



The duration and quality of sleep of children has been decreasing over the previous two decades(Reference Matricciani, Olds and Petkov1), including in Brazil, especially due to industrial development, which has encouraged the acquisition of consumer electronics, and has led to widespread internet usage in this age group and the exacerbation of students’ appointments, which generates stress, fatigue and emotional breakdown. Additionally, the lack of options for play in the country has contributed to this finding(Reference Hoefelmann, Silva and Lopes2).
Klein and Gonçalves(Reference Klein and Gonçalves3) studying Brazilian children 7 to 11 years of age, found that 43·6 % slept less than 9 h per night and 18·6 % presented sleep disruptions, including insomnia, tiredness when waking up, daytime sleepiness and snoring. Gonzaga et al. (Reference Gonzaga, Sena and Coura4) indicated that 40·7 % of children and adolescents (n 135, 5–18 years) in the Brazilian northwest had low sleep quality, with the prevalence among girls (44·7 % v. 35·6 % male). Souza et al. (Reference Souza and Tomaz5) utilised the Sleep Disability Scale for Children (SDSC) for a group 5 to 10 years of age living on the south cost of Paraíba, and found 15·0 % hyperhidrosis among those with poor sleep quality.
There has been an increase in public discussion regarding the theme of sleep and the childhood population, mostly with regard to how sleep duration and quality influence health and, specifically, cognitive performance in education(Reference Warren, Riggs and Pentz6). Studies show an association between sleep irregularity and a negative impact on behaviour control, the emotions, and food, as well as physical fitness(Reference Collings, Wijndaele and Corder7,Reference Pereira, Teixeira and Louzada8) . Irregular sleep favours the alteration of the homeostasis of hormone secretion such as melatonin, cortisol, insulin and ghrelin, which are regulators of memory, development and energetic expense(Reference Gamble, Berry and Frank9). The US National Sleep Foundation recommends that individuals 6 to 13 years of age sleep from 9 to 10 h per night(10).
Sleep disorders can cause disturbances and psychological and behaviour problems, which arise in importance during the school phase, internalisation (sadness, discouragement, fear and loneliness), externalisation (anxiousness, depression, impatience, and rules violation) and the use or abuse of certain substances(Reference Tomé, Camacho and Matos11). Furthermore, they can culminate in a preference for the intake of food with high energetic density, mainly lipid and saturation fat(Reference Stelmach-Mardas, Iqbal and Mardas12), since the regulation neuroendocrine can be compromised. A longitudinal study with participants (n 312, 5–12 years) enrolled from the elementary schools of Aalter presented an association between reduced sleep hours and a higher intake of fatty foods and lower intake of fruit and vegetables(Reference Michels, Sioen and Boone13).
In light of the foregoing revelations, the present investigation represents a theme that is still an incipient approach, although it is important from the point of view of attention to the integral health of children and adolescents.
This study aimed to estimate the prevalence of indicators (duration and self-evaluation of quality) of the habitual sleep of the schoolchildren and the unhealthy behaviour associated with it. This information is important with regard to minimising the negative effects of sleep on social behaviour, food consumption, lifestyle, and the biological changes in the sleep-wake cycle of the population investigated.
Methods
Cross-sectional study, with data collection between 2014 and 2015, approved by the Human Research Ethics Committee. All participants gave their consent, in addition to the signed consent of mothers and/or legal guardians.
Sampling
The sample was representative of children in the 4th grade in the public elementary schools of Belo Horizonte (1·43 million inhabitants, 330·9 km2), with the phase of life represented by progressive independence and cognitive maturity(Reference Moore, Tapper and Moore14,Reference Riley15) , as well as the formation of new social entailment. For the sample calculation a proportion of 50 % was adopted for the characteristics determined for a finite population (n 10·623), a value that gives a bigger sampling size, and the level of significance and sampling error was fixed at 5 % (α or error type I), according to Hulley and Cummings criteria(Reference Hulley, Cummings and Browner16). The sampling of participants was realised by the conglomeration of two stages (schools and class) with stratification proportional to location. The sampling size (n 742) was stratified proportionally to the size of each of the nine regional administrations of Belo Horizonte. Thus, they were selected by a simple conglomerate sample of 17 schools, with a total of 931 students drawn from all genders. The exclusion criteria were the use of controlled medicines or the actual treatment of infectious diseases; respiratory (asthma, bronchitis, sinusitis and/or rhinitis) or chronic degenerative illnesses; difficult venous access; and membership in the Social Inclusion Program (with health, mental or cognitive problems), according to the teacher’s report. From the total number of invited students, 101 were not assessed for absence on the day of the data collection, 31 for mental illness, and 2 did not present the parental consent form. In the sample (n 797) under consideration, individuals whose data was incomplete or inconsistent had their evaluations excluded from the results (3 for sleep, 8 for social behaviour, 29 for food intake, 7 for nutritional status, 37 for physical activity and 23 for screen time). It should be noted that students excluded from the study have not presented differences related to sex, age or the region of the town (P > 0·05) from those who remain.
