



Sleep is a fundamental biological requirement vital for physical and mental health. Inadequate or reduced sleep quality has wide-ranging negative effects on health and everyday living(Reference Adams, Appleton and Taylor1,Reference Hansen, Capener and Daly2) . For example, sleeping <6–7 h/d has been associated with increased risk of obesity(Reference Wu, Zhai and Zhang3), diabetes(Reference Cappuccio, D’Elia and Strazzullo4), hypertension(Reference Gangwisch, Heymsfield and Boden-Albala5) and heart disease(Reference Adams, Appleton and Taylor1,Reference Cappuccio, Cooper and D’Elia6) . Poor sleep also reduces natural immune function, which increases the risk of infections and even cancer(Reference Irwin, McClintick and Costlow7). Insomnia and self-reported poor sleep quality are associated with increased risk of mortality(Reference Adams, Appleton and Taylor1,Reference Kripke, Garfinkel and Wingard8,Reference Kurina, McClintock and Chen9) . Sleep disturbances have also been reported to cause derangements in mood, concentration, thinking, learning, memory, alertness and reaction times(Reference Van Someren, Cirelli and Dijk10). Such disturbances can affect daily living, work performance and significantly increase the risk of road traffic accidents. Ultimately, sleep disturbances produce a notable burden on public health, social life and workplace functioning(Reference Adams, Appleton and Taylor1).
It is particularly common for young adults to experience poor sleep quality or disturbed sleep(Reference Adams, Appleton and Taylor1,Reference Lund, Reider and Whiting11–Reference Coren13) . Many factors can underlie this, including the presence of a sleep disorder such as insomnia (defined as difficulty initiating and maintaining sleep) and lifestyle behaviours(Reference Cormier, Walker, Hall and Hurst14). The 2016 Australian Sleep Health Survey, and the Sleep Health Foundation’s recent report, found symptoms of excessive daytime sleepiness (i.e. sleepiness, fatigue or feeling irritable) were significantly more common among younger age groups than older adults, with these problems occurring in around half of 18–24-year-olds, twice the level of those aged >65 years(Reference Adams, Appleton and Taylor1,15) . Pathological daytime sleepiness, where people describe a strong tendency to doze off, as assessed by the Epworth Sleepiness Scale (ESS), was also found to be significantly more common in younger adults than in older adults, as was insomnia(Reference Adams, Appleton and Taylor1). Significant sex differences also exist whereby difficulties related to sleep onset and maintenance, insomnia and daytime sleep-related symptoms are more common in females than males(Reference Adams, Appleton and Taylor16–Reference Ohayon, Reynolds and Dauvilliers19).
Lifestyle behaviours, such as the consumption of caffeine, can also influence sleep negatively. Caffeine is a central nervous system and cardiac stimulant which acts as an antagonist to adenosine, a chemical that has been shown to promote sleep and to influence autonomic nervous system arousal(Reference Lohsoonthorn, Casillas and Lertmaharit20). The consumption of caffeine-containing beverages, such as coffee and tea, has been linked with sleep disturbances. For example, double-blind randomised controlled studies have shown that ingesting caffeinated coffee, particularly in the evening, has significant negative effects on sleep quality, sleep latency and frequency of waking, compared with ingesting decaffeinated coffee(Reference Lloret-Linares, Lafuente-Lafuente and Chassany21,Reference Distelberg, Staack and Elsen22) . Furthermore, the 2016 Australian Sleep Health Survey found 61 % of adults who consumed six or more cups of tea or coffee per d experienced two or more sleep problems (i.e. difficulty falling asleep, repeated overnight waking, daytime fatigue or exhaustion, irritability or moodiness, or excess daytime sleepiness (ESS > 10)), compared with 40 % of adults who did not drink tea or coffee(Reference Adams, Appleton and Taylor1).
Energy drinks (ED) are another type of stimulant drink which have the potential to affect sleep. ED are defined by Food Standards Australia New Zealand as, ‘flavoured non-alcoholic beverages to which other substances have been added, that: (a) contain caffeine; and (b) have the purpose of enhancing mental performance’(23). The use of these drinks has increased dramatically amongst young people over recent years. Indeed, ED represent the fastest growing segment of the beverage market, with annual sales in Australia increasing more than 600 % between 2001 and 2012(24). In 2015, it was reported that the global ED market was worth 38·2 billion euro globally (approximately 55 billion AUD), with a further 40 % growth forecast by 2020(Reference Starling25).
