



Introduction
Because genetics is a relatively new and fast-moving field, there is often a severe imbalance of knowledge between patient and clinician. Knowledge imbalance generally serves professional interests (Abbott Reference Abbott1988: 102–8; Adler et al. Reference Adler, Seok-Woo and Heckscher2008: 363–5; but contrast Reed Reference Reed1996: 591). Given Michel Foucault’s (Reference Foucault and Gordon1980, Reference Foucault and Sheridan1995 [1975]) arguments on the fusion of power and knowledge in the contemporary bureaucratic-disciplinary-surveillance period, this knowledge exclusivity might give a genetic counselor exceptionally high autonomy in patient interactions. But I will show this is not the case. Instead, in genetic counseling, cultural expectations constrain clinical practice despite a vast imbalance of knowledge between clinician and patient.
Culture saturates medicine (Stein Reference Stein2018 [1990]), such that treatment decisions are at least partly culturally determined rather than taken on purely scientific grounds (Payer Reference Payer1988; Stein Reference Stein2018 [1990]). It is now a widespread view in social science that broader social values and political disputes over moral issues shape scientific norms, both for practicing medicine and for conducting scientific research (Fujimura Reference Fujimura2006; Harding Reference Harding, Essed, Theo Goldberg and Kobayashi2009; Fujimura and Rajagopalan Reference Fujimura and Rajagopalan2011; Kuhn Reference Kuhn2012 [1962]: esp. 94; Latour and Woolgar Reference Latour and Woolgar1986 [1979]; Latour Reference Latour1999: esp. 236–43). A long list of variations in clinical practice have been attributed to these sorts of cultural conditions, for example the use of psychotropic medication (Hoebert et al. Reference Hoebert, Mantel-Teeuwisse, Leufkens and van Dijk2017), increasing fibromyalgia and chronic fatigue syndrome diagnoses (Aho Reference Aho2018), placebo effects (Ongaro and Ward Reference Ongaro and Ward2017), and of course abortion (Kimport Reference Kimport2022: chap. 4), to name a few. Such cultural influences would be particularly strong where clinicians confront morally laden situations, such as genetic counseling around reproductive decisions. Indeed, bioethical attitudes vary so widely across cultures that the same intervention can be mandatory in one country and prohibited in another. I show below that this is the case for genetic counseling. For reasons elaborated in the methods section, the mid-1990s were an opportune historical moment to observe these medico-social dynamics.
Why should there have been considerable variation in genetic couseling practices across societies? One theoretically possible explanation is variation in formal institutional regulation, especially from professional associations, accreditation bodies, or government agencies. However, professional associations that could regulate genetic counseling were rare internationally. In the mid-1990s, only the United States, Canada, United Kingdom, and Australia had formally established standards of practice (Begleiter Reference Begleiter2002: 558–60). Meanwhile, direct government regulation appeared to be rare aside from China and India. Thus variation in genetic counseling practices are unlikely to result from formal institutional controls. Likewise, differential scientific knowledge does not explain the variation reported below, because scientific paradigms in genetics were similar across the medical systems of these 36 countries. Rather than scientific knowledge or regulation, the most promising explanation is cultural.
But which cultural mechanisms? Virtually all studies of genetic counseling note a likely relationship between counseling and abortion attitudes, but do not systematically investigate it (e.g., Bosk Reference Bosk1992; Rothman Reference Rothman1993 [1986]; Carnevale et al. Reference Carnevale, Lisker, Villa and Armendares1998; Rapp Reference Rapp1999; Browner 2006; Williams Reference Williams2006; Hashiloni-Dolev Reference Hashiloni-Dolev2007; Pilnick Reference Pilnick2008; Samerski Reference Samerski2009; Karlberg Reference Karlberg, Jean Moore and Kosut2010; Raz Reference Raz2010; Pilnick and Zayts Reference Pilnick and Zayts2014). This study fills that gap by demonstrating a strong link between abortion attitudes and counseling practices across 36 countries. Identifying abortion attitudes as a cultural mechanism affecting genetic counseling practice is a contribution to the history of medical professions, the development of applied ethics in clinical genetics, and the global history of abortion.
Given the same scientific information, genetic counselors facing the same sorts of cases practiced in opposite ways. This cross-national variation in genetic counseling correlated not with the medical characteristics of patients, but with national abortion attitudes. Specifically, in the mid-1990s, the level of directiveness in genetic counseling corresponded to prevailing abortion attitudes across societies. The less social and political controversy over abortion within a society, the more directive genetic counselors in that society were willing to be, regardless of whether the prevailing view was pro-restriction or pro-liberalization. The more social and political controversy over abortion, the less directive genetic counselors were willing to be.
Background
The genetic counseling profession
Genetic counseling is the explanation of personalized genetic information. Typical counseling sessions either consider whether to have genetic testing or explain the results of tests after they are conducted. Topics include the probability of having a genetic condition, how particular conditions affect daily life, and what treatments may exist. Since these conversations can be intense, genetic counselors are usually trained in a combination of medical science and emotional counseling (Marks Reference Marks, Bartels, LeRoy and Caplan1993: 19–20; Resta Reference Resta2006).
Since prenatal genetic testing implies the possibility of abortion, genetic counselors routinely deal with politically and religiously controversial issues. To be clear, abortion is a not the sole factor shaping counseling practices, even if it has considerable influence, and genetic counseling covers more than abortion-related topics. There are many reproductive concerns other than whether to terminate a pregnancy, such as whether and how to become pregnant in the first place. Prenatal and reproductive screening together still constitute the largest area of genetic counseling practice, ahead of oncology (National Society of Genetic Counselors 2021: 8).
The task of genetic counseling exists in all modern medical systems, but countries vary in how and whether they organize it. The relevant professionals may be physician geneticists, pediatricians, midwives, specialized nurses, or some combination. In the United States, master’s-prepared genetic counselors have their own professional association and board certification. With the apparatus of a clinical profession, they have collective interests to protect and advance.
The practice of genetic counseling mixes relatively low-tech methods, like pedigrees and family histories, with relatively high-tech methods, like comparative-genomic hybridization micro-array testing. (Medical technologists carry out the mechanics of the test; the genetic counselor interprets the results.) In recent years, new technologies of exome sequencing, whole genome sequencing, and genome-wide association studies have dramatically increased the clinical applicability of genetic testing and the quantity and comprehensiveness of information generated.