Recruitment
One subsample was adopted to establish biochemical parameters, and parameters for social behaviour as reported by teachers, to support the questions related to human, material, technical and logistical resources. Calculated according to the Campos criteria(Reference Campos17), the subsample of the biochemical parameters was estimated among 72 schoolchildren considering a percentage of loss of individuals, a confidence level of 95 %, a finite population, and a desired maximum error of 5 mg/dl, adopting the sd expected of the main outcome (total cholesterol TC)(Reference Bibiloni, Salas and Garza18,Reference Gyllenhammer, Weigensberg and Spruijt-Metz19) . Of the 797 study participants, 285 were eligible for biochemical parameters, with 177 excluded due to a negative response from the parents (n 138) or from the child (n 37), or due to difficult venous access (n 2), and 108 (37, 9 %) individuals from a total of four regional administrations were assessed. The subsample of teachers (n 7) for the evaluation of the social behaviour of the schoolchildren was obtained by agreement, totalling 31·6 % (n 252) of the volunteers analysed (Fig. 1).
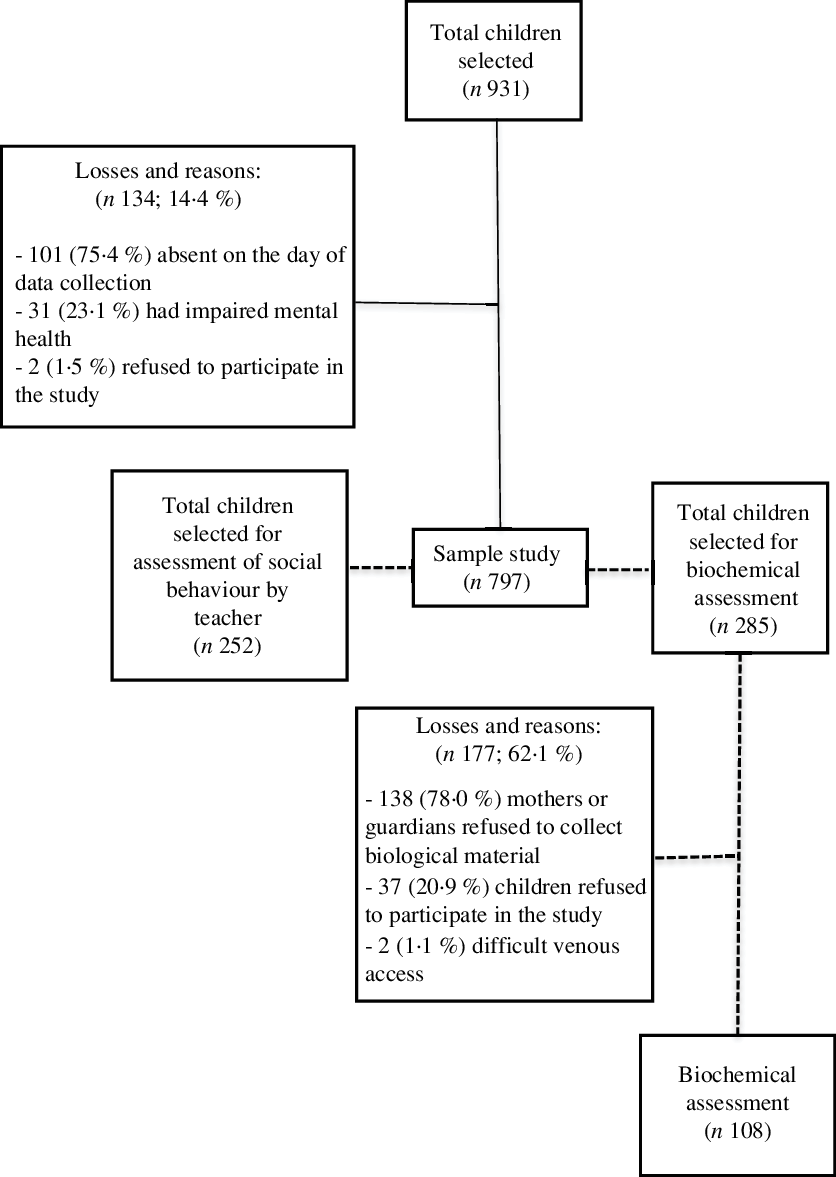
Fig. 1 Flowchart of the study sample
Instruments
A questionnaire was distributed on site to the schoolchildren in the teaching units.
