda for transmission prevention within the Veterans Health Administration, 2024–2028
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 11 April 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Spatiotemporal distribution of community-acquired phenotypic extended-spectrum beta-lactamase Escherichia coli in United States counties, 2010–2019
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 4 / April 2024
- Published online by Cambridge University Press:
- 11 December 2023, pp. 540-542
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Persistence of potential ST398 MSSA in outpatient settings among US veterans, 2010–2019
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 20 October 2023, e177
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Diagnostic accuracy of antibiograms in predicting the risk of antimicrobial resistance for individual patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s42-s43
-
- Article
-
- You have access
- Open access
- Export citation
-
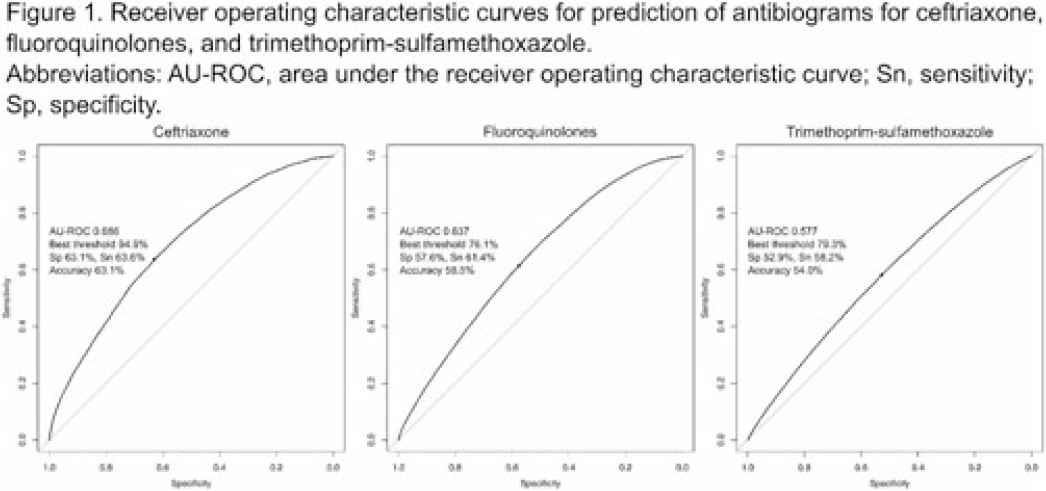
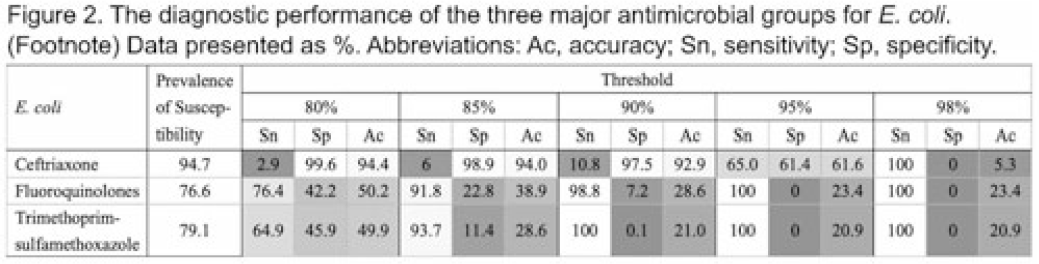
Background: Many clinical guidelines recommend that clinicians should use antibiograms to decide on empiric antimicrobial therapy. However, antibiograms aggregate epidemiologic data without consideration for any other factors that may affect the risk of antimicrobial resistance (AMR), and little is known about an antibiogram’s reliability in predicting antimicrobial susceptibility. We assessed the diagnostic accuracy of antibiograms as a prediction tool for E. coli clinical isolates in predicting the risk of AMR for individual patients. Methods: We extracted microbiologic and patient-level data from the nationwide clinical data warehouse of the Veterans Health Administration (VHA). We assessed the diagnostic accuracy of the antibiogram for 3 commonly used antimicrobial classes for E. coli: ceftriaxone, fluoroquinolones, and trimethoprim-sulfamethoxazole. First, we retrospectively generated facility-level antibiograms for all VHA facilities from 2000 to 2019 using all clinical culture specimens positive for E. coli, according to the latest Clinical & Laboratory Standards Institute guideline. Second, we created a patient-level data set by including only patients who did not have a positive culture for E. coli in the preceding 12 months. Then we assessed the diagnostic accuracy of an antibiogram for E. coli to predict resistance for the isolates in the following calendar year, using logistic regression models with percentages in the antibiogram as dependent variables. We also set 5 stepwise thresholds at 80%, 85%, 90%, 95%, and 98%, and we calculated sensitivity, specificity, and accuracy for each antimicrobial. Results: Among 127 VHA hospitals, 1,484,038 isolates from 704,779 patients were available for analysis. The area under the ROC curve (AU-ROC) was 0.686 for ceftriaxone, 0.637 for fluoroquinolones, and 0.578 for trimethoprim-sulfamethoxazole, suggesting their relatively poor prediction performances (Fig. 1). The sensitivity and specificity of the antibiogram widely varied by antimicrobial groups and thresholds, with substantial trade-offs. Along with AU-ROC, these metrics suggest poor prediction performances when antibiograms are used as the sole prediction tool (Fig. 2). Conclusions: Antibiograms for E. coli have poor performances in predicting the risk of AMR for individual patients when they are used as a sole tool, and their contribution to the clinical decision making may be limited. Clinicians should also consider other clinical and epidemiologic data when interpreting antibiograms, and guideline statements that suggest antibiogram as a valuable tool for decision making in empiric therapy may need to be reconsidered. Further studies are needed to evaluate the contribution of antibiograms when combined with other patient-level factors.