This is not a history of genetic counseling. While practitioners publish especially in the American Journal of Human Genetics and the Journal of Genetic Counseling, there is still relatively little social science of this medical field, possibly because genetics has only recently begun to fundamentally re-shape mainstream medicine. As pharmacogenetics, personalized medicine, and other genetic applications progressively take over medical practice, interest is sure to grow. Previous research on genetic counseling emphasizes its emotional impact on patients and clinicians alike (Bosk Reference Bosk1992; Rothman Reference Rothman1993 [1986]). Ethical consternation regarding the counselor–patient relationship is nearly omnipresent, underscoring its intense moral implications (Rapp Reference Rapp1999; Browner 2006; Pilnick Reference Pilnick2008; Samerski Reference Samerski2009; Karlberg Reference Karlberg, Jean Moore and Kosut2010: 53–61, 93–8). One study examines gender dynamics of this majority-female profession (Kenen Reference Kenen1984), and another the intersection of genetic counseling with public health programming (Senier et al. Reference Senier, Kearney and Orne2015). International comparisons on a smaller scale than this article found divergence in the practice of directiveness across countries, though consistency in the perceived moral implications (Carnevale et al. Reference Carnevale, Lisker, Villa and Armendares1998: 430; Hashiloni-Dolev Reference Hashiloni-Dolev2007; Raz Reference Raz2010; Pilnick and Zayts Reference Pilnick and Zayts2014). Those moral implications often manifest in debates about directiveness.
Non-directiveness
A non-directive ethical code eschews advice beyond factual information on the belief that patients should autonomously decide what to do without influence from the counselor’s values (Reed Reference Reed1980 [1955]; West Reference West1988: 195; Fine Reference Fine, Bartels, LeRoy and Caplan1993: 107–8; Timmermans and Buchbinder Reference Timmermans and Buchbinder2013: 15). As of the mid-1990s, when the survey used in this article was conducted, 96 percent of United States genetic counselors considered non-directiveness “very important” to their work (Bartels Reference Bartels1997: 172). However, some Italian counselors argued that strict non-directiveness is impossible in practice (Pennacchini and Pensieri Reference Pennacchini and Pensieri2011: 141), some German counselors continued to practice directively within a nominally non-directive standard (Cottebrune Reference Cottebrune2019), and some United States practitioners admitted that, faced with a debilitating condition like Huntington’s chorea, they could not bring themselves to remain non-directive (LeRoy Reference LeRoy, Bartels, LeRoy and Caplan1993: 53). Such confessions still acknowledged non-directiveness as the standard. When research found even a few United States counselors failing to uniformly practice non-directiveness, reactions suggested anxiety and defensiveness (e.g., Bernhardt Reference Bernhardt1997: 18–9; Kessler Reference Kessler1997: 466–7). In interview studies in the United States, the non-directive compulsion to encourage patient autonomy came through strongly (Markens Reference Markens2013: 440–5; Morrison Reference Morrison, Rothman, Armstrong and Tiger2008: 187–95).
Current official United States and Canadian guidelines accord with non-directiveness by emphasizing patient autonomy (Canadian Association of Genetic Counselors 2006: 1; National Society of Genetic Counselors 2017: 2.4), and alternatives remain marginalized (e.g., Gervas Reference Gervas, Bartels, LeRoy and Caplan1993: 130; Rehmann-Sutter Reference Rehmann-Sutter2009: 113). Across countries, however, counseling practices varied enormously over time. The purpose of this article is to understand how and why abortion attitudes may be driving this variation.
Hypotheses
Four hypotheses are tested pertaining to the relationship between international variation in genetic counseling practices and abortion attitudes. Terminology pertaining to abortion attitudes is defined below. If genetic counselors routinely advised clients to have abortions in a society without broad social consensus on the legitimacy of abortion, they would risk a dramatic downturn in their professional status. Their medical legitimacy would likewise suffer if they explicitly encouraged clients to avoid abortion. Hence hypotheses 1 and 2:
-
1. Where abortion is polarized, non-directiveness is the dominant genetic counseling practice.
-
2. Where abortion is contested but not polarized, non-directive genetic counseling is prevalent, but less dominant than in polarized societies.
However, in a society where abortion was not controversial, prenatal genetic counselors might behave differently. In a society where abortion is anathema, it would be uncontroversial to counsel directively against abortion. Conversely, in a society where abortion is widely accepted, it would be uncontroversial to advise a patient in certain situations to have an abortion. Hence hypotheses 3 and 4:
-
1. Where abortion is broadly rejected, genetic counselors will practice directive counseling in the form of advising patients not to have abortions more than in societies where abortion is controversial or polarized.
-
2. Where abortion is broadly accepted, genetic counselors will practice directive counseling in the form of advising patients to have abortions more than in societies where abortion is controversial or polarized.
Data and methods
Genetic counseling data
This article is as a historically informed sociological investigation of how genetic counseling norms vary across societies. It is not meant as a report on the current situation. The theoretical interest of this study is the effect of culture, in its global variation, on medical practice. A historically informed approach is appropriate because the present moment is not necessarily the best time to observe maximum variation. Rather, the earliest moment that global cross-cultural comparability is possible occurs once a medical technology is established on every inhabited continent. This historical moment comes after a professionalizable medical activity has spread itself globally, but before any global norm within that profession has been firmly established. Investigating at this moment thus minimizes the effects of any trans-national professional norms that could later develop and maximizes the potential to observe the effect of local cultural norms on professional practice. This approach best investigates the variation of interest here because it captures the cultural expectations of the country or region on the medical practice that occurs within that country or region. For genetic counseling, this analytically ripe moment came in the mid-1990s, after training programs had been established in Australia and South Africa, but while the profession was still relatively young in most of the world (Wertz and Fletcher Reference Wertz and Fletcher2004: 7).
Because social dynamics evolve, due to professionalization and many other reasons, proper cross-cultural comparability is only possible if all countries are studied at approximately the same time. Fortunately, earlier research struck at precisely the right moment. A mid-1990s international 36-country survey of prenatal genetic counselors is by far the most comprehensive study of counseling attitudes, covering all countries in which there were at least 10 practicing medical geneticists. In distributing this survey, local knowledge was essential because the institutional structure of the same medical activity varied widely across countries. One to four prominent medical geneticists from each country described their country’s population of genetic counseling practitioners (Wertz and Fletcher Reference Wertz and Fletcher2004: 307–16 reports their biographies). All identifiable practitioners received a mailed survey and up to two subsequent attempts to contact non-respondents (Wertz and Fletcher Reference Wertz and Fletcher2004: part 1).
The number of genetic counselors in a country varied with population, development of the medical system, and integration of genetics within that system. It bears repeating that these are different types of clinicians in different countries; the American para-profession model was only one of many configurations. Table 1 lists the 36 countries with response rates and numbers of respondents. A total of 2,906 responded, for an overall response rate of 63 percent (for descriptive statistics see Wertz and Fletcher Reference Wertz and Fletcher2004: 321–4). Median national response rate is also 63 percent.
Table 1. Countries sampled and response rate

Note. Total n = 2,906, response rate = 63%.
Source: Wertz and Fletcher (Reference Wertz and Fletcher2004: 321–4).
For nearly all countries, sample sizes were large relative to population, even when the absolute number appears deceptively small. For instance, the Greek sample of 12 constituted 100 percent of practicing genetic counselors in the country. This survey is by far the best available metric of how professional genetic counseling norms vary across societies.
