
505 results
Assessing harmonized intelligence measures in a multinational study
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 11 / 2024
- Published online by Cambridge University Press:
- 23 February 2024, e22
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Psychometric Properties of the Mini International Neuropsychiatric Interview (MINI) Psychosis Module: A Sub-Saharan Africa Cross Country Comparison – CORRIGENDUM
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 2 / January 2024
- Published online by Cambridge University Press:
- 10 January 2024, p. 436
-
- Article
-
- You have access
- HTML
- Export citation
Understanding Ludwig Lachmann's Economics
-
- Published online:
- 25 December 2023
- Print publication:
- 01 February 2024
-
- Element
- Export citation
6 Association Between American Football Play and Parkinson's Disease: Analysis of the Fox Insight Data Set
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 415-416
-
- Article
-
- You have access
- Export citation
64 Neuroimaging Evidence of Neurodegenerative Disease in Former Professional American Football Players Who “Fail” Validity Testing: A Case Series
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 574-575
-
- Article
-
- You have access
- Export citation
Childhood trauma moderates schizotypy-related brain morphology: analyses of 1182 healthy individuals from the ENIGMA schizotypy working group
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 6 / April 2024
- Published online by Cambridge University Press:
- 20 October 2023, pp. 1215-1227
-
- Article
- Export citation
On a multi-parameter variant of the Bellow–Furstenberg problem
- Part of
-
- Journal:
- Forum of Mathematics, Pi / Volume 11 / 2023
- Published online by Cambridge University Press:
- 19 September 2023, e23
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We prove convergence in norm and pointwise almost everywhere on
 $L^p$,
$L^p$,  $p\in (1,\infty )$, for certain multi-parameter polynomial ergodic averages by establishing the corresponding multi-parameter maximal and oscillation inequalities. Our result, in particular, gives an affirmative answer to a multi-parameter variant of the Bellow–Furstenberg problem. This paper is also the first systematic treatment of multi-parameter oscillation semi-norms which allows an efficient handling of multi-parameter pointwise convergence problems with arithmetic features. The methods of proof of our main result develop estimates for multi-parameter exponential sums, as well as introduce new ideas from the so-called multi-parameter circle method in the context of the geometry of backwards Newton diagrams that are dictated by the shape of the polynomials defining our ergodic averages.
$p\in (1,\infty )$, for certain multi-parameter polynomial ergodic averages by establishing the corresponding multi-parameter maximal and oscillation inequalities. Our result, in particular, gives an affirmative answer to a multi-parameter variant of the Bellow–Furstenberg problem. This paper is also the first systematic treatment of multi-parameter oscillation semi-norms which allows an efficient handling of multi-parameter pointwise convergence problems with arithmetic features. The methods of proof of our main result develop estimates for multi-parameter exponential sums, as well as introduce new ideas from the so-called multi-parameter circle method in the context of the geometry of backwards Newton diagrams that are dictated by the shape of the polynomials defining our ergodic averages.


Patterns, predictors, and patient-reported reasons for antidepressant discontinuation in the WHO World Mental Health Surveys
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 14 September 2023, pp. 67-78
-
- Article
- Export citation
Prospective association of attachment style with suicide attempts among US Army soldiers
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 4 / March 2024
- Published online by Cambridge University Press:
- 31 August 2023, pp. 785-793
-
- Article
- Export citation
The use of a Subjective wellbeing scale as predictor of adherence to neuroleptic treatment to determine poor prognostic factor in African population with Schizophrenia
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S156
-
- Article
-
- You have access
- Open access
- Export citation
Psychometric Properties of the Mini International Neuropsychiatric Interview (MINI) Psychosis Module: A Sub-Saharan Africa Cross Country Comparison
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 10 March 2023, pp. 7042-7052
-
- Article
- Export citation
A practical risk calculator for suicidal behavior among transitioning U.S. Army soldiers: results from the Study to Assess Risk and Resilience in Servicemembers-Longitudinal Study (STARRS-LS)
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 09 March 2023, pp. 7096-7105
-
- Article
- Export citation
Mega-analysis of association between obesity and cortical morphology in bipolar disorders: ENIGMA study in 2832 participants
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 14 / October 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 6743-6753
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prospective associations of emotion reactivity and risk behaviors with suicide attempts in US Army soldiers
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 13 / October 2023
- Published online by Cambridge University Press:
- 04 November 2022, pp. 6124-6131
-
- Article
- Export citation
The thalamus and its subregions – a gateway to obsessive-compulsive disorder
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S77-S78
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Higher thalamic volume has been found in children with obsessive-compulsive disorder (OCD) and children with clinical-level symptoms within the general population (Boedhoe et al. 2017, Weeland et al. 2021a). Functionally distinct thalamic nuclei are an integral part of OCD-relevant brain circuitry.