Disclosures: None


Perceptions of an automated benchmarking dashboard for antimicrobial stewardship programs among antimicrobial stewards within the veterans’ health administration: a multicenter qualitative study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 10 July 2023, e118
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impacts of Hurricane Matthew Exposure on Infections and Antimicrobial Prescribing in North Carolina Veterans
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 20 March 2023, e357
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Tracking antimicrobial stewardship activities beyond days of therapy (DOT): Comparison of days of antibiotic spectrum coverage (DASC) and DOT at a single center
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 10 January 2023, pp. 934-937
- Print publication:
- June 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
County-level spatiotemporal distribution of fluoroquinolone-resistant Enterobacteriaceae in outpatient settings of the Veterans’ Health Administration, 2000–2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 02 December 2022, pp. 1497-1499
- Print publication:
- September 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Is the number of prescriptions an appropriate metric for outpatient antimicrobial consumption? A comparison between the prescription counts and days supplied
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 23 August 2022, pp. 941-944
- Print publication:
- June 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Investigation of factors influencing inpatient antibiotic prescribing decisions in the Veterans’ Health Administration
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 23 June 2022, e99
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antibiotic use in end-of-life care patients: A nationwide Veterans’ Health Administration cohort study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s19-s20
-
- Article
-
- You have access
- Open access
- Export citation
-
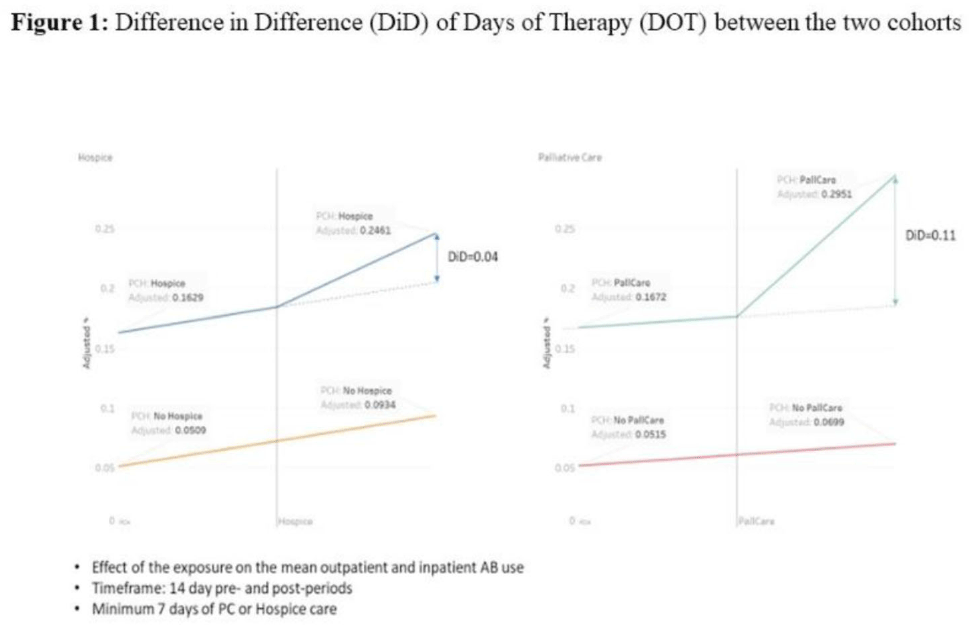
Background: Antibiotic use during end-of-life (EOL) care is an increasingly important target for antimicrobial stewardship given the high prevalence of antibiotic use in this setting with limited evidence on safety and effectiveness to guide antibiotic decision making. We estimated antibiotic use during the last 6 months of life for patients under hospice or palliative care, and we identified potential targets (ie time points) during the EOL period when antimicrobial stewardship interventions could be targeted for maximal benefit. Methods: We conducted a retrospective cohort study of nationwide Veterans’ Affairs (VA) patients, 18 years and older who died between January 1, 2014, and December 31, 2019, and who had been hospitalized within 6 months prior to death. Data from the VA’s integrated electronic medical record (EMR) were collected including demographics, comorbid conditions, and duration of inpatient antibiotics administered, along with outpatient antibiotics dispensed. A propensity-score matched-cohort analysis was conducted to compare antibiotic use between patients placed into palliative care or hospice matched to patients not receiving palliative care or hospice care. Repeated measures ANOVA and repeated measures linear regression methods were used to analyze difference in difference (D-I-D) of days of therapy (DOT) between the 2 cohorts. Results: There were 251,822 patients in the cohort, including 23,746 in hospice care, 89,768 in palliative care, and 138,308 without palliative or hospice care. The median days from last discharge to death was 9 days. The most common comorbidities were chronic obstructive pulmonary diseases (50%), malignancy (46%), and diabetes mellitus (43%). Overall, 18,296 (77%) of 23,746 hospice patients, and 71,812 (80%) of 89,768 palliative care patients received at least 1 antibiotic, whereas 95,167 (69%) of 138,308 who were not placed in hospice or did not receive palliative care received antibiotics. In the primary matched cohort analysis that compared patients placed into hospice or palliative care to propensity-score matched controls, entry into palliative care was associated with a 11% absolute increase in antibiotic prescribing, and entry into hospice was associated with a 4% absolute increase during the 7–14 days after entry versus the 7–14 days before entry (Fig. 1). The stratified cohorts had very similar balanced covariates as the overall cohort. Conclusions: In our large cohort study, we observed that patients receiving EOL care had high levels of antibiotic exposure across VA population, particularly on entry to hospice or during admissions when they received palliative care consultation. Future studies are needed to identify the optimal EOL strategies for collaboration between antimicrobial stewardship and palliative care.