Data collection
The data collection was performed by a nutritionist and academics, who specialise in nutrition in public and federal higher education institutions, and who were trained and supervised by the main researcher. The study aimed to characterise the schoolchildren’s sleep, determine its relation to social behaviour and food consumption, and, in addition, to identify how this relates to demographic, anthropometric and biochemical measurements and lifestyle.
Demographic variables
Demographic data such as sex and the birth date for the age calculation were obtained by consulting school documents.
Anthropometric variables
Height and weight measurements were taken at the school, utilising appropriated equipment and techniques. Height was assessed with a portable stadiometer (Altura Exata®) with an amplitude of 220 cm and sub-divisions of 0·5 cm, and the reading was obtained with the individual standing. Weight was assessed utilising an electronic scale (Marte LC 200 PS®) with a capacity of 200 kg and precision of 50 g. It was calculated using the anthropometrics index height-to-age (H/A) and BMI (weight(kg)/height(m)2)-to-age (BMI/A) with the help of the software WHO AnthroPlus®(20). Classification of the individual’s nutritional status was achieved utilising the charts of the World Health Organization(21). In this study, H/A was categorised as low height (score-Z < –2) and adequate height (score-Z ≥ –2), and BMI/A as eutrophic (score-Z ≥ –2 e score-Z ≤ +1), overweight (score-Z > +1 e score-Z ≤ +2) and obese (score–Z > +2)(22).
Lifestyle variables
The amount of physical activity was determined on the basis of the schoolchildren’s report regarding the weekly expenditure in hours, including the time dedicated to classes in physical education, and to sports activities, planned exercise, physically active leisure, and locomotion activities. The practice was classified according to the criteria of WHO(23), with 60 min daily or 300 min weekly considered adequate. The amount of daily screen time, an important marker of inactivity, was obtained through the following question: ‘How long do you watch TV, use your computer or mobile phone, or play video games daily?’(24). The answer was categorised as adequate time (≤ 120 min/d) or inadequate time (> 120 min/d)(Reference Scaglioni, Salvioni and Galimberti25).
Biochemical variables
Blood collection was undertaken in one subsample (n 108; 37,9 %), in the morning at the school, after 12 h of fasting, by a laboratory technician with a high degree of experience working with children, and this was explained in instructions given to the parents and schoolchildren in writing at the school and by phone. A maximum of 5·0 ml was collected from each volunteer by puncturing a vein in the fold of the elbow. The enzymatic-colorimetric methodology utilising the kit Glucose-PP and the Spectrophotometer BIOTRON BRT 811® measured the blood glucose after fasting. Schoolchildren with a concentration of glucose serum ≥ 100 mg/dl were considered to have elevated blood sugar(Reference American Diabetes26). The lipid metabolism (triglyceride TG, TC and HDL-cholesterol HDL-c) was measured using the enzymatic-colorimetric semi-automatic BIO-2000 (BIOPLUS®) method, employing the reagents of the brand Labtest Diagnóstica®. The low-density lipoprotein-cholesterol (LDL-c) was measured using the formula LDL-c = TC (HDL-c + TG/5) of Friedewald(Reference Friedewald27). Serum concentrations of TG ≥ 150 mg/dl were considered to identify excess; for TC, values ≥ 200 mg/dl were utilised to indicate an increase, HDL-c ≤ 35 mg/dl to signal deficiency, and values of LDL-c ≥ 130 mg/dl to diagnose an increase(Reference American Academy28). The analyses of the serum samples obtained were performed in the Haematology and Clinic Biochemistry Laboratory of the School of Pharmacy of the FUMG. Additionally, serum insulin, melatonin, growth hormone (GH) and cortisol were determined by sandwich ELISA, utilizing kits from R&D Systems® (Minneapolis, MN, USA) and Cloud-Clone Corporation® (Houston, TX, USA)(Reference Wilasco, Goldani and Dornelles29), in the Interdisciplinary Medical Research Laboratory of the School of Medicine of the FUMG. It considered hyperinsulinemia values > 15 mUI/ml(Reference Hegazi, Soliman and Hasaneen30). Serum concentrations of GH > 4·5 ng/ml(Reference Gamble, Berry and Frank31) and of cortisol > 20 μg/dl were declared in excess(Reference Kennaway32) Finally, results of melatonin < 30 pg/ml indicated a hormone deficiency(Reference Kennaway32).
