
285 results
A Comparison of Variable Input Strategies used for Risk-adjustment Models of Antimicrobial Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s30-s31
-
- Article
-
- You have access
- Open access
- Export citation
-
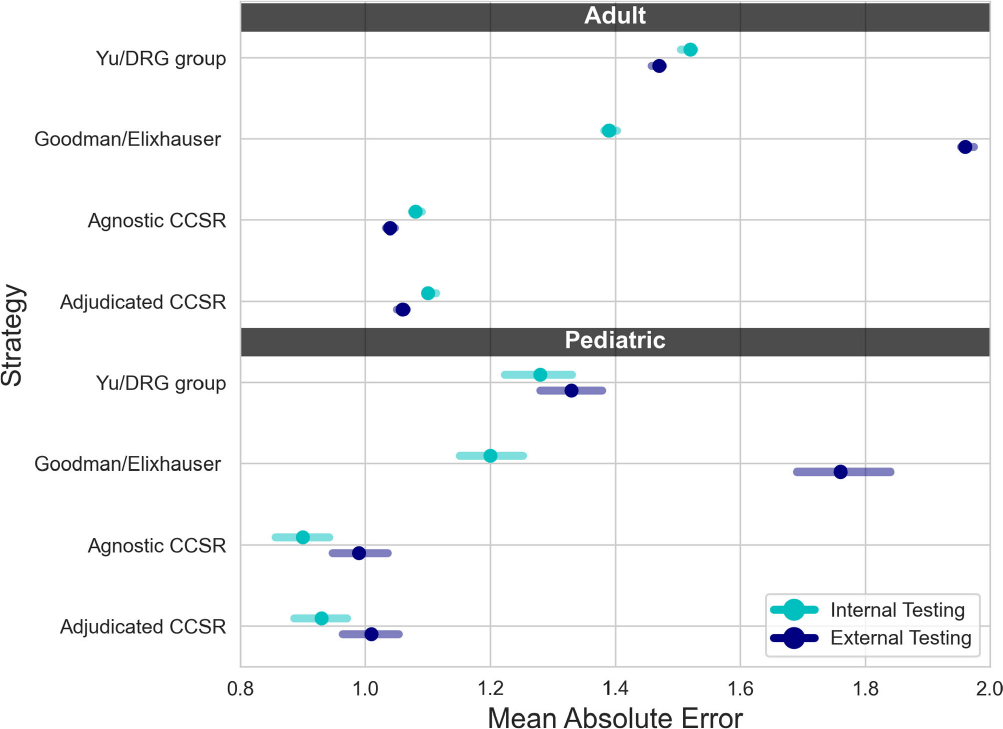
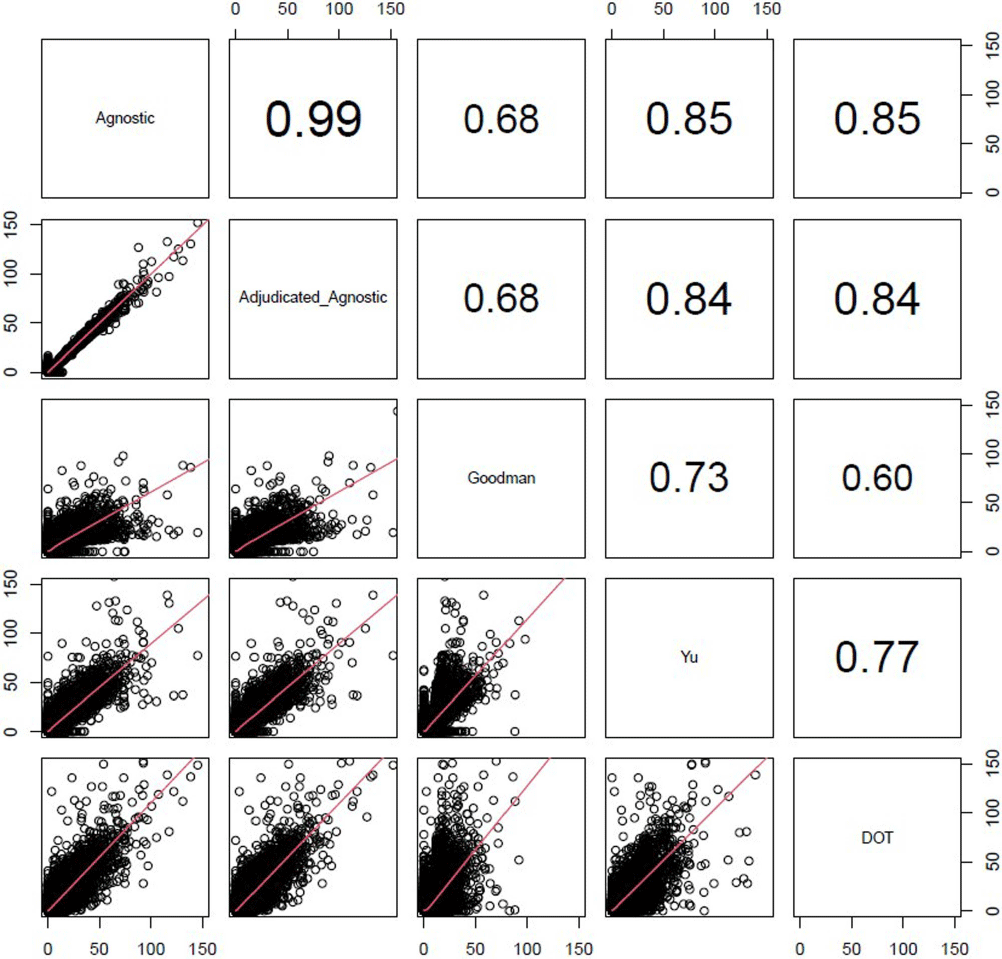
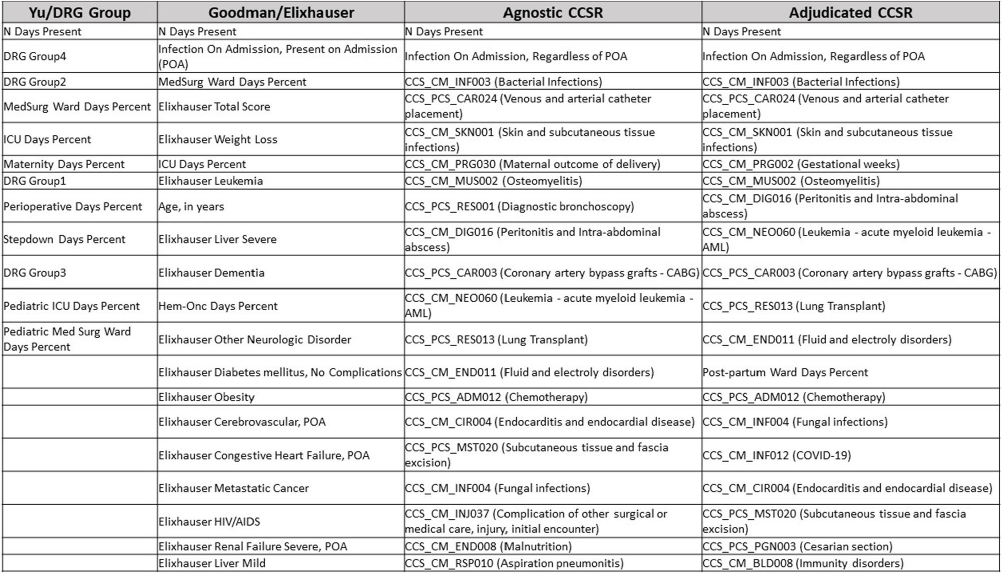
Background: External comparisons of antimicrobial use (AU) may be more informative if adjusted for encounter characteristics. Optimal methods to define input variables for encounter-level risk-adjustment models of AU are not established. Methods: This retrospective analysis of electronic health record data included 50 US hospitals in 2020-2021. We used NHSN definitions for all antibacterials days of therapy (DOT), including adult and pediatric encounters with at least 1 day present in inpatient locations. We assessed 4 methods to define input variables: 1) diagnosis-related group (DRG) categories by Yu et al., 2) adjudicated Elixhauser comorbidity categories by Goodman et al., 3) all Clinical Classification Software Refined (CCSR) diagnosis and procedure categories, and 4) adjudicated CCSR categories where codes not appropriate for AU risk-adjustment were excluded by expert consensus, requiring review of 867 codes over 4 months to attain consensus. Data were split randomly, stratified by bed size as follows: 1) training dataset including two-thirds of encounters among two-thirds of hospitals; 2) internal testing set including one-third of encounters within training hospitals, and 3) external testing set including the remaining one-third of