Funding: None
Disclosures: None

Qualitative Evaluation of an automated nationwide benchmarking antimicrobial utilization dashboard for the VHA
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s4
-
- Article
-
- You have access
- Open access
- Export citation
-
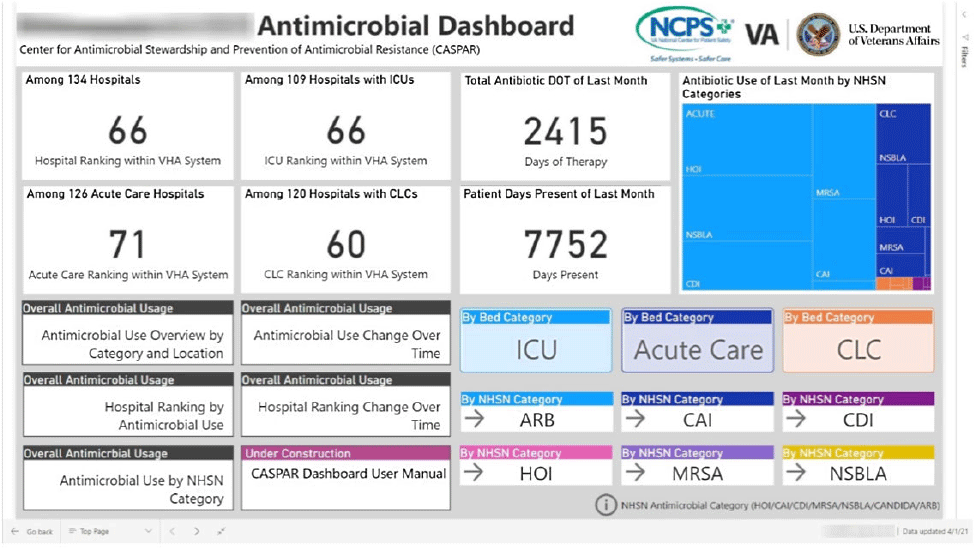
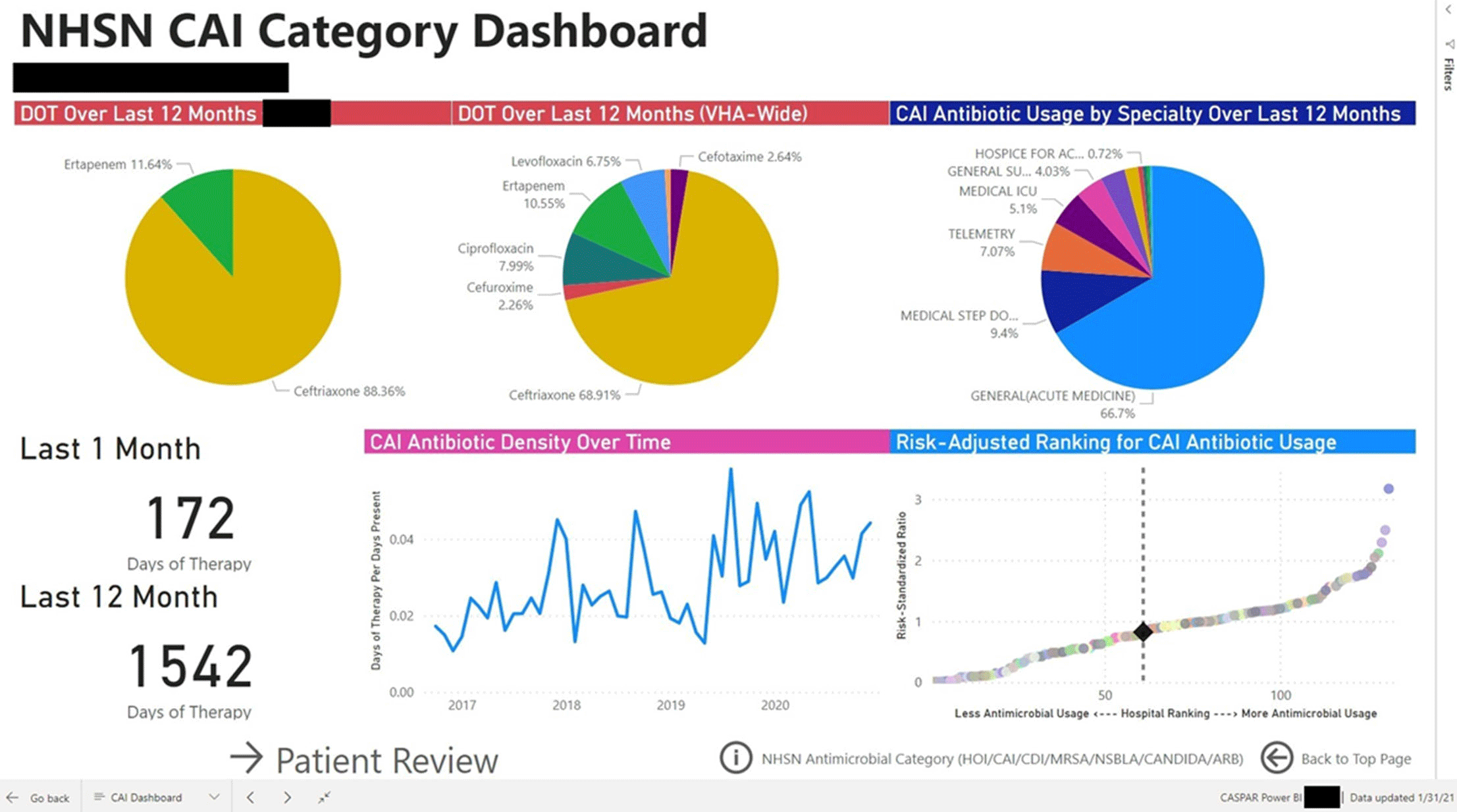
Background: Antimicrobial stewardship programs (ASPs) are advised to audit antimicrobial consumption as a metric to feedback to clinicians. However, many ASPs lack the tools necessary for appropriate risk adjustment and standardized data collection, which are critical for peer-program benchmarking. We evaluated the impact of the dashboard deployment that displays these metrics and its acceptance among ASP members and antimicrobial prescribers. Materials/methods: We conducted semistructured interviews of ASP stewards and antimicrobial prescribers before and after implementation of a web-based ASP information dashboard (Fig. 1) implemented in the VA Midwest Health Care Network (VISN23). The dashboard provides risk-adjusted benchmarking, longitudinal trends, and analysis of antimicrobial usage patterns at each facility. Risk-adjusted benchmarking was based on an observed-to-expected comparison of antimicrobial days of therapy at each facility, after adjusting for differences in patient case mix and facility-level variables. Respondents were asked to evaluate several aspects of the dashboard, including its ease of use, applicability to ongoing ASP activities, perceived validity and reliability, and advantages compared to other ASP monitoring systems. All interviews were digitally recorded and transcribed verbatim. The analysis was conducted using MaxQDA 2020.4 and the Consolidated Framework for Implementation Research (CFIR) constructs. Results: We completed 4 preimplementation interviews and 11 postimplementation interviews with ASP champions and antimicrobial prescribers from 6 medical centers. We derived 4 key themes from the data that map onto CFIR constructs. These themes were interconnected so that implementation of the dashboard (ie, adapting and adopting) was influenced by respondents’ perception of a facility’s size, patient population, and priority placed on stewardship (ie, structural and cultural context), the availability of dedicated stewardship staff and training needed to implement the dashboard (ie, resources needed), and how the dashboard compared to established stewardship activities (ie, relative advantage). ASP champions and antimicrobial prescribers indicated that dashboard metrics were useful for identifying antimicrobial usage and for comparing metrics among similar facilities. Respondents also specified barriers to acceptance of the risk-adjusted metric, such as disagreement regarding how antimicrobials were grouped by the current NHSN protocol, uncertainty of factors involved in risk adjustments, and difficulty developing a clear interpretation of hospital rankings. Conclusions: Given the limited resources for antimicrobial stewardship personnel, automated, risk-adjusted, antimicrobial-use dashboards provided by ASPs are an attractive method to both facilitate compliance and improve efficiency. To increase the uptake of surveillance systems in antimicrobial stewardship, our study highlights the need for clear descriptions of methods and metrics.
Funding: None
Disclosures: None

Hospital-level variation in the utilization of antipseudomonal antibiotics: A nationwide cross-sectional study at the VHA
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s21
-
- Article
-
- You have access
- Open access
- Export citation
-
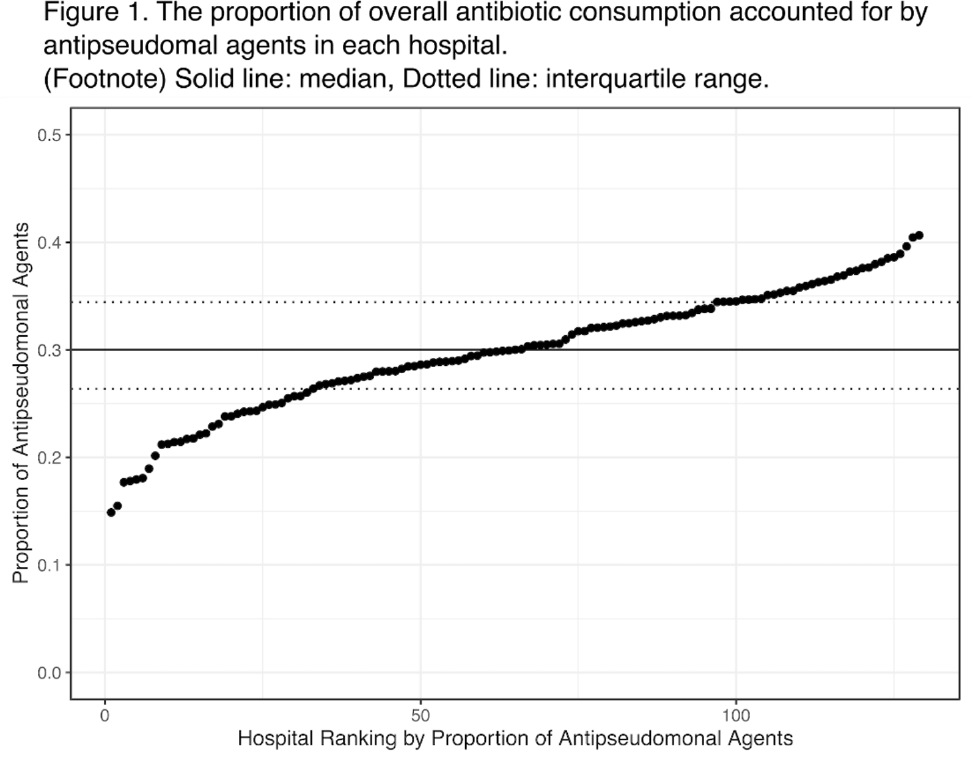
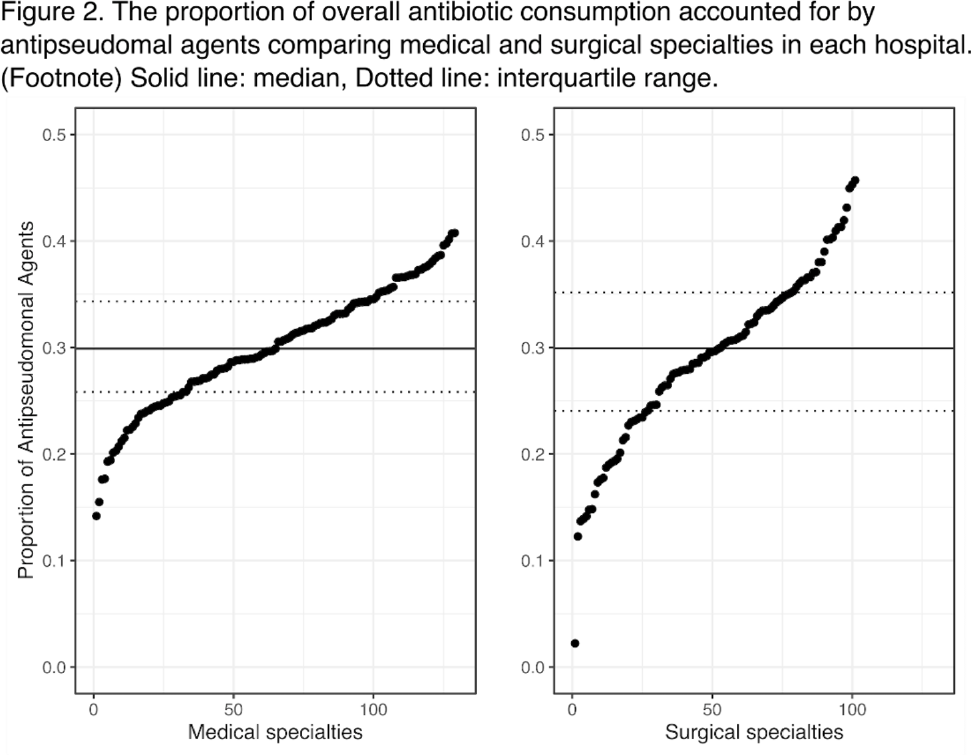
Background: Avoiding unnecessary antipseudomonal coverage is 1 of the most common targets for antibiotic stewardship programs (ASPs), but little is known about the magnitude of facility-level variation in antipseudomonal agent utilization. We aimed to describe the variability in the use of antipseudomonal agents across inpatient settings within a nationwide integrated healthcare system. Method: We analyzed the data from a retrospective cohort of patients who were admitted to acute-care hospitals