Outcome variables
Social behaviour
For the analysis of the social behaviour of the individuals under consideration, the Strengths and Difficulties Questionnaire (SDQ) was utilised, and it was validated for the Brazilian population(Reference Saud and Tonelotto33) through interviews with the schoolchildren. It is a simple self-evaluation instrument featuring an easy application that contains 25 items to identify difficulties and capacities perceived by the individual about their social and emotional behaviour in five domains: hyperactivity problems, conduct, emotional symptoms, relationship problems with colleagues, and pro-social behaviour. Each item on the questionnaire is divided into three responses (false, more or less true, and true), and scores (1, 2 and 3) are pre-determined, for the most part. The total result from the sum of the scales of all 20 items in the first four domains was calculated (obtaining a minimum score of 0 and a maximum of 40 points) to obtain a score of difficulties with values ≥ 26 points (average score plus 2 sd, percentile 95 p95), according to the scale proposed by Biggs et al. (Reference Biggs, Lushington and Heuvel34), indicating the worst social behaviour (inadequate). The same was performed for pro-social behaviour, with five items and a score from 0 to 10 points, which is considered inadequate for values ≤ 9 points (p95). In a similar way, teachers who signed the consent form also answered the SDQ with the aim of evaluating this characteristic and the reliability of the report on the schoolchildren, as this verification was made in one subsample of the volunteers (n 252, 31·6 %). To assess the responses of the teachers who agreed to participate in the study and signed the consent form (n 7), the difficulties score ≥ 20 points for inadequate social behaviour was adopted. The score of the pro-social domain was kept equal to that of the children(Reference Biggs, Lushington and Heuvel34). In the study, the schoolchildren not evaluated by a teacher have not presented differences regarding sex, age and city region (P > 0·05) versus those who were evaluated.
Food consumption
The energy intake of macronutrients and micronutrients, involved in brain formation, immunological and cognitive maturation (magnesium, zinc, vitamin B3 and B6)(35), of the schoolchildren was analysed through the average of two 24 h recalls on non-consecutive days. The participant stated what s/he had consumed in terms of food and drink, with the respective methods of cooking where applicable, on the previous day of the interview(Reference Menezes, Horta and Santos36). Another day was booked for the interviewer to return to the school and apply the second R 24 h with a maximum break of 7 d. Household measurement tools usually utilised in eating and drinking (e.g. glasses, spoons, etc) were presented to the individuals with the aim of obtaining a more precise report with regard to the quantities of food and drink consumed. The data on food and drink intake provided by the schoolchildren using household measurement tools were tabbed in the software Brasil Nutri and converted to units of weight and volume (grams and millilitres). Afterwards, they were correlated with the respective information regarding nutritional composition, according to the methodology proposed by the Brazilian Institute of Geography and Statistics(37) for the treatment of data on dietary intake from the Search for Family Budgets 2008/2009. To assure greater consistency of the information, data on energetic intake under 2092 kJ (n 2) or above 20 920 kJ (n 16) per day of the sample of the study were excluded(Reference He, Bixler and Berg38). To verify the relation between nutrients and the duration of sleep, the adjustment of the total caloric intake according to the method of nutrient density was utilised, which was the result of the multiplication of the value of the intake of each nutrient by 418·4 kJ divided by the total energy consumed(Reference Cavalcante, Moreira and Mota39). The macronutrients, the SFA and the fibres were evaluated in g/4184 kJ, and the cholesterol and the micronutrients were analysed in mg/4184 kJ.
Sleep
A questionnaire was used for the children in the teaching units to assess their sleep time on weekdays (Sunday to Monday and Monday to Thursday) and weekends (Friday to Saturday and Saturday to Sunday). The sleep duration (h) was obtained from the difference between the average of the sleep hours and the wake-up time on seven consecutive days and categorised in < or ≥ 9 h(10), inadequate and adequate, respectively, according to sleep hours proposed by Klein and Gonçalves(Reference Klein and Gonçalves3). A bedtime between 8 pm and 10 pm and a wake-up time between 5 am and 7 am were considered adequate(Reference Gonzaga, Sena and Coura4,Reference Kobayashi, Yorifuji and Yamakawa40) . The alterations in sleep (snoring, moving the legs, speaking, walking during sleep, and difficulty in getting to sleep) were self-reported by the schoolchildren(Reference Louzada and Menna-Barreto41) and identified in terms of the frequency of occurrence (never, sometimes and always). The school shift was evaluated with the propose of explaining its influence over the total number of hours of sleep. The habit of taking a shower before school and its respective frequency of occurrence (never, sometimes and always) was also questioned in order to evaluate the influence of that practice on sleep duration, besides being positive with regard to contributing to alertness throughout the day(Reference Pereira, Teixeira and Louzada8). The indicator of sleep quality was self-evaluation based on the question: ‘During the last 30 d (in general) how do you classify the quality of your sleep?’, and the options for the answers were ‘very good’, ‘good’, ‘poor’ or ‘very poor’(Reference Klein and Gonçalves3). The variables ‘very good’ and ‘good’ were grouped and categorised as adequate sleep quality; and ‘poor’ and ‘very poor’ as inadequate sleep quality(Reference Pereira, Teixeira and Louzada8).