Genetic counseling measurement
Each respondent was asked whether they would “provide unbiased counseling” for a variety of conditions, as opposed to either “give pessimistically slanted information” or “urge termination of pregnancy.” The former is non-directive and either or both of the latter two are directive toward abortion.
Analysis focuses on three conditions: Trisomy 21 (popularly known as Down syndrome), severe open spina bifida, and Huntington’s chorea. Each was incurable and untreatable at the time of the survey. Trisomy 21 causes mental disability and mild physical disability. The survey asked about “severe, open spina bifida,” which differs from surgically correctible forms of spina bifida (Rofail et al. Reference Rofail, Maguire, Kissner, Colligs and Abetz-Webb2014: 215). In severe open spina bifida, vertebrae do not form normally and a portion of the spine protrudes from the body causing nerve damage, varying degrees of paralysis, loss of sensation below the protrusion, and sometimes lower body deformities. Individuals with Huntington’s chorea have a normal childhood and young adulthood, but around age 35 cognitive abilities decline precipitously, physical infirmities set in, and they lose capacity for basic independent function.
Each of these conditions profoundly affects life, but in different ways. Trisomy 21 is primarily a mental disability with some physical consequences. Severe open spina bifida indirectly increases risk of cognitive impairment, but it is possible for any given individual to beat the odds and live into adulthood with normal cognitive function, though severely reduced bodily function. Huntington’s chorea onsets in adulthood, causing profound loss of cognitive and social function, and less profound physical consequences.
Selecting three conditions with distinct types of impact partially controls for the cultural salience that different types of disability may have. Note that none of these conditions are fatal. The decision of whether to abort a pregnancy affected by one of these genetic conditions thus pertains not to life or death but to life with disability.
Abortion attitudes data
An accurate assessment of prevailing national abortion attitudes is required to demonstrate their effect on genetic counseling practice. Unfortunately, there is no reliable and straightforward numerical measure of abortion attitudes. Frequency and intensity of political debate is relevant, but in some societies, politicians debate despite a strong consensus in the general population, e.g., Thailand (Florida Reference Florida and Keown1998: 25; Warakamin et al. Reference Warakamin, Boonthai and Tangcharoensathien2004: 150). Abortion law is a relevant but not always reliable indicator of prevailing attitudes for some of the same reasons, but also because similar statutes might be interpreted or implemented quite differently in different societies. Incidence is relevant, but people may have an abortion and still believe it is immoral; thus incidence may be high in strongly anti-abortion societies, e.g., Chile (Singh and Wulf Reference Singh and Wulf1994; Singh et al. Reference Singh, Henshaw, Bankole, Hass, Wulf, Hollander and Johnson1999: 23). Polls and surveys are particularly important, but must be interpreted with care because results can be highly sensitive to minor changes in question wording and sample construction. Polls are also less reliable in more authoritarian countries. The best method to assess national political culture on abortion is to consider all of these indicators holistically and in historical perspective.
Abortion attitudes analytic approach
Based on a comparative-historical investigation of policy, frequency and intensity of political debate, incidence rates, and polling data in all 36 countries, this study classifies abortion attitudes as broadly accepted, broadly rejected, contentious, polarized, or a fifth category of contentious politically but broadly accepted in the population. Abortion was ‘broadly accepted’ when a substantial majority of the population (usually approximately two-thirds or more) favored legal abortion under relatively broad circumstances (usually at least the first trimester with little or no justification), and there was no serious effort within the political arena to restrict the procedure. ‘Broadly rejected’ means a substantial majority of the population favored banning abortion except under narrow circumstances (usually genetic anomaly, rape, incest, or specifically defined threats to the mother’s health), and there was no serious effort within the political arena to liberalize the procedure.
‘Contentious’ means there was no substantial majority among the population on abortion policy, and the issue was at least somewhat politically active. ‘Polarized’ means the population was approximately evenly divided, and abortion debates were so fundamental that they affect the entire political arena. ‘Contentious politically, broadly accepted in population’ means a substantial majority of the population favored legal abortion under broad circumstances, but some faction continued to press the issue within the political arena. In no country with a divided population was the issue politically dormant.
Results
Directiveness in genetic counseling
Figure 1 reports the percentage of genetic counselors by country who said they would use non-directive counseling for a patient with a pregnancy affected by each condition. Countries are listed ascendingly from left to right by the mean percent of non-directiveness across all three conditions. The figure shows enormous international variation in genetic counseling practices. A fitted trendline would ascend diagonally left to right from zero to nearly 100. Almost no genetic counselors in China would use non-directive counseling, whereas only a small percentage of counselors in Canada would use directive counseling. In some countries, counselors were divided, suggesting no strong norm of non-directiveness and that directive counseling was often acceptable. The survey also asked the opposite question: whether genetic counselors would explicitly urge abortion or intentionally slant information to create pessimistic impressions. As expected, the answers to these two sets of questions were approximate inverses (data not shown).

Figure 1. Non-directiveness by Country for Three Serious Genetic Conditions.
It would require data more fine-grained than what is available to explain the intranational as well as international variation in Figure 1, but apparently genetic counselors in some countries were more sensitive to one of these conditions than the other two. In most countries, counselors were most directive for spina bifida, and least directive for Huntington’s chorea. Table 2 reports standard deviations within countries, listed in order of country directiveness. Across countries, standard deviations of genetic conditions were 26.6 for Trisomy 21, 21.7 for spina bifida, and 25.0 for Huntington’s chorea. As expected, standard deviations across countries were much higher than within countries. What is crucial for the present argument is that the general pattern of decreasing directiveness with increasing abortion controversy was strong for all three conditions.
Table 2. Means and standard deviations of non-directiveness across genetic conditions

Source: Author’s calculations.
Abortion attitudes
The key period for abortion attitudes was the early to mid-1990s because that is when the survey was conducted. Classification of national attitudes as of this period are presented in Table 3.Footnote 1 In four countries, abortion attitudes were polarized. In seven (all European) they were contentious. In nine mostly Latin American countries, abortion was broadly rejected. In 14 countries abortion was broadly accepted, and in four others it was broadly accepted in the general population but contentious politically. For reasons explained below, one country split into two regions, and one into two time periods.