within the VHA system in 2019. We defined antipseudomonal agents as systemic antibiotics with activity against wild-type Pseudomonas aeruginosa, and we evaluated overall and antipseudomonal antibiotic use among 129 hospitals, according to the agents described in the NHSN Antimicrobial Usage and Resistance Module. We calculated each hospital’s overall and antipseudomonal days of therapy (DOT) per 1,000 days present and the proportion of antipseudomonal agent usage among all antibiotics based on DOT at each hospital. Hospital-level variation was assessed by comparing the proportion of total antibiotic consumption accounted for by antipseudomonal agents. Associations between antipseudomonal proportions and overall antibiotic consumption were also assessed. Results: Among 129 VHA hospitals, the median DOT per 1,000 days present for all antibiotics was 434.4 (IQR, 371.9–487.1), and the median antipseudomonal DOT per 1,000 days present was 127.7 (IQR, 99.8–159.6). The median proportion of total antibiotic consumption accounted for by antipseudomonal agents was 30.0% (range, 14.9%–40.7%; IQR, 26.4%–34.4%) (Fig. 1). We detected only a weak correlation between overall antibiotic consumption and antipseudomonal proportion (Pearson correlation coefficient, 0.396), which suggests that hospitals with higher total antibiotic consumption were not necessarily using more antipseudomonal agents. In a stratified analysis, there was more prominent hospital-level variability in surgical specialties than medical specialties (Fig. 2). Conclusions: We detected high hospital-level variability in the consumption and proportion of antipseudomonal antibiotics among an integrated healthcare system. Although it is plausible that these variabilities originated from case-mix differences among hospitals, including differing rates of P. aeruginosa infections, it may also highlight opportunities for reducing antipseudomonal antibiotic utilization, especially among surgical specialties. Further studies are needed to evaluate the contribution of modifiable patient- and facility-level factors to this variability.