Statistical analyses
The descriptive analysis was realised including measures of the central tendency and of the dispersion. The Kolmogorov Smirnov test was applied to evaluate the adhesion of the variables to normal distribution. The majority of the variables presented non-normal distribution, opting for standard presentation of the results (median; min-max).
To evaluate the relation between sleep duration on weekdays and weekends, and the reliability of children’s school records versus teachers’ scores regarding strengths and difficulties of social behaviour, Spearman’s correlation test was used. The strength of the correlations was considered weak when the coefficients were smaller than 0·30, moderate when the values of r presented between 0·40–0·60, and strong when r was higher or equal to 0·70(Reference Dancey and Reidy42). The association between the duration of sleep, which was stratified as adequate or inadequate, and sex, nutritional status, sleep and wake-up time, and sleep quality, was conducted for Chi-square or Fisher’s exact test; it included the Bonferroni correction for the variables pertaining to the school shift and showering before the class. To compare the relation between sleep duration (hours per night), age, physical activity, screen time, biochemical parameters, social behaviour, and food consumption the MannWhitney test was applied.
The influence of sleep quality (independent variable) in the alterations in sleep and social behaviour (dependent variables) was tested through the Multinomial and Binary Logistic Regression, respectively. Confounding factors such as sex, age, screen time, bedtime and wake-up time were included as adjustments in these models. No violation of supposition was found in the analysis. OR and 95 % CI were used as a measure of effect.
The Stata version 13.0 was utilised to analyse the data, adopting a value of significance of 5 %.
Results
A total of 797 schoolchildren were evaluated, 50·9 % (n 406) of whom were female with a median of 9·7 (9·5–10·0) years of age and energy intake of 7613·6 (5982·7–9766·2) kJ. Excess weight (overweight/obese) was identified in 31·6 % of the sample, and 76·8 % reported insufficient weekly physical activity (< 300 min).
The daily limit of screen time (≤ 120 min) was exceeded by 46·9 % of the participants. One hundred percent of the schoolchildren presented normal values for blood glucose after fasting, TG and all hormones. Biochemical alterations were identified for TC (2·8 % above), LDL-c (6·7 % with high values) and HDL-c (19·8 % below). Additional information is described in Table 1.
Table 1 Relationship between the characteristics of schoolchildren and sleep duration in median (min-max), percentage and P values, in Brazil, 2014–2015
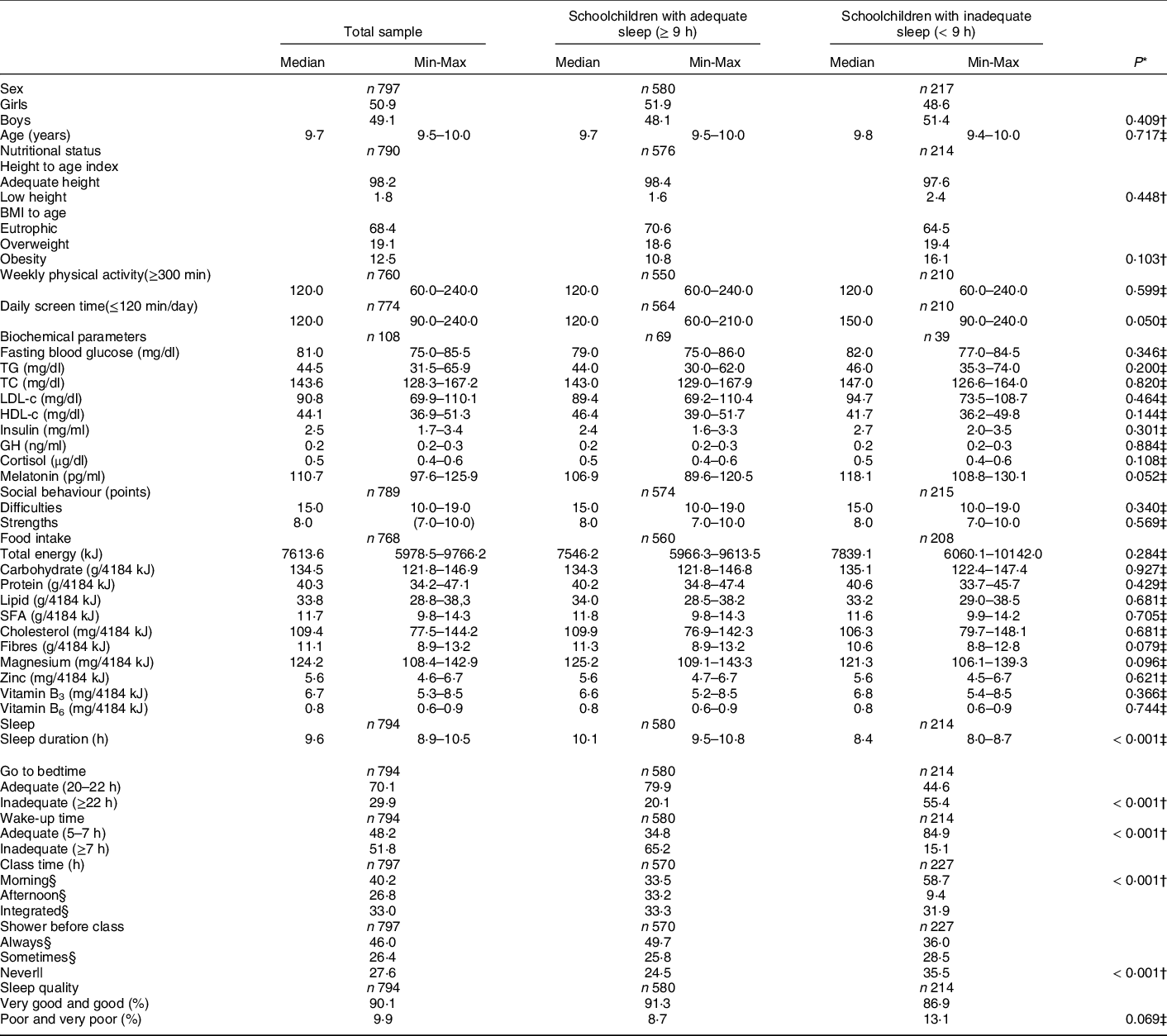
TG = Triglyceride; TC = Total Cholesterol; LDL-c = Low Density Lipoprotein-Cholesterol; HDL-c = High Density Lipoprotein-Cholesterol; GH = Growth Hormone; SFA = Saturated Fatty Acids; B3 = Niacin; B6 = Pyridoxine; Min = minimum; Max = maximum; % = percentage.