Caffeine is a key ingredient in ED and is capped at 80 mg/250 ml (equivalent to an instant cup of coffee) in Australia(23). However, other countries, such as the USA and the UK, have no restrictions on the amount of caffeine ED can contain. Aside from caffeine, other ingredients commonly found in ED include sugar, Na, B vitamins, amino acids, colourings, flavourings and herbal stimulants, all of which may act synergistically with the caffeine to enhance its stimulatory effects(26–Reference Finnegan28). Current evidence shows that adolescents (13–17 years) and young adults (18–34 years) are the most frequent users of ED, with around a third to a half reporting regular use(Reference Mitchell, Knight and Hockenberry29–Reference Trapp, O’Sullivan and Robinson33). Amongst these age groups, common reasons for consuming ED include helping them stay up late to party, complete assignments or exams, work, drive at night or long distances and for video game sessions(Reference Francis, Martin and Costa34,Reference Treloar, Tidwell and Williams35) .
Despite the popularity of ED amongst young adults and the high prevalence of sleep problems in this age group, few studies have investigated the relationship between ED consumption and sleep. Internationally, studies have consistently reported positive associations between ED use and sleep disturbances amongst college students from a wide range of ethnic backgrounds including the USA(Reference Stasio, Wagener and Glassman36), the United Arab Emirates(Reference Faris, Jahrami and Al-Hilali37), Saudi Arabia(Reference Alsunni and Badar38), Chile(Reference Vélez, Traslaviña and Barbosa39), Thailand(Reference Lohsoonthorn, Casillas and Lertmaharit20) and Peru(Reference Sanchez, Martinez and Oriol40). However, the extent to which behaviours in college populations reflect similar behaviours in the wider population is unclear. For example, comparative analysis studies conducted in Australia and the USA have found significant demographic and behavioural differences between college and non-college research participants; college students participating in research studies are more likely to be white, female, have attended independent schools, have lower incomes, live with their parents, be from higher socio-economic backgrounds and be more risk-averse than their non-college counterparts(Reference Gainsbury, Russell and Blaszczynski41–Reference Barnes, Welte and Hoffman43). To date, only one study has investigated the relationship between ED use and sleep disturbances within a population-based sample. This US study found ED use to be associated with an increased risk of difficulty in falling and staying asleep, as well as insufficient duration of sleep in males aged 20–34 years(Reference Larson, Laska and Story44). This study highlights the need for further research involving population-based samples of both males and females in order to better understand the relationship between ED use and sleep disturbances in young adults. Furthermore, only two studies to date have stratified their results by sex, which is surprising given the differences in sleep patterns and risk for sleep disturbances between males and females(Reference Adams, Appleton and Taylor16–Reference Ohayon, Reynolds and Dauvilliers19,Reference Larson, Laska and Story44) . The purpose of this study, therefore, was to investigate the association between ED use and sleep disturbances in a population-based sample of young adults from the Raine Study, and to stratify the results by sex.
Methods
Participants
This study draws data from the Raine Study, which has collected thousands of social, physical and medical measurements on each participant from gestation to young adulthood. Full details about the Raine Study have been published elsewhere, see Newnham et al. (Reference Newnham, Evans and Michael45) and Straker et al. (Reference Straker, Mountain and Jacques46). Briefly, between 1989 and 1991, 2900 pregnant women (at 16–20 weeks gestation) were recruited from public and private antenatal clinics across Perth, Western Australia. Living infants were born to 2804 (97 %) of these women and owing to multiple births produced a cohort of 2868. This cohort and their families have been monitored regularly. This study focuses on data from the cohort (called Gen2 participants) when they were 22 years of age (Gen2_22) as this was the only time point where ED use and sleep data were both collected. Data collection for the Gen2-22-year follow-up occurred during 2012 to 2014, and of the 2262 young adults eligible, 1234 (55 %) participated. Socio-demographic variables measured at birth were also used in the study.
Loss to follow-up
Details about cohort attrition have been published previously(Reference Straker, Mountain and Jacques46–Reference Robinson, Oddy and McLean48). At the time of the Gen2-22 years follow-up, 565 of the cohort had withdrawn from the study, 41 had died and 1029 had deferred or were lost to follow-up(Reference Straker, Mountain and Jacques46). Families lost to follow-up were characterised by greater socio-economic disadvantage at the time of enrolment compared with families who continued in the study(Reference Straker, Mountain and Jacques46).