Funding: None
Disclosures: None


Reduction in outpatient antibiotic utilization: An unintended benefit of the COVID-19 pandemic?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s64
-
- Article
-
- You have access
- Open access
- Export citation
-
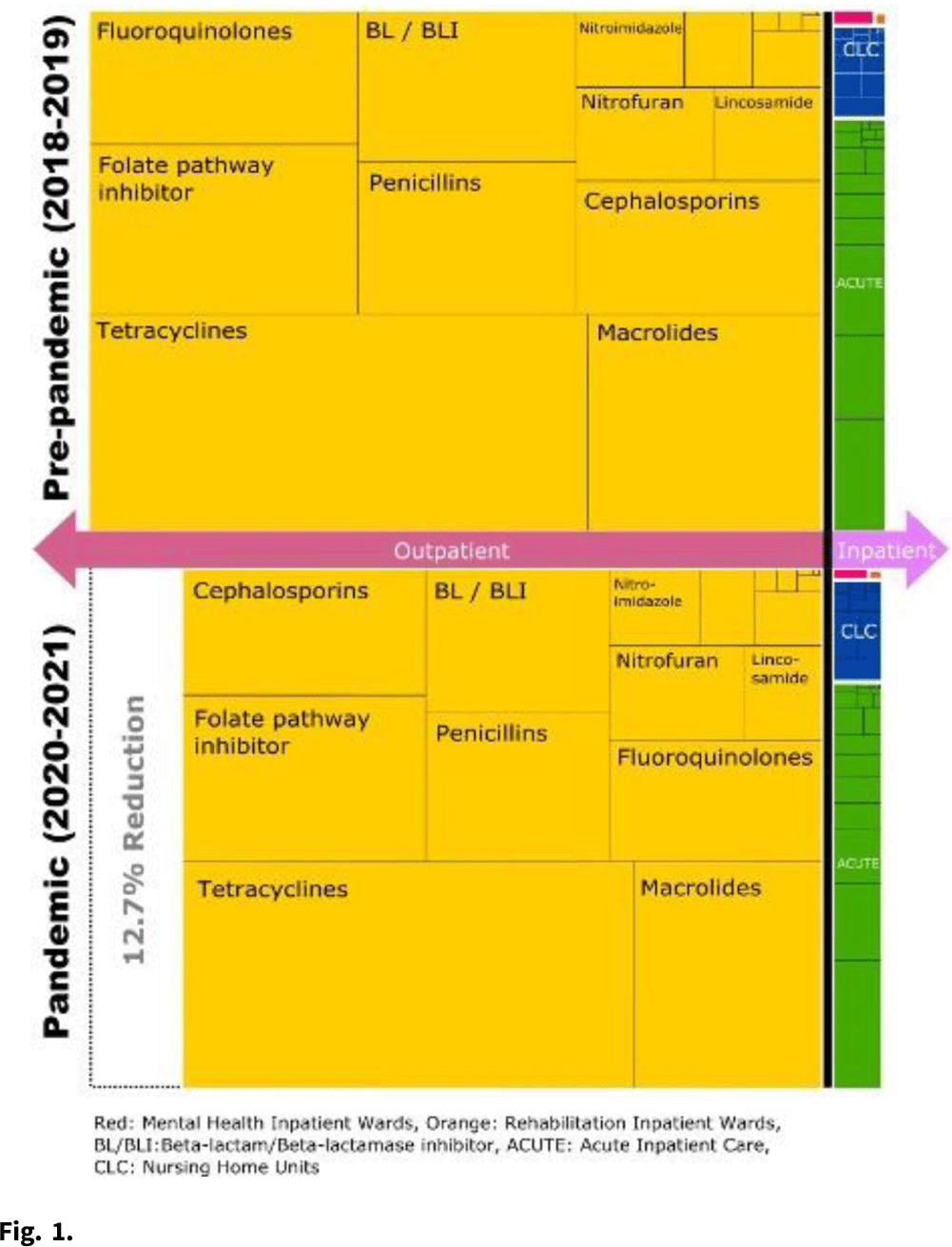
Background: The COVID-19 pandemic heavily affected healthcare delivery systems in the United States. However, little is known about its impact on overall antimicrobial consumption, especially in outpatient settings. We assessed the impact of the COVID-19 pandemic on antimicrobial consumption in both outpatient and inpatient (acute-care, long-term care, and mental health) settings in the Veterans’ Health Administration (VHA) during the 2 years before and after the start of the pandemic. Methods: We conducted a retrospective study for all patients who received care within the VHA from January 2018 to December 2021. We used antibiotic days as the primary outcome measure (days of therapy for inpatient settings and dispensed days supply for outpatient settings), and we obtained data for antimicrobial consumption from the VHA Corporate Data Warehouse. Antibiotics were categorized into classes by the NHSN protocol and included only systemic agents (oral and parenteral). We defined 2018–2019 as the prepandemic period and 2020–2021 as the pandemic period. We compared the relative and absolute difference in antibiotic consumption between the 2 periods. Results: Across all periods, 8.3 million patients received care in the VHA, and an average of 28,709,680 antibiotic days were prescribed per year. Overall, 92.9% of all antibiotic days were outpatient and 7.1% were inpatient. Total antibiotic days during the pandemic period decreased by 12.4% compared to the prepandemic period (pandemic period: 53,613,840 and prepandemic period: 61,224,878). This reduction was primarily driven by reductions in outpatient settings (relative reduction: 12.7% and absolute reduction: 7,254,880 antibiotic days over 2 years), but antibiotic days in inpatient settings decreased more modestly (relative reduction: 8.4% and absolute reduction: 356,158 antibiotic days over 2 years) (Fig. 1). When frequently prescribed antimicrobials were categorized by classes, fluoroquinolones and lincosamides showed the largest decreases (fluoroquinolones: 29.2% reduction and lincosamides: 27.2% reduction). Tetracyclines and sulfamethoxazole–trimethoprim had the smallest reductions (5.2% and 11.2%, respectively). Conclusions: Compared to the prepandemic period, the pandemic was associated with a substantial reduction in overall antibiotic consumption, especially in outpatient settings, which accounted for 95% of the overall reduction despite being outside the domain of most traditional antibiotic stewardship programs. The impact of the pandemic was most modest in the use of tetracyclines and trimethoprim–sulfamethoxazole and was most prominent in the use of fluoroquinolones and lincosamides. Further studies are required to improve the causal inference between the COVID-19 pandemic and this reduction in antibiotic consumption, as well as its impact on patient outcomes.