hospitals. We used a gradient-boosted machine (GBM) tree-based model and two-staged approach to first identify encounters with zero DOT, then estimate DOT among those with >0.5 probability of receiving antibiotics. Accuracy was assessed using mean absolute error (MAE) in testing datasets. Correlation plots compared model estimates and observed DOT among testing datasets. The top 20 most influential variables were defined using modeled variable importance. Results: Our datasets included 629,445 training, 314,971 internal testing, and 419,109 external testing encounters. Demographic data included 41% male, 59% non-Hispanic White, 25% non-Hispanic Black, 9% Hispanic, and 5% pediatric encounters. DRG was missing in 29% of encounters. MAE was lower in pediatrics as compared to adults, and lowest for models incorporating CCSR inputs (Figure 1). Performance in internal and external testing was similar, though Goodman/Elixhauser variable strategies were less accurate in external testing and underestimated long DOT outliers (Figure 2). Agnostic and adjudicated CCSR model estimates were highly correlated; their influential variables lists were similar (Figure 3). Conclusion: Larger numbers of CCSR diagnosis and procedure inputs improved risk-adjustment model accuracy compared with prior strategies. Variable importance and accuracy were similar for agnostic and adjudicated approaches. However, maintaining adjudications by experts would require significant time and potentially introduce personal bias. If findings are confirmed, the need for expert adjudication of input variables should be reconsidered.