Table 3. Classification of prevailing abortion views by country, 1990s
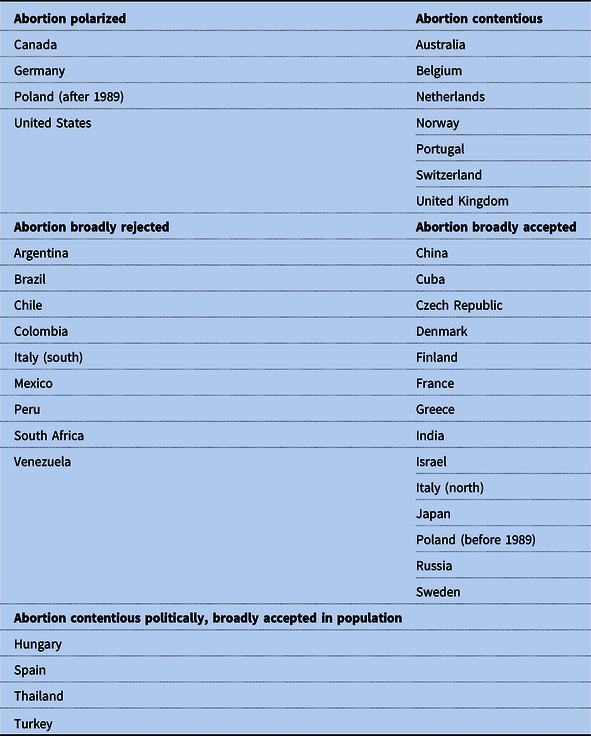
To demonstrate the classification procedure and show a sample of the background research, I review all countries superficially, then I more thoroughly review one country from each category.
In four countries, abortion attitudes were polarized. Canadian public opinion was evenly split, and parties avoided drudging up the issue in memory of the intensely divisive debates of the late 1980s (Halfmann Reference Halfmann2011: 207). In Germany, abortion complicated East-West reunification; a compromise law banned the procedure but suspended prosecution (Ferree Reference Ferree2012: 37–40, 62–6, 145–55). In the United States, the most enduringly polarized of all, the public split between emphasizing life in utero and emphasizing women’s reproductive choice, both sides using human rights discourses (Tribe Reference Tribe1992).Footnote 2 See below for Poland.
In seven countries, views were contentious. Belgium and Portugal are discussed briefly below. The Netherlands permissively implemented its moderately restrictive law, though 1990s surveys, which suffer from poor wording, suggested strong majorities against the procedure after intense parliamentary debates in the 1970s and 1980s (Ketting and Visser Reference Ketting and Visser1994: 162–4). In Norway, the procedure was established in the medical system but moderately contentious, as religious and conservative groups vocally protested it and substantial numbers of physicians refused to perform abortions (Løkeland Reference Løkeland2004: 167). In Switzerland, abortion was publicly stigmatized and remained illegal until 2002, but was rarely prosecuted (O’Dea Reference O’Dea2012). In the United Kingdom, abortion was technically illegal, but the law was interpreted so broadly and with so many exceptions that abortion was widely available in practice; half the country favored additional restriction in the mid-1990s (McVeigh Reference McVeigh2012). See below for Australia.
In nine mostly Latin American countries, abortion was broadly rejected. In the 1990s, abortion was only legal in extremely limited circumstances and public opinion overwhelmingly opposed broad legalization in Argentina (Beldon Russonello Reference Beldon Russonello2011: 12, but see below), Brazil (Pichonelli Reference Pichonelli2010), Mexico (Lerner and Salas 2013), Peru (Heimburger Reference Heimburger2008: 17–30), and Venezuela (Blanco Reference Blanco2011). In Chile (Singh et al. Reference Singh, Henshaw, Bankole, Hass, Wulf, Hollander and Johnson1999: 23) and Colombia (Moloney Reference Moloney2009: 534), abortion was banned in all circumstances. Although post-apartheid South Africa liberalized abortion, the procedure was widely stigmatized and hard to obtain, and surveys showed most of the population was not even aware of the legalization (Morroni et al. Reference Morroni, Myer and Tibazarwa2006: 2).
In Italy, abortion appeared controversial on an aggregate national basis, but within regions, consensus was rather high: most of the north was permissive toward abortion, while Sicily, Sardinia, and most of the south were restrictive. There was a marked regional split in public opinion, incidence, and rates of physician conscience objections (Bettarini and D’Andrea Reference Bettarini and D’Andrea1996: 270–1; see also Finchelstein Reference Finchelstein2005: 13). Medical practitioners are likely aware of both these realities—a high local consensus and the presence of national debate—but local consensus could be most relevant to the daily practice of genetic counseling.
In 14 countries abortion was broadly accepted. China was the only country in the sample with mandatory abortion. Under the one-child policy in effect in the 1990s, penalties for exceeding two children could be steep, even including forced abortion or forced sterilization (Greenhalgh and Winckler Reference Greenhalgh and Winckler2005: e.g., 42). In Denmark (Norup Reference Norup1997: 440, 443–4, see also below), France (Naour and Valenti Reference Naour and Valenti2003), and Sweden (Linders Reference Linders2004: 372), a period of national deliberation over abortion in the 1970s produced fairly broad consensus. In Finland, that debate happened earlier, with enduring results for popular opinion (Finchelstein Reference Finchelstein2005: 13). In Israel, abortion has never been prosecuted; it was broadly available and politically a non-issue (Eshet Reference Eshet2012). In Japan, abortion was legal and minimally controversial in a culture that prioritized a strong family unit (LaFleur Reference LaFleur and Keown1998). In some European countries like the Czech Republic (Rychtarikova Reference Rychtarikova1999: 20), Greece (Ioannidi-Kapolou Reference Ioannidi-Kapolou2004: 177–8), and Russia (Popov Reference Popov1993: 25), abortion was often seen as just another form of contraception. Roughly speaking, this also applied to Cuba (Bélanger and Flynn Reference Bélanger and Flynn2009: 15–24) and India (Visaria et al. Reference Visaria, Ramachandran, Ganatra, Kalyanwala, Visaria and Ramachandran2007: 3–13), though for different historical reasons in each case.
In four other countries, abortion was broadly accepted in the general population but contentious politically. See below for Hungary. Spain implemented its restrictive abortion laws permissively, and strong majorities favored abortion on demand since the 1980s despite political maneuvering around the issue (Valiente Reference Valiente and McBride Stetson2001: esp. 231–43). Turkish politicians routinely denounced abortion despite high rates of public acceptance (Igde et al. Reference Igde, Gul, Igde and Yalcin2008: 370–2). In Thailand, abortion was a standard option even in public hospitals, despite being technically illegal and vocally decried by some politicians (Warakamin et al. Reference Warakamin, Boonthai and Tangcharoensathien2004: 150).
Polarized example: Poland
From World War II to 1989, this heavily Catholic country was a satellite state of the Soviet Union allowing abortion almost without restriction (historical material draws primarily on Eberts Reference Eberts1998: 823–6; Kulczycki Reference Kulczycki1999: Chapter 4). Debate erupted after the first elections in 1989. The Catholic Church had been substantially forced underground during the period of Soviet domination. It now made banning abortion the core of its moral renewal program, and applied severe pressure to rightist politicians, who promptly restricted the procedure and considered an absolute ban. But in the absence of quality contraception, “abortion had become widely used for birth control purposes” (Kulczycki Reference Kulczycki1999: 112) and ingrained in the medical system. After four years of clashes in the National Assembly, rightist parties emerged victorious in 1993, banning abortion except in cases of rape, incest, fetal malformation, or a threat to the health of the mother that three physicians agreed was serious (Tatalovich Reference Tatalovich1997: 83). The next year, a far more permissive law to allow first-trimester abortion on demand passed the National Assembly, only to be vetoed by anti-abortion president Lech Walesa. In 1996, the assembly again passed an exemption for financial or personal difficulties, but it was struck down by the constitutional court on right to life grounds, leaving the 1993 law in force. In summary, after democratization, abortion law became highly restrictive, and the country polarized “with an intensity unimaginable before Poland entered systemic change” (Kulczycki Reference Kulczycki1999: 113).