Assessment of energy drink use
Participants were asked about their frequency of ED intake in a confidential self-report questionnaire. Usage options were: never, <1 month, 1 d/month, 2 d/month, 3 d/month, 1 d/week, 2 d/week, 3 d/week, 4 d/week, 5 d/week, 6 d/week and every day. Responses were collapsed into three usage categories: none/rare (never to ≤once/month); occasional (>once/month to <once/week) and frequent (≥once/week).
Assessment of daytime sleepiness, sleep quality and insomnia
Three validated self-administered questionnaires were used to assess various sleep-related domains: the ESS, the Functional Outcomes of Sleep Questionnaire (FOSQ-10) and the Pittsburgh Sleep Symptoms Questionnaire–Insomnia (PSSQ-I).
The ESS is widely used in the field of sleep medicine as a subjective measure of an individual’s daytime sleepiness(Reference Johns49). It consists of a list of eight different situations where participants rate their usual chance of ‘dozing off’ or falling asleep in recent times. The scales range from 0 (no chance of dozing), 1 (slight chance of dozing), 2 (moderate chance of dozing) to 3 (high chance of dozing). These scores were added to provide a continuous ‘ESS Total Score’ ranging from 0 to 24, where the higher the score, the higher the level of daytime sleepiness. ESS scores ≥10 are considered to indicate that excessive daytime sleepiness is present(Reference Johns50). Using this established cut-off, an ‘ESS Binary’ variable was also created where 0 indicated excessive daytime sleepiness was not present and 1 indicated excessive daytime sleepiness was present.
The FOSQ-10 is used to assess functional status resulting from daytime sleepiness and has been used commonly as a measure of sleep-related quality of life across five subscales(Reference Büttner, Feier and Galetke51). Participants rate the difficulty they had in undertaking ten everyday activities due to being too sleepy or tired, including when operating a motor vehicle, watching a movie, or visiting family and friends.
Ratings are 0 (do not do this activity for other reasons), 4 (no difficulty), 3 (a little difficulty), 2 (moderate difficulty) and 1 (extreme difficulty). The FOSQ-10 is measured continuously with a maximum possible score of 20. A lower score indicates greater impact of daytime sleepiness on daily activities. When scoring, an average score is calculated for each of the five subscales, these are totalled resulting in a total score. Responses from activities in which the respondent does not do this activity ‘for other reasons’ are not included in the average values for the subscales and thus not used in the calculation of the total score either. Of note, for the Gen2–22 years Raine Study follow-up, the responses were reverse-coded; thus, the ratings in the Raine questionnaire were 0 (do not do this activity), 1 (no difficulty), 2 (a little difficulty), 3 (moderate difficulty) and 4 (extreme difficulty). Therefore, for this data set, a higher score indicates greater impact of daytime sleepiness on daily activities.
The PSSQ-I(Reference Okun, Kravitz and Sowers52) (also known as the Insomnia Symptom Questionnaire) was used to determine whether participants have an insomnia disorder. It comprises thirteen self-rated questions where participants are asked to identify how frequently they have experienced five common sleep complaint symptoms during the prior month. Ratings were 0 (never), 1 (do not know), 2 (rarely – less than once a week), 3 (sometimes – 1–2 times per week), 4 (frequently – 3–4 times per week) and 5 (always – 5–7 times per week). If a participant experienced any symptom, they were asked to report how long each one had persisted in weeks, months or years. Symptomatic participants were also asked a further eight questions to determine how their sleep affected daily life, with options for each item being 0 (not at all), 1 (a little bit), 2 (moderately), 3 (quite a bit) and 4 (extremely). Answering ‘frequently’ or ‘always’ to select sleep symptom criteria (i.e. having difficulty falling asleep, difficulty staying asleep or feeling that your sleep is unrefreshing), as well as having prolonged symptoms (≥4 weeks), and responding ‘quite a bit’ or ‘extremely’ to at least one daytime impairment question resulted in a diagnosis of insomnia disorder being assigned.