ObjectivesWe aimed to study the thalamic nuclei volume in relation to subclinical and clinical OCD across different age ranges. Understanding the role of thalamic nuclei and their associated circuits in pediatric OCD could lead towards treatment strategies specifically targeting these circuits.
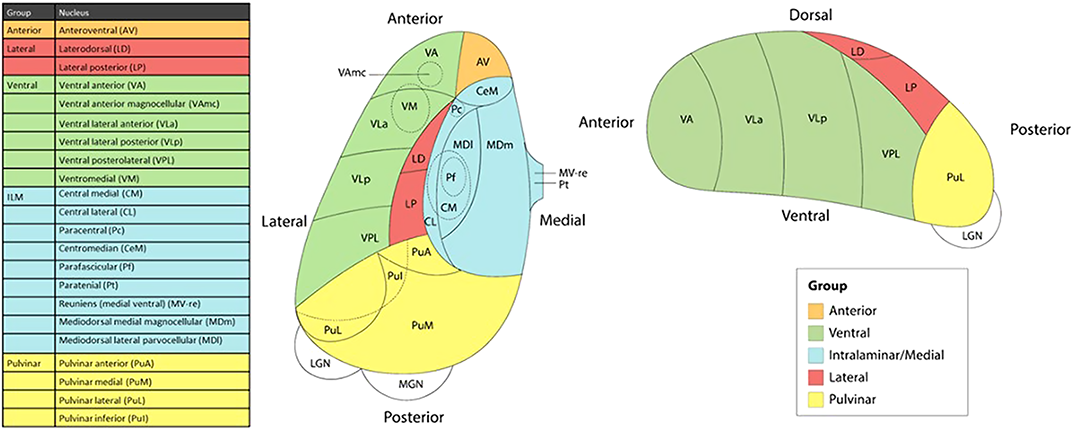
MethodsWe studied the relationship between thalamic nuclei and obsessive-compulsive symptoms (OCS) in a large sample of school-aged children from the Generation R Study (N = 2500) (Weeland et al. 2021b). Using the data from the ENIGMA-OCD working group we conducted mega-analyses to study thalamic subregional volume in OCD across the lifespan in 2,649 OCD patients and 2,774 healthy controls across 29 sites (Weeland et al. 2021c). Thalamic nuclei were grouped into five subregions: anterior, ventral, intralaminar/medial, lateral and pulvinar (Figure 1).