Survey results vary, but on balance they suggested a divided population (e.g., Central Statistical Office 1991: 178–83, cited in Simon Reference Simon1998: 103–4; Kulczycki Reference Kulczycki1999: 124). An early 1990s survey conducted at the height of clerical power showed only 26 percent approved of abortion if a couple did not want more children, but this low approval may have been specific to lawfully married couples. The same survey found 74 percent approved of abortion in the event of fetal disability; results were consistent across demographic categories (Simon Reference Simon1998: 103–4).
All Polish genetic counselors practicing at the time of the survey were trained under the old, highly permissive system. As of the 1990s, public debate was quite a recent development. This probably makes the broad acceptance of the soviet era most relevant for the present study. Whether genetic counseling practice in Poland has since transformed is an area for further research. Absent other mitigating factors, I would expect more emphasis on non-directiveness in the 2020s than in the mid-1990s, particularly among younger genetic counselors trained after the political system polarized.Footnote 3
Example of ‘contentious’: Australia
Australian states regulated abortion; there was no binding federal policy. Abortion was illegal and sometimes actively prosecuted until the late 1960s or early 1970s, when states adopted different rules about the conditions under which it would be allowed (Coleman Reference Coleman1988). Some statutes were ambiguous and most abortions may have been technically illegal, but as a practical matter, having an abortion early in a pregnancy brought no criminal consequences. This arrangement was partially disrupted in 1998, when two doctors were arrested in Western Australia for providing abortions. The Western Australian Parliament initially deadlocked, then passed a relatively liberal law allowing abortions (O’Connor et al. Reference O’Connor, Orloff and Shaver1999: 164). Abortion polling over decades suggested a steady increase in public support for legal abortion; as of 1995 support was at 55 percent (Betts Reference Betts2004: 23). Some politicians remained outspoken on both sides (Griffiths Reference Griffiths2013). Abortion was at least somewhat contentious in Australia, but not polarizing to the extent of fundamentally shaping the contours of politics.
Example of ‘broadly rejected’: Argentina
At the time of the survey, and for years after, abortion was illegal in Argentina except in rare cases. Sometimes even when the procedure was legally permitted, no licensed doctor could be found willing to do the abortion (Human Rights Watch 2005: 48–50). The procedure was formally banned in 1921, punishable by lengthy incarceration. From 1974 to 1987, it was illegal even to tell a patient about basic contraception (Rogers Reference Rogers1994; cf. Human Rights Watch 2005: 26–30). Strong statements against abortion were customary among top officials until at least the early 2000s.
Pro-liberalization agitation remained marginal until long after this survey was conducted. It was after 2005 when an abortion liberalization movement cohered, and it took many years to shift politics on the issue (Sutton and Borland Reference Sutton and Borland2019). According to a 2011 survey financed by a pro-liberalization organization, only 13 percent of Argentinians believed abortion should be legal in “most cases,” although support was much higher when the woman’s life was in danger (Beldon Russonello Reference Beldon Russonello2011: 12). A liberalization bill failed in 2018, then passed in 2020, legalizing abortion on demand for the first 14 weeks of pregnancy. This may become a watershed for the region—time will tell. In any case, the Argentine social and political consensus was consistently anti-abortion into the 21st century.
Example of ‘broadly accepted’: Denmark
Abortion was illegal in Denmark until 1937, when a new law allowed women to request permission for abortion in cases of fetal genetic impairment, rape, or serious risk to the life or health of the mother (Folketing 1938). This law was adjusted in 1970 and overhauled in 1973, when first-trimester abortion became available without restriction (Hansen et al. Reference Hansen, MÆlgaard-Nielsen, Knudsen and Keiding2009: 648). Since then, abortion has not been an object of major political controversy. A 1995 national survey found that 85 percent supported the law and only about two percent opposed abortion in all cases (Norup Reference Norup1997: 440, 443–4). There is a high social consensus in Denmark supporting permissive abortion policies.
Example of ‘broadly accepted in population but contentious politically’: Hungary
In recent decades, including when the data for this study were gathered, abortion law and abortion attitudes in Hungary have been broadly permissive. But the longer-term political history is more complicated. Hungary has repeatedly legalized and banned the procedure since the early 20th century, despite consistently high public support for liberalization (David Reference David and David1999: 151–5). Hungary restricted abortion in the early 20th century as a means of increasing its population, then liberalized its laws in the 1950s. Restrictions were re-inserted in 1976, then substantially repealed in 1988 (Szalai Reference Szalai1988; David Reference David and David1999: 151–5). A 1992 law legalized any first-trimester abortion that created a “crisis situation” as defined by the woman; this meant abortion was formally restricted, but in practice broadly available (Batar Reference Batar1993: 17). This law is still in effect. Even after enacting a controversial new constitution in 2011 that sought to protect all life from the moment of conception, the rightist ruling party promised not to use this to restrict access to abortion, although some doubted their intentions (United Nations 2013: 8).
Throughout all the legislative back and forth, public attitudes remained consistently permissive. According to a 1990s survey, a large majority of the population—74 percent of the weighted sample—supported abortion on demand. The mean voter is in the 88th percentile supporting the pro-liberalization position (Kitschelt et al. Reference Kitschelt, Mansfeldova, Markowski and Toka1999: 331, 335). Even within the political parties where the elected politicians are divided on abortion law (the Christian Democratic People’s Party, the Independent Smallholders Party, and the Hungarian Democratic Forum), a majority of voters still favored abortion on demand (Kitschelt et al. Reference Kitschelt, Mansfeldova, Markowski and Toka1999: 318).
Surveys from the early 1980s and early 1990s—before and after the end of soviet political influence—return remarkably consistent overall results. Where a couple does not want more children, 69 percent in both periods approved of abortion (Simon Reference Simon1998: 107). Regarding genetic anomalies, about 91 percent in each period supported abortion if the child was likely to be disabled. These results are consistent across gender, religion, and marital status; the only attitudinal split was among those of low socioeconomic status (ibid.: 87, 108). Political transitions and disputes in Hungary are not affecting permissive attitudes.
Genetic counseling and abortion attitudes
Having classified abortion attitudes within the same set of countries that were surveyed in the mid-1990s, I now overlay these classifications onto the survey results and see whether any patterns that emerge are consistent with the hypotheses.