* P values tested the difference between schoolchildren with adequate or inadequate sleep for each characteristic analysed.
† Chi-square or Fisher‘s exact tests.
‡ Mann-Whitney.
§ Proportions with different letters are statistically different according to Bonferroni correction.
|| Proportions with equal letters are statistically equal according to Bonferroni correction. Sampling size different due to absence or inconsistency of information and study methodology.
In relation to social behaviour, a median of difficulty of 15·0 (10·0–19·0) points was noted, with 5·6 % of the schoolchildren exceeding the maximum score for this parameter. The median of capability was 8·0 (7·0–10·0) points, and 70·0 % of the schoolchildren presented results below the minimum for this domain (Table 1). There was a weak correlation between scores indicating difficulty in social behaviour described by schoolchildren and teachers (r = 0·194, P = 0·002).
The sleep duration presented a median of 9·6 (8·9–10·5) h and was smaller on weekdays: 9·3 (8·5–10·2) versus 10·5 (9·5–11·5) h at the weekend (P < 0·001). There were no associations between sleep duration independent of the day of the week and the variables of demography, nutritional status, physical activity, biochemical parameters, social behaviour and food consumption. Inadequate sleep duration was identified in 27·0 % of the sample and higher among the schoolchildren who remained in front of a screen above the recommended time per day (P = 0·05), with an inappropriate bedtime or adequate wake-up time among the schoolchildren studied during the morning shift (P < 0·001) who never took a shower before school (P < 0·001).
Finally, 9·9 % of the schoolchildren classified the quality of their sleep as poor or very poor. The negative assessment of the self-evaluation of sleep quality was significantly related to the increase in sleep alterations and the inadequacy of social behaviour evaluated by the schoolchildren.
The self-evaluation of poor and very poor sleep quality, for example, was associated, after adjustment for the confounding factors, with the higher probability of always speaking while sleeping (OR = 2·82; 95 % CI: 1·43, 5·53) and having difficulty in getting to sleep (OR = 4·75 times; 95 % CI: 2·43, 9·25), but not walking while sleeping (OR = 0·88; 95 % CI: 0·20, 3·84). Lastly, the negative assessment of the self-evaluation of sleep quality was consistently associated with inadequate social behaviour according to an assessment of the schoolchildren (OR = 5·53; 95 % CI: 2·74, 11·18) (Table 2).
Table 2 Multinomial and binary logistic regression between self-evaluated sleep quality and alterations in the sleep and social behaviour of schoolchildren in Brazil, 2014–2015

Binary Logistic Regression = Social Behaviour; Multinomial Logistic Regression = Alterations in sleep; OR = Odds Ratios, CI = Confidence Intervals.