Adjustment variables
Potential confounding variables included: family income at birth (low income, i.e. AU$0–35 999 per annum v. high income i.e. ≥AU$36 000 per annum); mother’s educational qualification level at birth (school only v. post-school qualification); highest education level completed at 22 years (school only v. post-school); smoking status at 22 years (yes v. no); alcohol consumption at 22 years (g/d ethanol), measured via the self-administered Anti-Cancer Council of Victoria Food Frequency Questionnaire(Reference Hodge, Patterson and Brown53); caffeine from other sources (mg/d) including black and green tea, instant and ground coffee and caffeinated soft drinks, measured via the Anti-Cancer Council of Victoria Food Frequency Questionnaire(Reference Hodge, Patterson and Brown53); physical activity at 22 years (met min/week), assessed using the short-form of the International Physical Activity Questionnaire(Reference Booth, Ainsworth and Pratt54); BMI at 22 years (weight in kg divided by height in metres squared, measured objectively by a trained research assistant using standard calibrated equipment); depression, anxiety and stress symptoms at 22 years, measured by the short-form depression, anxiety and stress scales (DASS-21)(Reference Lovibond and Lovibond55); and marijuana, stimulant, depressant and other recreational drug use at 22 years, assessed via self-report questionnaire with response options coded as never/once, occasional (<weekly) or frequent (≥weekly).
Statistical methods and control variables
Descriptive statistics were computed for all variables and stratified by ED use and sex. When comparing frequent v. none/rare categories of ED use, independent samples t tests used for continuous variables and χ 2 tests used for categorical variables. Regression modelling was used to estimate the association between ED use and sleep problems at age 22. Linear regression models were used for the FOSQ-10 score, and logistic regression models for the binary outcomes arising from the ESS and PSSQ-I. Analyses were stratified by sex. All models included the following covariates as potential confounders: family income at birth; mother’s educational qualification level at birth; highest education level completed; smoking status; alcohol consumption; caffeine from other sources; physical activity; BMI; DASS-21 depression, anxiety and stress scores; and, marijuana, stimulant, depressant and other recreational drug use.
Results
The sample characteristics and prevalence of ED use are presented in Table 1. In total, 1115 participants from the Raine Study (53·7 % females and 46·3 % males) provided data on their ED use at the 22-year follow-up. Of these participants, 66 % reported they never or rarely (i.e. ≤once/month) used ED, 17·0 % reported they were occasional users (i.e. >once/month to <once/week) and 17 % reported they were frequent users (≥once/week). When ED use was stratified by sex, a higher proportion of females reported never or rarely using ED, compared with males (74 % v. 57 %), whereas a higher proportion of males used ED on an occasional (19 % v. 15 %) or frequent (24 % v. 11 %) basis.
Table 1 Sample characteristics at 22-year follow-up, stratified by sex and energy drink use†

FOSQ-10, Fundamental Outcomes of Sleep Questionnaire; ESS, Epworth Sleepiness Scale; DASS, Depression Anxiety Stress Scale; PSSQ – Insomnia, Pittsburgh Sleep Symptoms Questionnaire–Insomnia.
† Denominators show numbers for which data were available.
‡ ≤once/month.
§ >once/month to <once/week.
‖ ≥once/week.
* P values for comparison of frequent v. none/rare categories of energy drink use. Independent samples t tests used for continuous variables and χ 2 tests used for categorical variables.
In terms of the sleep domains for the whole sample, the mean ESS total score was 5·7 ± 3·5 (range 0–19) and the mean FOSQ-10 score was 7·2 ± 2·1 (range 0–16). Just over 7 % were classified as having an insomnia disorder as measured by the PSSQ-I, and 14·5 % were classified as having excessive daytime sleepiness as measured by the ESS binary variable. When stratified by sex, females scored higher than males on all four sleep disturbance measures: 10·2 % of females v. 4 % of males were classified as having an insomnia disorder as measured by the PSSQ–I; 16·1 % of females v. 13 % of males were classified as having excessive daytime sleepiness as measured by the ESS binary variable; mean female FOSQ-10 scores were 7·5 ± 2·2, mean male FOSQ-10 scores were 6·8 ± 2·1; mean female ESS total scores were 6·1 ± 3·5 and mean male ESS total scores were 5·3 ± 3·5.