Figure 2 presents a quartile whisker plot showing the clusters that result when classification of abortion attitudes is combined with mean non-directiveness across countries. Directiveness per country is measured by the mean across the three conditions. Countries in which abortion is contentious are noticeably higher in non-directiveness than countries where it is not, and that countries in which abortion is polarized are higher still. These findings support hypothesis one, which stated that where abortion attitudes are polarized, non-directive counseling will predominate. A minimum of two-thirds of counselors practice non-directively in polarized countries, and in most the proportion is far larger.
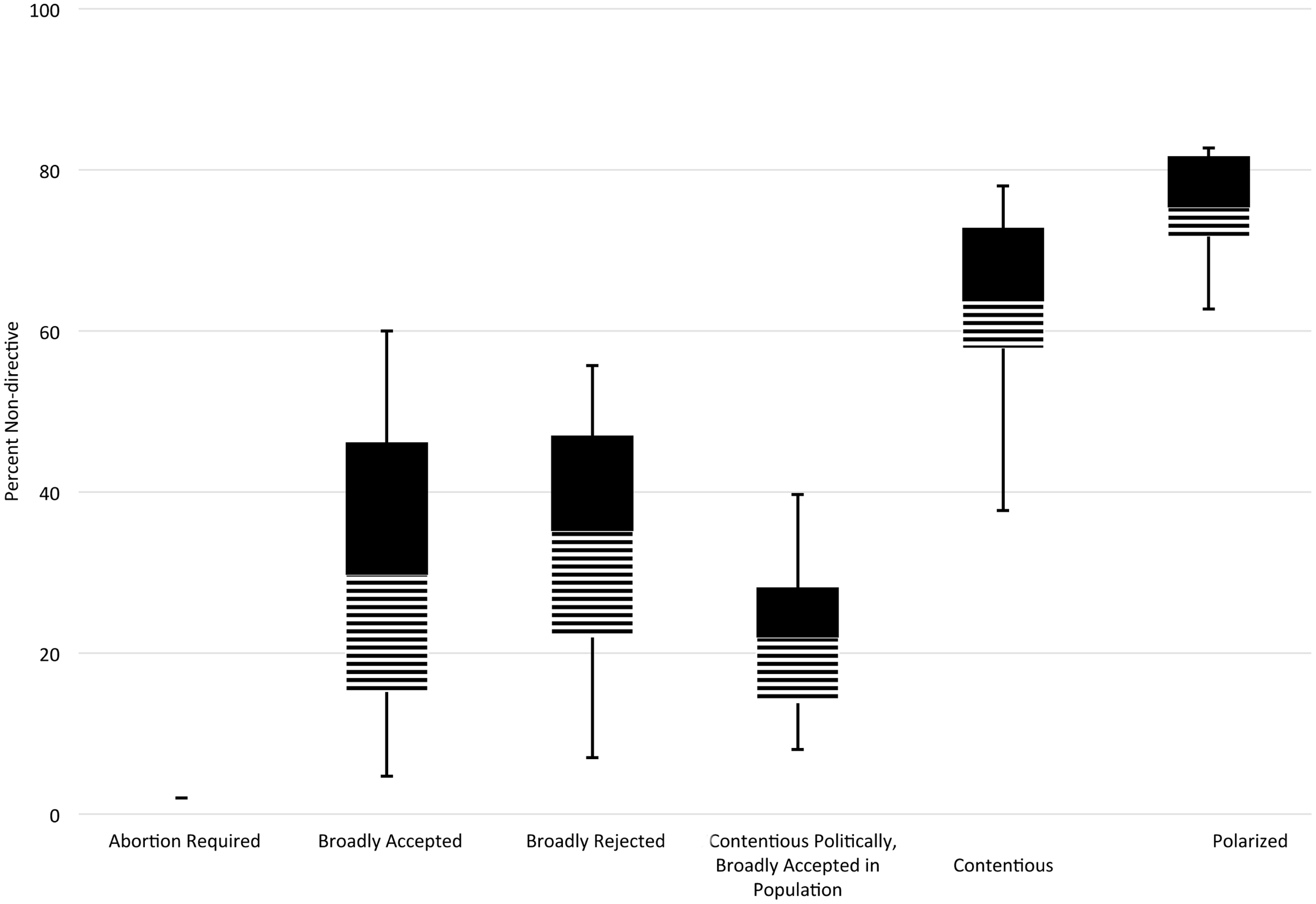
Figure 2. Quartile whisker plot of non-directiveness by abortion category.
Note: Within each cluster, lines extend from the minimum value to the 25th percentile and from the maximum value to the 75th percentile. Dashed bars extend from the 25th percentile to the mean and black bars from the 75th percentile to the mean. Dashed and black bars meet at the mean. Only in China is abortion frequently required. Poland and Italy are omitted; see the text.
These results also support hypotheses three and four, which stated that when abortion attitudes are not contentious, directive counseling will predominate. In the vast majority of countries where abortion was either accepted, rejected, or contentious politically but not in the general population, well over half of genetic counselors practiced directively. The partial overlap between the contentious cluster and the accepted and rejected clusters is due to the coarseness of these categories. Detailed examination of the countries at the extremes of their cluster—a sort of comparative-historical data scrubbing—reveals they are either the least or most contentious within their respective categories, which is consistent with the hypotheses.
The pattern appears clear, but statistical confirmation greatly increases confidence. I have sought this in two ways. I constructed a quantitative variable for abortion attitudes using a value of zero for broadly rejected, one for controversial but historically trending toward rejection, two for polarized or contentious without apparent historical trend, three for controversial trending toward acceptance, four for broadly accepted, and five for abortion required (which applies only to China). Using this simple abortion scoring reduces the role of my own interpretation of complex national cultures, but underestimates the finding. A more nuanced scale would produce even stronger results.
This scale is useful because it permits my classification of country-by-country abortion attitudes, reported above, to feature in a statistical model. But its simplicity also presents limitations. It assumes quantitative continuity in the way it plots abortion attitudes on the x-axis. That is, it assumes that the difference between a value of zero and a value of one is the same as the difference between a value of one and a value of two, and so on. Substantively, this requires the claim that the difference between ‘broad rejection of abortion’ and ‘contention that historically tends toward rejection’ is quantitatively equivalent to the difference between such contention and polarization. I do not believe this is the case. Public discourse in many of the contentious countries seems much closer to public discourse in the polarized countries than it does to countries with either widespread rejection or widespread acceptance. Fundamentally, the abortion classifications are qualitative, not numerical differences.
I thus performed two analyses: a polynomial least squares regression assuming a continuous x-axis for national abortion attitudes, and a simple t-test of a single population parameter that removes that assumption. As I have said, the continuous x-axis assumption is not fully empirically accurate. If the results of both analyses are consistent, confidence in the robustness of the finding is higher than if their results are inconsistent.