 Results
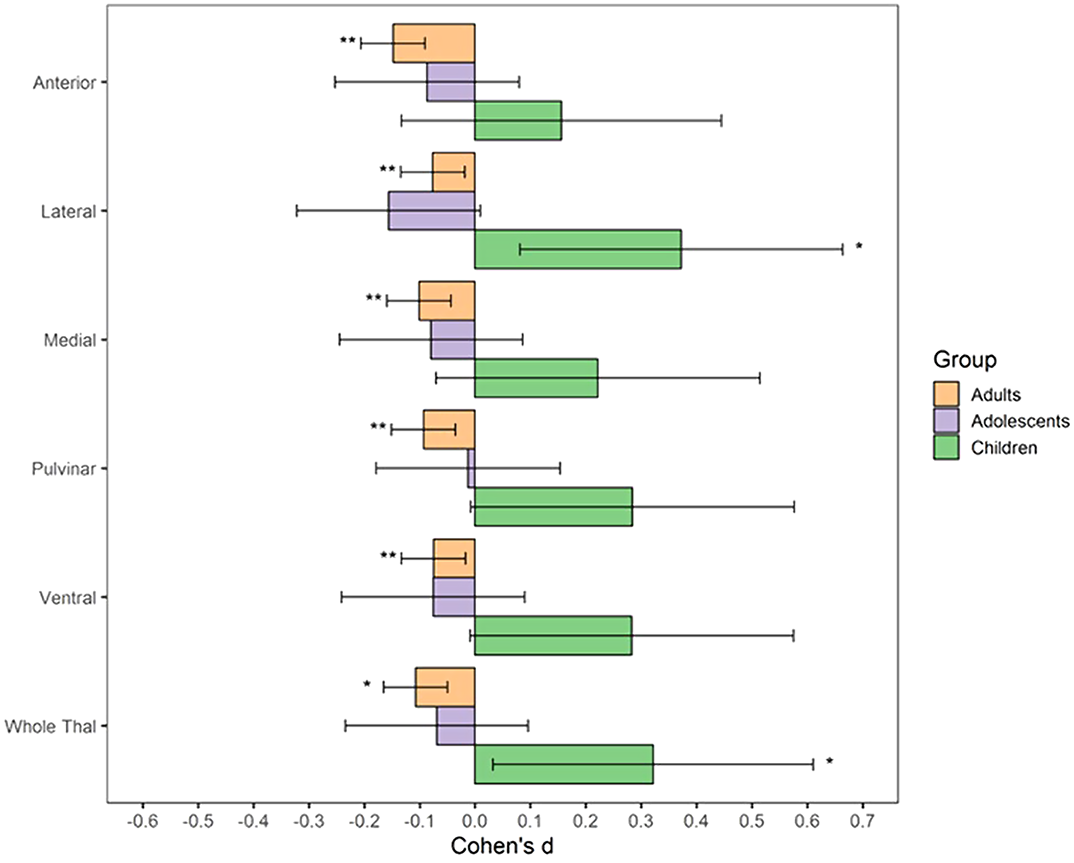
ResultsBoth children with subclinical and clinical OCD compared with controls show increased volume across multiple thalamic subregions. Adult OCD patients have decreased volume across all subregions (Figure 2), which was mostly driven by medicated and adult-onset patients.
 Conclusions
ConclusionsOur results suggests that OCD-related thalamic volume differences are global and not driven by particular subregions and that the direction of effects are driven by both age and medication status.
DisclosureNo significant relationships.


Mental Health in Individuals with a History of Mental Disorder during COVID-19-Pandemic - Preliminary Results of the National Cohort Study in Germany
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S376-S377
-
- Article
-
- You have access
- Open access
- Export citation
Associations of vulnerability to stressful life events with suicide attempts after active duty among high-risk soldiers: results from the Study to Assess Risk and Resilience in Servicemembers-longitudinal study (STARRS-LS)
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 9 / July 2023
- Published online by Cambridge University Press:
- 27 May 2022, pp. 4181-4191
-
- Article
- Export citation
Risk of bacterial bloodstream infection does not vary by central-line type during neutropenic periods in pediatric acute myeloid leukemia
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 25 April 2022, pp. 222-229
- Print publication:
- February 2023
-
- Article
- Export citation
Eight-year trajectories of behavior problems and resilience in children exposed to early-life intimate partner violence: The overlapping and distinct effects of individual factors, maternal characteristics, and early intervention
-
- Journal:
- Development and Psychopathology / Volume 35 / Issue 2 / May 2023
- Published online by Cambridge University Press:
- 14 March 2022, pp. 850-862
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Unsparing self-critique strengthens the field, but Bailey et al. overstate the ‘problems with delay discounting’
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 4 / March 2023
- Published online by Cambridge University Press:
- 28 February 2022, pp. 1658-1659
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