* Adjusted for sex, age, screen time, bedtime and wake-up time.
† The categories Never and Adequate were considered as references in the analyses.
‡ P<005 for trend in outcome.
§ P<0·01.
Discussion
This study reviewed the relationship between sleep duration and self-evaluation of the quality of social behaviour, food consumption, demographic and nutritional conditions, lifestyle, and the biochemical parameters of a representative sample of schoolchildren from a Brazilian metropolis.
At least one third of the population investigated presented inadequate sleep duration, mainly on weekdays, and it was observed that there was an association with screen time, total sleep hours, bedtime and wake-up time, school shift, and showering before class. As many as 1 in 10 children surveyed indicated unsatisfactory sleep quality in their self-evaluation. A negative assessment of sleep quality in the self-evaluation was associated with a higher probability of always talking while sleeping, having difficulty to getting to sleep, and inadequate social behaviour, after making adjustments for demographic factors and lifestyle.
The reduced sleep duration identified in the present study was also found in other investigations concerning schoolchildren(Reference Matricciani, Olds and Petkov1,Reference Klein and Gonçalves3) . The fact that the duration is smaller on weekdays (versus during the weekend) reflects an increase in social obligations, academic demands and exposure to technology (such as TV, video games, computers and social networks), and the specifics of class days and this phase of life(Reference Keller, Smith and Gilbert43). In the study Pasch et al. (Reference Pasch, Laska and Lytle44), short sleep duration during the week was more predictive of risks, such as fatigue, daytime sleepiness, depression and aggressiveness, when compared to the weekend, suggesting that the increase in sleep hours during the weekend is not sufficient to protect schoolchildren from the outcome behaviours resulting from the accumulated loss of weekly sleep. In the present study, despite the difference in sleep duration between weekdays and the weekend, there was no different association with the variables investigated when studying sleep in these moments.
The insufficient quantity of sleep hours shown is associated with excessive daily screen time (51·9 %), as well as with an inadequate bedtime and wake-up time, with more than half of the sample (55·4 %) going to bed after 10 pm and 15·1 % waking up after 7 am. This result corroborates with the study scots children whose screen time also was associated with delayed sleep onset(Reference Woods and Scott45). In the study conducted by Magee et al. (Reference Magee, Gordon and Caputi46), children with persistently short sleep presented worse physical (indisposition), emotional and social health versus those with normal sleep. Kobayashi et al. (Reference Kobayashi, Yorifuji and Yamakawa40) conducted research on Japanese children 8 years of age and noted that an irregular or late (after 11 pm) bedtime was positively related with aggressiveness and attention problems in relation to an earlier bedtime (before 9 pm). In contrast, there was no evidence of an association between sleep and physical activity. The sufficient practice of weekly physical activity could contribute to the reduction of the problems above, but studies have demonstrated that cultural, economic and geographical aspects, and also technological advances are important barriers to the practice of physical activity(Reference Dresch, Bertoli and Silva47).
Additionally, in our study of short sleep duration the morning school shift was the primary period when that occurred, as the schoolchildren delayed their bedtime and woke up early to study; this contributed to a daily loss of sleep which, consequently, could lead to daytime fatigue, reduced learning and cognitive performance, and sedentary behaviour(Reference Foley, Maddison and Jiang48). Taking a shower before class may be a possible recommendation to reduce the negative effects of reduced sleep hours (8 h) and increase the attention span in the classroom, but not more than 36 % of individuals with inadequate sleep hours reported always performing this practice.
In 2014, Becker determined that insufficient sleep remained significantly associated with anxiety, as well as with the worst academic performance and social behaviour, evaluated by the child and teacher(Reference Becker49). Other authors observed significant correlations between reduced sleep duration and an increase in the internalization and externalization of the scores in 1·622 children, from 5 to 10 years of age(Reference Biggs, Lushington and Heuvel34). However, in the present study no association was identified between sleep duration and social behaviour assessed by schoolchildren and teachers. Such findings may be related to the adaptation of the Brazilian schoolchildren to routine and daily adversity, considering that significant differences were not found in socioeconomics in all the variables analysed, despite known situations regarding social vulnerability(Reference Nahas50) in a significant percentage of the research population(Reference Carmo, Almeida and Oliveira51).
In contrast to other investigations, in the study referred to, associations of short sleep duration with higher energy, or carbohydrate or lipid ingestion by schoolchildren were not observed. In an intervention study, Hart et al. (Reference Hart, Carskadon and Considine52) detected higher energy intake during one week of restricted sleep (< 6 h). Other studies also suggested a relationship between inadequate sleep and intake of determined macronutrients, such as carbohydrates and fat. Weiss et al. (Reference Weiss, Xu and Storfer-Isser53), for example, asserted that short sleep duration (< 8 h) was associated with a higher proportion of energy intake via lipids, but with a reduction in carbohydrates.