T-test results are reported in Table 4. The first line of Table 4 shows that counselors in countries that were polarized over abortion were more than 26 percent more likely to practice non-directively than counselors in countries that were not polarized over abortion. Equivalently, they were over 26 percent less likely to practice directively. As seen in Table 3, four countries in the sample were polarized over abortion and 32 were not. There are 1,626 survey respondents from polarized countries, and 1,280 from countries that were not polarized. In terms of number of respondents, sample sizes for the categories of polarized and not polarized are not radically unbalanced. This finding in the first line of Table 4 is highly significant, with a p value slightly over 0.01 on 36 observations.
Table 4. T-tests of relationship between abortion attitudes and genetic counseling directiveness

The second line of Table 4 reports a different comparison. It compares genetic counseling in countries where abortion was contentious or polarized to countries where abortion was broadly accepted or broadly rejected. The distinction here is between some discernible level of active contention in the public sphere over abortion (the categories of polarized and contentious) versus minimal discernible contention in the population (all other categories). The finding is that genetic counselors in countries with active contention over abortion were more than 17 percent more likely to practice non-directively than countries with minimal or no contention. Equivalently, they were over 17 percent less likely to practice directively. As seen in Table 3, 19 countries in the sample were contentious and 17 were not. There are 1,812 survey respondents from contentious countries and 1,096 from non-contentious countries, so the sample is not radically unbalanced between contentious and not contentious on both the number of countries and the number of respondents. This finding in the second line of Table 4 is highly significant, with a p value slightly over 0.01 on 36 observations.
These results include the odd cases of Italy and Poland, whose regional and temporal transformations were discussed above. Results are similar and remain highly significant when these two countries are omitted.
Now for the polynomial regression. To review once again, the hypotheses of this study are that level of directiveness correlates with level of abortion contestation. The trend line consistent with these hypotheses should resemble an inverted parabola, like an upside down U. Any shape pronouncedly different from this would be inconsistent with the hypotheses. Figure 3 presents a scatter plot locating all 36 countries by mean self-reported genetic counseling directiveness and abortion attitudes, using the one-to-five scale described above.

Figure 3. Non-directiveness plotted by abortion acceptance with unsmoothed trendline.
Note: >1 percent separates Argentina and Colombia.
The plot in Figure 3 includes an unsmoothed trendline derived from a second degree polynomial least squares regression on mean non-directiveness of all countries, treating abortion attitudes as a factor variable. The resulting inverted U-shaped curve is strongly consistent with the hypotheses. Separate regressions were run for each of the three conditions. Table 5 reports the results. Results were similar and significant without Italy and Poland, and separately when China was classified with the other broadly accepted countries. All models are highly significant with large effect sizes.
Table 5. Bivariate polynomial regressions of abortion attitudes on genetic counseling practice

Note: N = 36 for each model; N = 108 for likelihood ratio and Wald tests.
* p < .05;
** p < .01;
*** p < .001 (two-tailed tests).
I performed likelihood ratio tests for the curve of each of the three diseases. I also performed Wald tests for the curve of each of the three diseases. All likelihood ratio and Wald tests found that the shape of each disease-specific curve did not significantly differ from the others, showing the pattern of relationship to abortion attitudes is the same for all three conditions. The intercept term for the Huntington’s and Trisomy 21 curves did not significantly differ, but the spina bifida intercept did. This indicates what is already visible from Figure 1: level of directiveness for spina bifida is different, but the pattern of international variation is the same. Thus findings from t-tests, polynomial regression, likelihood ratio tests, and Wald tests all support the hypotheses of the study. The more controversial abortion was within a society, the less directive genetic counselors were willing to be, whereas the less controversial abortion was, the more directive the counseling.
Complications and limitations
Strictly speaking, this analysis demonstrates only that countries without abortion controversy used directive counseling, not whether that counseling was for or against abortion. However, since the survey shows that they counseled directively, it would be extremely surprising if clinicians in countries where abortion was legal and widely accepted counseled directively against it. Likewise, it would be surprising if genetic counselors recommended abortions in countries where abortion was uncontroversially banned. The classification of abortion attitudes pertains to the general population of the country, not to the counselors themselves, whose private views may not have accorded with those that prevailed in the culture in which they practiced.
Relatedly, it is worth noting that directiveness corresponded to abortion attitudes, not to abortion’s legality. If directiveness had corresponded to legality, then one plausible interpretation would be that counselors wished to save their patients from entanglements with the criminal justice system, or were motivated by obedience to the law. But the data are far more nuanced. Levels of directiveness were about the same in Japan, where abortion was broadly legal, and in Argentina, where it was almost totally banned. Directiveness varied widely even across societies where abortion was legal. For instance, abortion was legal in the two more non-directive countries and the two most directive countries (see Figure 1).
Another factor that could potentially influence directiveness is which sub-populations receive genetic services. Sub-populations may be subject to discriminatory, eugenic, or other attitudes in ways advantageous or disadvantageous toward them. While it is too simple to attribute the findings below to eugenic histories, it is likewise too simple to rule out that historical influence. Although practitioners usually disclaim any connection to historical eugenics, some historians see medical genetics as the product of a continuous development from earlier eugenic initiatives (Kevles Reference Kevles1995;; Bashford Reference Bashford, Bashford and Levine2010: 541–2; Stern Reference Stern2012). After all, “Active selection is everywhere in reprogenetics” (Bashford Reference Bashford, Bashford and Levine2010: 551). Some assail genetic testing (not necessarily counseling) as frankly “eugenic” with an agenda of preventing disabled births (Tankard Reist Reference Tankard Reist2006: esp. 3–10). An historian has found that “references to disability saturated the abortion debates of the 1960s–70s” (Herzog Reference Herzog2018: 16). Some continue to defend selective abortion and genetic interventions for eugenic goals (Singer Reference Singer2011; Savulescu and Singer 2021).
Whether some, none, or all of genetic counseling is eugenic depends, of course, on the definition of “eugenics” which often varies. Broadly though, the option of abortion presents a clear relationship between genetic testing and selective birth: “Arguably the most overlooked trajectory of eugenics lies in its connection to the liberalization of abortion law” (Bashford Reference Bashford, Bashford and Levine2010: 546). Studies of eugenic history generally focus on Europe and North America (e.g., Kevles Reference Kevles1995; Takard Reist Reference Resta2006; Stern Reference Stern2012; Herzog Reference Herzog2018; the collection in Bashford and Levine Reference Bashford and Levine2010 is an exception). Since the Euro-American experience does not necessarily generalize globally, it is especially intriguing to observe a fairly consistent global pattern in any behavior pertaining to eugenics and disability. The findings of this study constitute such an observation.
Having demonstrated an influence of abortion attitudes on medical practice, this study does not specify which cultural factors are or are not responsible for variations in abortion attitudes. I suspect it is not the same set of causes across all countries. There is no broad consensus on whether the explanation is diverging ideas of gender and motherhood (see Luker Reference Luker1985) or diverging political conditions (see Halfmann Reference Halfmann2011; Ferree Reference Ferree2012), among other possibilities.