Funding: None
Disclosures: None

Decline in oral antimicrobial prescription in the outpatient setting after nationwide implementation of financial incentives and provider education: An interrupted time-series analysis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 06 April 2022, pp. 253-259
- Print publication:
- February 2023
-
- Article
- Export citation
Delays and declines in seasonal influenza vaccinations due to Hurricane Harvey narrow annual gaps in vaccination by race, income and rurality
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 16 March 2022, pp. 1833-1839
- Print publication:
- December 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Outpatient antibiotic prescribing for common infections via telemedicine versus face-to-face visits: Systematic literature review and meta-analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 31 August 2021, e24
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Automated Nationwide Benchmarking Dashboard for Antimicrobial Stewardship Programs within the Veterans’ Health Administration
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s23-s24
-
- Article
-
- You have access
- Open access
- Export citation
-
Group Name: VHA Center for Antimicrobial Stewardship and Prevention of Antimicrobial Resistance (CASPAR) Background: Antimicrobial stewardship programs (ASPs) are advised to measure antimicrobial consumption as a metric for audit and feedback. However, most ASPs lack the tools necessary for appropriate risk adjustment and standardized data collection, which are critical for peer-program benchmarking. We created a system that automatically extracts antimicrobial use data and patient-level factors for risk-adjustment and a dashboard to present risk-adjusted benchmarking metrics for ASP within the Veterans’ Health Administration (VHA). Methods: We built a system to extract patient-level data for antimicrobial use, procedures, demographics, and comorbidities for acute inpatient and long-term care units at all VHA hospitals utilizing the VHA’s Corporate Data Warehouse (CDW). We built baseline negative binomial regression models to perform risk-adjustments based on patient- and unit-level factors using records dated between October 2016 and September 2018. These models were then leveraged both retrospectively and prospectively to calculate observed-to-expected ratios of antimicrobial use for each hospital and for specific units within each hospital. Data transformation and applications of risk-adjustment models were automatically performed within the CDW database server, followed by monthly scheduled data transfer from the CDW to the Microsoft Power BI server for interactive data visualization. Frontline antimicrobial stewards at 10 VHA hospitals participated in the project as pilot users. Results: Separate baseline risk-adjustment models to predict days of therapy (DOT) for all antibacterial agents were created for acute-care and long-term care units based on 15,941,972 patient days and 3,011,788 DOT between October 2016 and September 2018 at 134 VHA hospitals. Risk adjustment models include month, unit types (eg, intensive care unit [ICU] vs non-ICU for acute care), specialty, age, gender, comorbidities (50 and 30 factors for acute care and long-term care, respectively), and preceding procedures (45 and 24 procedures for acute care and long-term care, respectively). We created additional models for each antimicrobial category based on National Healthcare Safety Network definitions. For each hospital, risk-adjusted benchmarking metrics and a monthly ranking within the VHA system were visualized and presented to end users through the dashboard (an example screenshot in Figure 1). Conclusions: Developing an automated surveillance system for antimicrobial consumption and risk-adjustment benchmarking using an electronic medical record data warehouse is feasible and can potentially provide valuable tools for ASPs, especially at hospitals with no or limited local informatics expertise. Future efforts will evaluate the effectiveness of dashboards in these settings.
Funding: No
Disclosures: None
Figure 1.
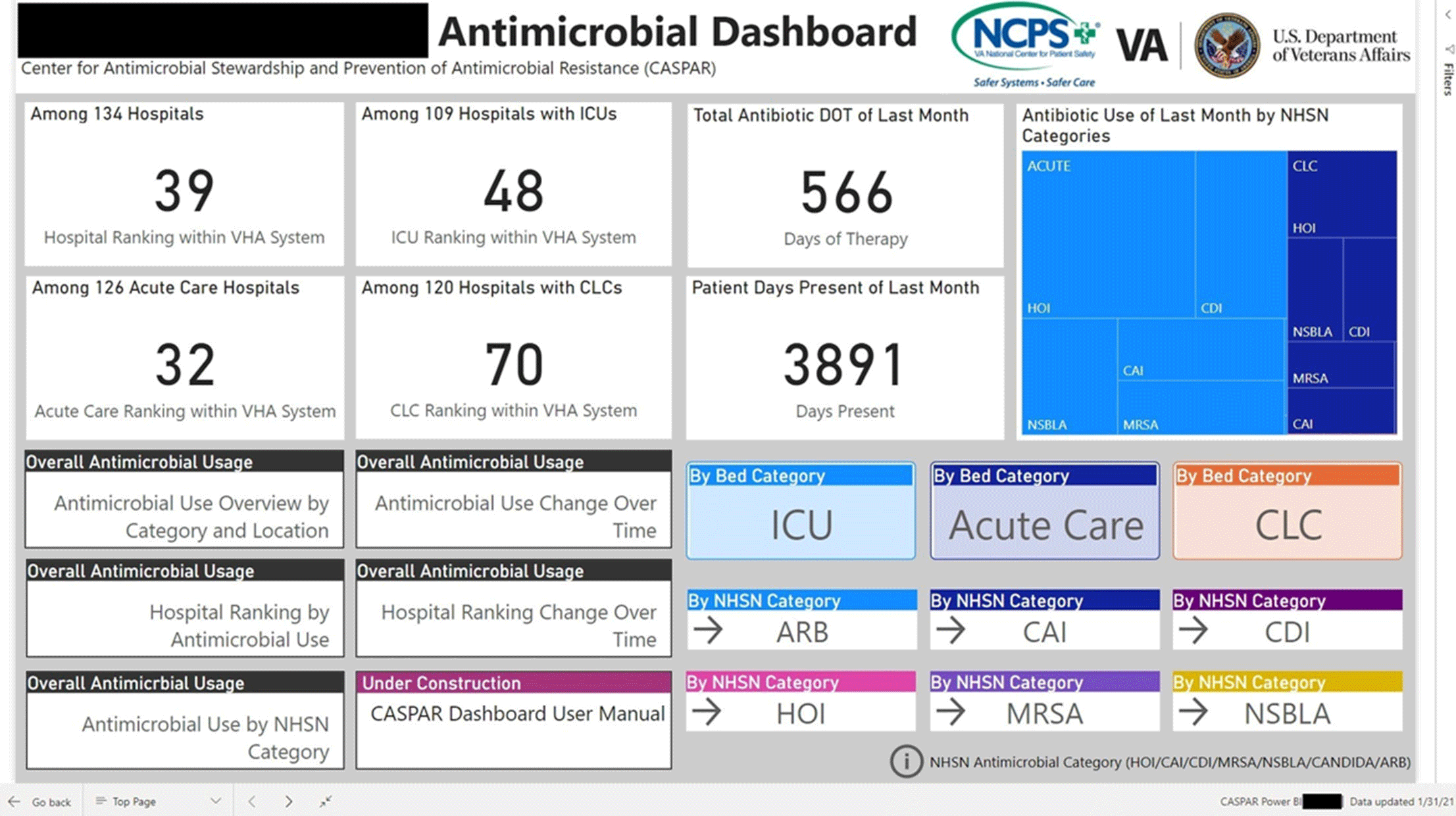
Figure 2.