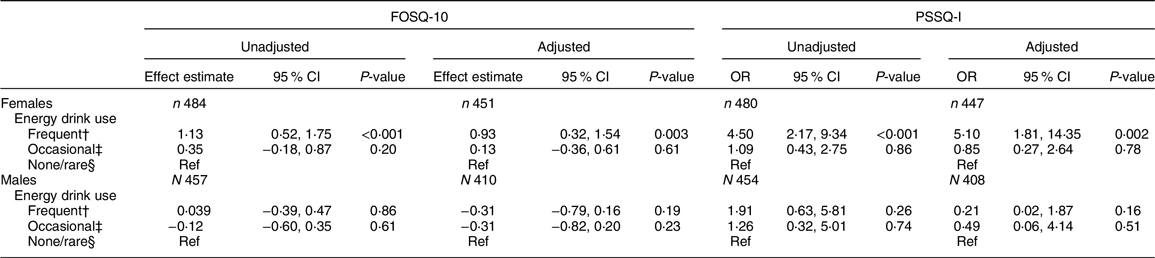
Table 2 presents the regression results of the association between ED use and FOSQ-10 scores and PSSQ-I scores (see online supplementary, Supplementary Table 2 for full multivariate model results). In females, frequent ED users (>1 week) had a significantly higher mean FOSQ-10 score than rare users (adjusted β = 0·93, 95 % CI 0·32, 1·54, P = 0·003), indicating a relatively impaired quality of life due to daytime sleepiness. There was also a significantly higher likelihood of insomnia in females as measured by PSSQ-I (Adjusted OR = 5·10, 95 %CI 1·81, 14·35, P = 0·002) for frequent ED users compared with rare users. In males, no significant effects were observed for the FOSQ-10 and PSSQ-I sleep outcomes.
Table 2 Regression results of the association between energy drink use and Fundamental Outcomes of Sleep Questionnaire (FOSQ-10) scores (linear regression), and Pittsburgh Sleep Symptoms Questionnaire–Insomnia (PSSQ – insomnia) scores (logistic regression)*
* Denominators show numbers for which data were available.
† ≥once/week.
‡ >once/month to <once/week.
§ ≤once/month.
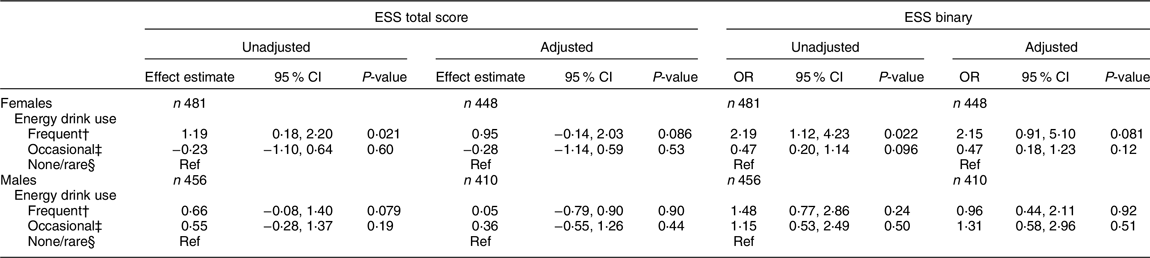
Table 3 presents the regression results of the association between ED use and ESS total scores and ESS binary scores (see online supplementary, Supplementary Table 3 for full multivariate model results). In females, there was a statistically significant increased likelihood of excessive sleepiness as measured by the ESS Total score (β = 1·19, 95 % CI 0·18, 2·20, P = 0·021) and ESS Binary score (OR = 2·15, 95 % CI 0·91, 5·10, P = 0·081) in unadjusted models for frequent users compared with never or rare users. However, the significance of these associations attenuated once confounding variables were adjusted for (both P > 0·05). In males, no significant effects were observed for the ESS total and binary score outcome variables.
Table 3 Regression results of the association between energy drink use and Epworth Sleepiness Scale (ESS) total scores (linear regression) and ESS binary (logistic regression)*
* Denominators show numbers for which data were available.
† ≥once/week.
‡ >once/month to <once/week.
§ ≤once/month.
Discussion
This study investigated the association between ED use and sleep disturbances in a population-based sample of young adult males and females from the Raine Study. Overall, there was a positive association between ED use and sleep disturbances in young adult females, but not young adult males.