Factors conceivably distorting results include low response rate in a few countries, reliance on self-reporting, and cross-national influences on the medical system. However, low response rate is probably not distorting overall results; the rate was below 40 percent in only four of 36 countries, and below 30 percent in only one. In any case, this is by far the best data available. Self-reports may differ from what a counselor does when faced with an actual patient. But if social desirability is biasing the results, it biases them toward the norm either of that country’s genetic counseling profession, or toward what the respondent believes American researchers prefer to hear. The former is precisely the data desired, and the latter biases toward non-directiveness, so the survey results represent a lower bound for directiveness and do not distort the general pattern.
Cross-national influence poses complications. Many genetic counselors practicing in one country may have been trained in another, or their domestic training programs may be closely modeled on those of another country. Abortion attitudes in the country that developed the training model would then interact through that training with abortion attitudes in the country where the counselors practice. This may be why Japanese genetic counselors were not even more directive than observed; their training was modeled on the United States.
As additional support for this interaction view, one might compare Australia and South Africa, two former British colonies where genetic counseling training followed the British model. Abortion was contentious in both the United Kingdom and Australia, and as expected, genetic counseling in both countries was non-directive. But South Africa, a culturally anti-abortion country, ranked near the middle of the non-directiveness spectrum.
Since the data come from the 1990s, any generalization past this period is speculative. My argument would predict that changes in genetic counseling would match any lasting cultural changes in abortion attitudes. There may be a lag as genetic counselors trained under a particular model age out of practicing. Beyond abortion, hypotheses based on this argument would be that genetic counselors do not counsel for what is culturally undesirable or contentious, and do counsel for what is culturally desirable or not contentious. For instance, prophylactic mastectomy has emerged in recent years as a procedure prompted by genetic counseling. In the absence of cultural or political resistance to this procedure, or perhaps any procedure, counselors could directively suggest it. Were a substantial and sustained movement to emerge against a procedure, counselors would shift to presenting the option neutrally if at all, but if the procedure were culturally taboo they would directively counsel against it. This is what to expect if the findings of this study are generalizable.
Conclusion
This article finds that clinicians in different societies, using the same scientific knowledge, employed virtually opposite approaches to medical practice. In genetic counseling, clinicians can be non-directive either by offering only scientific facts, or they can be directive by offering their opinion on what the patient should do or by deliberately slanting information intending to lead the patient to a particular conclusion. While there is often consensus within a country on which approach is best (e.g., Canadian Association of Genetic Counselors 2006; Morrison Reference Morrison, Rothman, Armstrong and Tiger2008; Markens Reference Markens2013; National Society of Genetic Counselors 2017), there has not historically been a global consensus (see LeRoy 2011; Pennacchini and Pensieri Reference Pennacchini and Pensieri2011; Cottebrune Reference Cottebrune2019).
Since genetic counseling is often sought prenatally, many have questioned whether abortion attitudes might influence its directiveness or lack thereof (e.g., Bosk Reference Bosk1992; Rothman Reference Rothman1993 [1986]; Rapp Reference Rapp1999; Browner 2006; Samerski Reference Samerski2009; Karlberg Reference Karlberg, Jean Moore and Kosut2010; Raz Reference Raz2010; Pilnick and Zayts Reference Pilnick and Zayts2014). This influence has never been empirically demonstrated with systematic data. A 36-country global survey, fortuitously timed for the mid-1990s after genetic counseling was established on every continent but before any strong trans-national norms, provides the necessary information on the genetic counseling side (Wertz and Fletcher Reference Wertz and Fletcher2004).
The present article has investigated abortion attitudes as of the mid-1990s in every country then-surveyed. Then with a series of statistical tests, it has shown that genetic counseling practices closely aligned with prevailing abortion attitudes in the society in which they occurred. Where abortion was unacceptable, it was considered legitimate to advise against aborting genetically anomalous pregnancies. Conversely, in a society where abortion was widely accepted, it was considered legitimate to encourage aborting genetically affected pregnancies. However, where abortion was controversial, the practice was to strive for non-directiveness and present only facts and available options without recommendations. Aligning with much historically informed medical sociology (e.g., Latour and Woolgar Reference Latour and Woolgar1986 [1979]; Payer Reference Payer1988; Latour Reference Latour1999; Harding Reference Harding, Essed, Theo Goldberg and Kobayashi2009; Kuhn Reference Kuhn2012 [1962]; Stein Reference Stein2018 [1990]), this argument supports the perspective that varying cultural values across countries help to determine varying medical practices.
This pattern was so strong that it applied to intermediate gradations in counseling directiveness and abortion attitudes and produced highly significant statistical results. Each of the few exceptional countries had some plausible peculiarity in its political history or level of national integration. Beginning with the least directive countries and moving toward the most directive, the pattern was as follows: countries in which abortion was politically polarized were the least directive in the world. They were followed by counties in which abortion was more moderately contentious, then a set of countries in which abortion was broadly rejected and not politically contentious. The median and slightly above median segments of the directiveness spectrum include a mixture of countries that broadly accepted and broadly rejected abortion, and also the two countries that sharply divided by region or historical period. Finally, the top quarter consisted of countries in which abortion was broadly accepted and not politically contentious.
As predicted in hypothesis 1, societies in which abortion was polarized consistently ranked as the least directive in genetic counseling. Poland, which split by historical period, ranked in the exact middle of the directiveness scale, consistent with the interpretation that Polish genetic counselors operated under the influence of their training, which took place during a period of broad acceptance of abortion.
As predicted in hypothesis 2, most societies in which abortion was contentious also ranked low in directiveness. There were two exceptions. Portugal, where abortion was moderately controversial in the political arena but the population was apathetic toward abortion policy (Blofield Reference Blofield2006: 181–2), ranked in the middle on directiveness. Belgium, with a mostly pro-liberalization abortion population cleaved by regional divisions and a no-motion political system (Witte et al. Reference Witte, Craeybeckx and Meynen2009), ranked within the top half of the directiveness distribution but not near the extreme.
As predicted in hypotheses 3 and 4, societies in which abortion was broadly accepted or broadly rejected constituted the upper three-quarters of the directiveness distribution. This result holds when including those countries in which abortion was moderately controversial politically but broadly accepted among the population. Of these, Spain was near the exact middle, and the other three were in the upper third. The overall pattern was highly statistically significant.
What was decisive for counseling practices was not whether countries broadly accepted or broadly rejected abortion. It was whether or not countries had a clear social consensus on abortion. This is why genetic counselors in countries with opposite abortion values answered similarly when asked if they would be directive: they would be directive in opposite ways. It was when abortion was controversial that genetic counselors were non-directive. In summary, the more controversial abortion was within a society, the less directive genetic counselors were willing to be, whereas the less controversial abortion was, the more directive the counseling.









 Open access
Open access