Disclosure: Elizabeth Dodds Ashley: Advisor- HealthTrackRx. David J Weber: Consultant on vaccines: Pfizer; DSMB chair: GSK; Consultant on disinfection: BD, GAMA, PDI, Germitec



Building a Special Pathogen Response Center from the Ground Up
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s95
-
- Article
-
- You have access
- Open access
- Export citation
SHEA position statement on pandemic preparedness for policymakers: emerging infectious threats
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 19 July 2024, pp. 1-3
-
- Article
- Export citation
SHEA position statement on pandemic preparedness for policymakers: the role of healthcare epidemiologists in communicating during infectious diseases outbreaks
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-5
-
- Article
- Export citation
SHEA position statement on pandemic preparedness for policymakers: building a strong and resilient healthcare workforce
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-4
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
SHEA position statement on pandemic preparedness for policymakers: introduction and overview
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
SHEA position statement on pandemic preparedness for policymakers: pandemic data collection, maintenance, and release
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 05 June 2024, pp. 1-5
-
- Article
- Export citation
Testing residual chloramine levels in tap water across sink locations in a US academic hospital setting
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 20 March 2024, pp. 1-2
-
- Article
- Export citation
The impact of minimally invasive surgical approaches on surgical-site infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 03 January 2024, pp. 557-561
- Print publication:
- May 2024
-
- Article
- Export citation
Strategies to maintain an N95 respirator supply during a pandemic supply-chain shortage
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 13 December 2023, pp. 688-689
- Print publication:
- May 2024
-
- Article
-
- You have access
- HTML
- Export citation
The impact of environmental cleaning protocol featuring PX-UV in reducing the incidence of multidrug-resistant gram-negative healthcare-associated infection and colonization in intensive care units in Thailand
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 13 December 2023, pp. 684-687
- Print publication:
- May 2024
-
- Article
- Export citation
Bacille Calmette-Guérin preparation and intravesical administration to patients with bladder cancer: Risks to healthcare personnel and patients, and mitigation strategies
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 4 / April 2024
- Published online by Cambridge University Press:
- 11 December 2023, pp. 520-525
- Print publication:
- April 2024
-
- Article
- Export citation
Approaching coronavirus disease 2019 (COVID-19) vaccine hesitancy among healthcare personnel: The importance of cultural competency
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 18 July 2023, pp. 1371-1372
- Print publication:
- September 2023
-
- Article
- Export citation
The role of environmental and healthcare-associated infections in Asia: Lessons learned from the coronavirus disease 2019 (COVID-19) pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 15 June 2023, e100
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Strategies to prevent Clostridioides difficile infections in acute-care hospitals: 2022 Update
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 12 April 2023, pp. 527-549
- Print publication:
- April 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Implementation should be a standard component of practice guidelines and guidance documents
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 02 March 2023, pp. 1365-1368
- Print publication:
- September 2023
-
- Article
- Export citation
Back to the future: Redefining “universal precautions” to include masking for all patient encounters
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 10 February 2023, pp. 1373-1374
- Print publication:
- September 2023
-
- Article
- Export citation
Increase in the incidence of Candida parapsilosis and Candida tropicalis bloodstream infections during the coronavirus disease 2019 (COVID-19) pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 10 January 2023, e2
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
How to measure time preferences: An experimental comparison of three methods
-
- Journal:
- Judgment and Decision Making / Volume 8 / Issue 3 / May 2013
- Published online by Cambridge University Press:
- 01 January 2023, pp. 236-249
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Asymptomatic screening for severe acute respiratory coronavirus virus 2 (SARS-CoV-2) as an infection prevention measure in healthcare facilities: Challenges and considerations
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 1 / January 2023
- Published online by Cambridge University Press:
- 21 December 2022, pp. 2-7
- Print publication:
- January 2023
-
- Article
-
- You have access
- HTML
- Export citation