A similar cut-off point for sleep hours (< 6 h) was also tested in the sample for this study, and the results were not different from those described above. Children registered in the public school system have the benefit of a healthy diet resulting from the inclusion of schools in the National School Feeding Program, which provides a better approach to the meal quality offered to schoolchildren, as the menu is devised by a nutritionist respecting local and cultural eating habits, with better monitoring of food and nutrition education of actions. Furthermore, this study was realised in an open environment, since the participants practised their normal daily routine without using control protocols. Even with regard to the existing association between inadequate sleep and food consumption, it seems that this relation becomes evident in experimental studies where the individuals under consideration are submitted to protocols and if the sleep duration is excessively reduced(Reference Bennett, Truby and Zia54). In addition, changes in fasting blood glucose and serum lipid and hormonal profiles were not identified in the results, which reinforce the absence of associations.
However, significant associations between the self-evaluation of sleep quality and sleep alterations and social behaviour were detected in the present study and deserve to be highlighted. The authors found that the increase in the prevalence of poor and very poor sleep quality increased the likelihood of schoolchildren always presenting sleep alterations and inadequate social behaviour in relation to those with good and very good sleep quality. Poor sleep quality seems to contribute to the development of sleep disorders, as well as depression, anxiety and low self-esteem(Reference Maia, Sousa and Azevedo55). Research conducted with Israeli children 7 to 13 years of age noted that lower sleep efficiency and higher nocturnal awakening predicted poor performance in processing emotional information(Reference Soffer-Dudek, Sadeh and Dahl56). In the study by Telzer et al. (Reference Telzer, Fuligni and Lieberman57), poor sleep quality was associated with risk behaviour, suggesting an imbalance between the affective and cognitive control systems. Similarly, sleep serves as a filter preventing memory loss and impulsivity, for example, which confirms the important role of parents and the relevance of establishing limits on sleep. It is presumed that a family that provides a favorable environment for good sleep quality is associated with less inadequacy of social behaviour and better or healthier choices made by children and adolescents.
In general, such discoveries highlight the necessity of paying greater attention to the intense changes that have occurred in the contemporary way of life of children and adolescents, and that more independence, together with the frequency and intensity of activities and the inconsistency of social resources, is not always healthy(Reference Ferreira, Rombaldi and Ricardo58). In this sense, actions aimed at the formation of good sleep and life habits are essential at school age. Additionally, there are demands on several actors (schools, children, parents, multi-professional staff, and public institutions) in this process.
It should be noted that the potential of this research is due to the deficiency of studies on this subject, focusing on this age range and with the defined sample size, in Brazil. Moreover, it highlights the utilization of a validated questionnaire for social behaviour evaluation, with appropriated statistical methods and adjustments for confounding factors in order to relate sleep duration and self-evaluation quality to sleep alterations, social behaviour and food consumption.
However, some limitations should be noted: 1) the socioeconomic characteristics of the sample, since only children from public school were evaluated, bearing in mind that it is an urban population whose geographic variability and increasing industrialisation provide more heterogeneous life and consumption habits; 2) the cross-sectional design, in which, to establish a casual relationship, longitudinal studies are indicated in order to elucidate the subjacent mechanisms of how sleep duration and quality influence the social behaviour and food consumption of schoolchildren over time(Reference Quach, Mensah and Hiscock59); and 3) the difficulty in validating the variables collected for the age group studied. Nevertheless, the results of the present study are relevant to guide future approaches to public health guidelines, in recommending that these individuals have an adequate sleep duration and quality.
Acknowledgements
Acknowledgements: The authors thank the children and schools for their important participation, and the staff of the Public Health Research Program at the Federal University of Minas Gerais for their dedication in collecting data from the population, which was carried out with the preservation of dignity and respect, and for their financial support. Financial support: This work was supported by the Federal University of Minas Gerais, Foundation for Research Support of Minas Gerais (FAPEMIG), and the National Council of Scientific and Technological Development (CNPq). Conflict of interest: All the authors declare no conflicts of interest. Authorship: A.C.S. designed the study; led the extraction and analysis of data, paper selection and data interpretation with L.C.S. and A.C.S., and E.L.M.V. performed the hormone analysis. ACS drafted the manuscript. A.C.S. and L.C.S. critically revised the manuscript and approved the final draft. A.C.S. is the guarantor for the study. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by Research Ethics Committee of the Federal University of Minas Gerais – UFMG (ETIC 00734412.0.0000.5149). Verbal informed consent was obtained from all schoolchildren participants and formally recorded.