These findings are consistent with several international studies on college students which have reported positive associations between ED use and poorer sleep quality, longer sleep latency, shorter sleep duration, lower habitual sleep efficiency and presence of insomnia. For example, in a recent study involving 919 college students from the United Arab Emirates, ED users were more than twice as likely to report poor sleep quality compared with non-users(Reference Faris, Jahrami and Al-Hilali37). Among US college athletes, Stasio et al. found frequent ED use to be associated with poorer sleep quality, longer sleep latency, shorter sleep duration and lower habitual sleep efficiency(Reference Stasio, Wagener and Glassman36). Similarly, in Velez et al.’s study involving 832 Chilean college students, where poor sleep quality was already prevalent, ED intake was associated with greater odds of poor sleep quality(Reference Vélez, Traslaviña and Barbosa39). In Thailand, ED use was shown to be significantly and positively associated with poor sleep quality (OR 1·50; 95 % CI 1·28, 1·77) in a large sample of college students (n 2854)(Reference Lohsoonthorn, Casillas and Lertmaharit20). Similarly, in a study involving 2458 Peruvian college students, ED use was identified as risk factor for poor sleep quality(Reference Sanchez, Martinez and Oriol40), with insomnia being the most frequently reported adverse effect of ED use in females (while it was increased urination in males)(Reference Alsunni and Badar38). To date, only one other population-based study has investigated the relationship between ED use and sleep disturbances in young adults. Our findings are in support of this study which found ED use to be associated with an increased risk in young adults of trouble going to, or staying, asleep(Reference Larson, Laska and Story44).
There are a number of possible explanations for the positive relationship between ED use and sleep disturbances. ED contain caffeine, an adenosine receptor antagonist, which has action blocking receptors in the brain that help regulate sleep and alertness(Reference Roehrs and Roth56,Reference Wikoff, Welsh and Henderson57) . Numerous studies have shown caffeine intake to disrupt sleep(Reference Lloret-Linares, Lafuente-Lafuente and Chassany21,Reference Wikoff, Welsh and Henderson57–Reference Salinero, Abian-Vicen and Gonzalez-Millán59) . Other ED ingredients such as sugar, Na, B vitamins, amino acids, colourings, flavourings and herbal stimulants may also act synergistically with caffeine to enhance its stimulatory effects(26–Reference Finnegan28). It is also possible that individuals experiencing sleep disturbances turn to ED for temporary relief of daytime sleepiness symptoms. Indeed, two-thirds of regular ED users in a study of 496 US college students cited an inadequate amount of sleep as the most common reason for ED intake(Reference Malinauskas, Aeby and Overton60).
Alternatively, it is possible that the relationship between ED and sleep disturbances is bidirectional. A cyclical pattern may exist whereby ED might be used to counter daytime sleepiness; however, the ED then cause sleep disruption, resulting in poor functioning and more daytime sleepiness which perpetuates the cycle of ED intake(Reference Juliano and Griffiths61–Reference Al-Shaar, Vercammen and Lu63). Evidence that ED may initiate sleep disturbances has been reported in a study which surveyed 667 first year US college students for up to 56 d each across four semesters yielding information on 25 616 person-days. On days when students used ED, they reported lower sleep quantity and quality that night, and greater next-day tiredness, compared with days of non-ED usage.
The current study found evidence of sex differences in the relationship between ED use and sleep disturbances. In young adult females (but not males), frequent ED users experienced significantly reduced functional status resulting from drowsiness as measured by the FOSQ-10 score and a significantly higher likelihood of insomnia as measured by the PSSQ-I, compared with none/rare users of ED. In females, a significant association with ED intake was found for the FOSQ-10 but not the ESS. This may be related to the fact they are measuring different constructs: daytime sleepiness in the case of the ESS and the effect of daytime sleepiness on functional outcomes related to daily behaviours and sleep-related quality of life. The reasons underlying the lack of association between ED use and sleep disturbances in young adult males are unclear. It may be related to potential differences in caffeine metabolism between males and females, including the influences of sex hormones(Reference Temple and Ziegler64) or differences in body fat and body weight(Reference Nawrot, Jordan and Eastwood65). Few other studies have examined differences between the sexes in the relationship between ED use and sleep disturbances, and those that have report mixed findings. For example, among members of the US military services (n 183, 81 % males, median age 27), Waits et al. did not find ED intake to be associated with insomnia in either sex(Reference Waits, Ganz and Schillreff66). However, this result may reflect the small sample of females in this study and the different context and setting within which the ED were used (i.e. during active service). Larson et al.’s larger population-based study found both sexes had trouble falling or staying asleep after ED consumption, while only males had perceived inadequate sleep(Reference Larson, Laska and Story44).
Given that the current study, and others, has linked ED use to sleep disturbances, it is important that there is more research in this relatively new and growing area. Future research could also employ more robust measures of sleep disturbances, such as using objective measures including actigraphy and polysomnography and try to elucidate whether it is the frequency or the amount of consumption, the type of ED, the individual or the combination of components that have the greatest impact on sleep disturbances. Finally, future research should incorporate longitudinal study designs as these types of study designs are needed to be able to draw conclusions regarding the causal relationships in question.