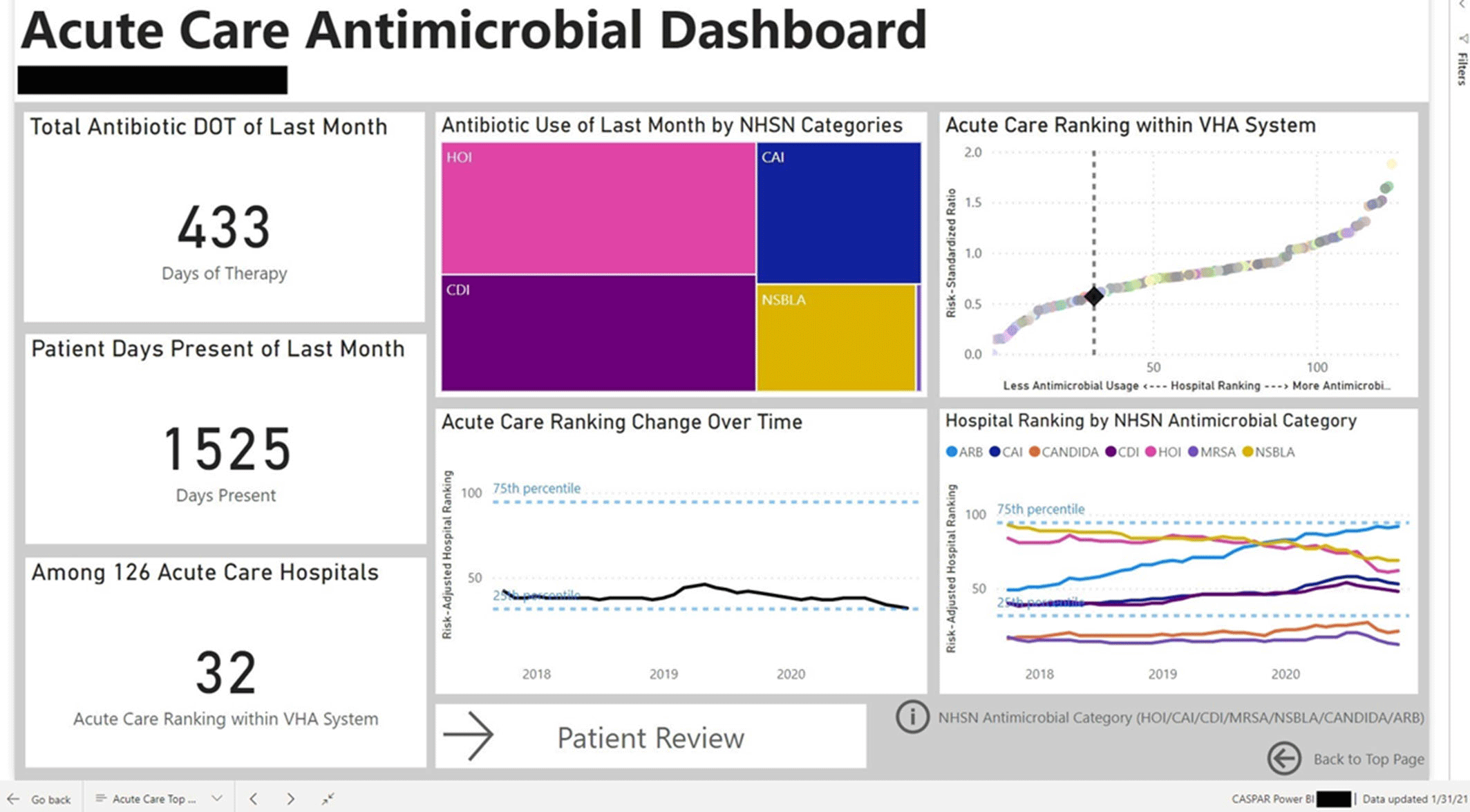
Figure 3.



Development of a fully automated surgical site infection detection algorithm for use in cardiac and orthopedic surgery research
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 10 / October 2021
- Published online by Cambridge University Press:
- 23 February 2021, pp. 1215-1220
- Print publication:
- October 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