The present findings have important implications for policymakers, educators, health professionals and the general public. Intervention strategies to curb ED use in young adults, particularly females may be needed including more education to inform young people about the ingredients and potential harms associated with ED use, including their potential role in initiating and exacerbating sleep disturbances. Health promotion programmes should promote alternative ways to increase daytime energy levels among young adults such as getting adequate sleep, eating a nutritious diet and engaging in regular physical activity. Practicing clinicians may wish to assess ED intake in routine evaluations, particularly for young females presenting with insomnia and excessive daytime sleepiness symptoms. Finally, health professionals, parents and peers should be aware of ED use as a possible marker for sleep disturbances in young people, especially young adult females.
The findings of the current study should be interpreted in light of several limitations. As ED data were not collected in any earlier Raine cohort follow-ups, this study was limited by its cross-sectional study design which restricts the ability to derive causation. Self-reported use of ED, alcohol and illicit drugs were also relied upon. Whilst self-report assessment has been established as a valid means for assessing these behaviours and may lead to more honest reporting than face-to-face assessment(Reference Del Boca and Darkes67), the possibility of individual over- or under-reporting cannot be discounted. Not all confounding variables relating to sleep were able to be adjusted for in modelling, for example, medication use which might interfere with sleep was not able to be controlled for, nor was night-time screen use, which has been associated with sleep disturbances and insufficient sleep duration(Reference Hansen, Capener and Daly2,68) . This issue may be particularly relevant to this age group given 75 % of young adults (18–24 years) in the 2016 Australian Sleep Health Survey reported using the internet just prior to their bedtime on most nights(Reference Adams, Appleton and Taylor1). Whilst it was a strength of this study to use a large population-based sample, care needs to be taken in generalising these results to the wider community as participants included in the Gen2-22 years follow-up of the Raine Study were more likely to be socio-economically advantaged relative to participants lost to follow-up(Reference Straker, Mountain and Jacques46). Replication of our results in other cohorts would help address this concern. Despite these limitations, the results from this study provide important information regarding the association between ED use and sleep disturbances among young adults, highlighting the presence of a relationship in females but not males.
Conclusion
This study found a positive association between ED use and sleep disturbances in young adult females, but no associations were observed in young adult males. Given the importance of sleep for health and well-being, and the rise in ED use, further research is needed to establish causality and the possible mechanisms behind this relationship between ED intake and sleep disturbances in young adult females and intervention strategies to curb ED use in young adults.
Acknowledgements
Acknowledgements: The authors would like to acknowledge the Raine Study participants for their ongoing participation in the study, the Raine Study Team for study co-ordination and data collection, the UWA Centre for Sleep Science in the School of Human Sciences for utilisation of the facility and the Sleep Study Technicians. The authors would like to acknowledge the University of Western Australia (UWA), Curtin University, the Raine Medical Research Foundation, the UWA Faculty of Medicine, Dentistry and Health Sciences, the Telethon Kids Institute, the Women and Infants Research Foundation (King Edward Memorial Hospital), Edith Cowan University, Murdoch University, and the University of Notre Dame for providing funding for the Core Management of the Raine Study. The Gen2-22 years Raine Study follow-up was funded by NHMRC project grants 1021855, 1021858, 1027449 and 1044840. The current study was funded by the Western Australian Health Promotion Foundation (Healthway). Financial support: The current study was funded by the Western Australian Health Promotion Foundation (Healthway). Gina Trapp is supported by a NHMRC Early Career Research Fellowship (ID1073233). Peter Eastwood is supported by a NHMRC Senior Research Fellowship (No. 1136548). Hayley Christian is supported by an Australian National Heart Foundation Future Leader Fellowship (#100794). No funding body had any role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: All authors contributed to the conceptual design of the research. P.J. conducted the data analysis and all authors contributed to the interpretation of results. G.S.A.T. and M.H. drafted the manuscript. All authors critically revised the article for important intellectual content and approved the final version to be published. Ethics of human subject participation:. Data from the Raine Study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the Human Research Ethics Committees at the University of Western Australia (RA/4/1/5202) and Curtin University (HR67/2013). Written informed consent was obtained from all participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020001652.





