



Introduction
Gender-typed behavior refers to behaviors that differ on average for females and males (Li, Kung, & Hines, Reference Li, Kung and Hines2017), whereas gender nonconformity is the extent to which a person's gender identity, role, or expression differs from the cultural norms prescribed for people of a particular gender (Coleman et al., Reference Coleman, Bockting, Botzer, Cohen-Kettenis, DeCuypere, Feldman and Zucker2012). Gender nonconforming behavior typically emerges around age 2 or 3 and becomes more evident later in childhood (Li et al., Reference Li, Kung and Hines2017; Rieger, Linsenmeier, Gygax, & Bailey, Reference Rieger, Linsenmeier, Gygax and Bailey2008). The prevalence of gender nonconforming behavior may vary depending on study settings (Zucker, Reference Zucker2017), but past reports suggest that the percentage is approximately 3% in boys and 13% in girls (Achenbach & Edelbrock, Reference Achenbach and Edelbrock1987; Achenbach & Rescorla, Reference Achenbach and Rescorla2001).
Individuals who experience gender nonconformity often face stigmatization in various forms, and the subsequent discrimination, family rejection, and social exclusion may result in psychological distress and mental health symptoms (Baams, Beek, Hille, Zevenbergen, & Bos, Reference Baams, Beek, Hille, Zevenbergen and Bos2013; Hall-Lande, Eisenberg, Christenson, & Neumark-Sztainer, Reference Hall-Lande, Eisenberg, Christenson and Neumark-Sztainer2007; Klein & Golub, Reference Klein and Golub2016; Martin-Storey & August, Reference Martin-Storey and August2016; VanBergen & Love, Reference VanBergen and Love2022). Previous studies have shown mixed results regarding gender nonconformity and mental health, suggesting that the associations may be context- and age-specific (Bennett, Borczon, & Lewis, Reference Bennett, Borczon and Lewis2019; Jones, Robinson, Oginni, Rahman, & Rimes, Reference Jones, Robinson, Oginni, Rahman and Rimes2017; Oginni, Robinson, Jones, Rahman, & Rimes, Reference Oginni, Robinson, Jones, Rahman and Rimes2019; Roberts, Rosario, Slopen, Calzo, & Austin, Reference Roberts, Rosario, Slopen, Calzo and Austin2013; Warren, Goldsmith, & Rimes, Reference Warren, Goldsmith and Rimes2019). For example, a study from a US cohort (N = 10 655) demonstrated an association between a retrospective examination of child gender nonconformity and depression from age 12 through 30 (Roberts et al., Reference Roberts, Rosario, Slopen, Calzo and Austin2013), whereas another study from a UK cohort (N = 4564) found no significant association between childhood gender nonconformity and anxiety disorder at age 17.5 (Jones et al., Reference Jones, Robinson, Oginni, Rahman and Rimes2017). Other studies have documented the social exclusion of gender nonconforming adolescents (Aspenlieder, Buchanan, McDougall, & Sippola, Reference Aspenlieder, Buchanan, McDougall and Sippola2009; Heinze & Horn, Reference Heinze and Horn2014; Martin-Storey & Baams, Reference Martin-Storey, Baams and Fitzgerald2019), which may result in subjective experiences of rejection and loneliness (Rood et al., Reference Rood, Reisner, Surace, Puckett, Maroney and Pantalone2016). Such experiences, in turn, have been associated with depression (Cacioppo, Hughes, Waite, Hawkley, & Thisted, Reference Cacioppo, Hughes, Waite, Hawkley and Thisted2006; Erzen & Çikrikci, Reference Erzen and Çikrikci2018) and sub-clinical psychotic experiences (Chau, Zhu, & So, Reference Chau, Zhu and So2019; Narita et al., Reference Narita, Banawa, Zhou, DeVylder, Koyanagi and Oh2021; Narita, Stickley, & DeVylder, Reference Narita, Stickley and DeVylder2020). In contrast, there is some evidence that socially transitioned transgender children who are supported in their gender identity may have normal levels of depression (Olson, Durwood, DeMeules, & McLaughlin, Reference Olson, Durwood, DeMeules and McLaughlin2016). Thus, the association between gender nonconformity and mental health may be socially produced rather than attributed to individual-level factors.
Adolescence is a critical period for social and emotional development, in which many mental health problems first emerge (World Health Organization, 2021). However, to our knowledge, no prospective study has evaluated the association between gender nonconformity during this developmental period and subsequent mental health. Furthermore, there has been no examination of gender nonconformity as a time-varying variable, accounting for time-varying confounders. We addressed these issues using longitudinal data collected at three time points (ages 12, 14, and 16). We aimed to examine the association of gender nonconformity at ages 12 and 14 with subsequent mental health at age 16, controlling for time-fixed and time-varying confounders. We evaluated depression, psychotic experiences, and anxiety because a substantial proportion of individuals during adolescence are at risk of experiencing these conditions (Kowalchuk, Gonzalez, & Zoorob, Reference Kowalchuk, Gonzalez and Zoorob2022; McMahon et al., Reference McMahon, Corcoran, Keeley, Clarke, Coughlan, Wasserman and Cannon2021; Thapar, Collishaw, Pine, & Thapar, Reference Thapar, Collishaw, Pine and Thapar2012). Specifically, psychotic experiences, which are common during adolescence (Endo et al., Reference Endo, Yamasaki, Nakanishi, DeVylder, Usami, Morimoto and Nishida2022), are of particular importance in sexual minority individuals (Post, Veling, & GROUP investigators, Reference Post and Veling2021), thereby emphasizing the necessity of rigorously examining this outcome. While some individuals may hold prejudice against this particular condition (Baba et al., Reference Baba, Nemoto, Tsujino, Yamaguchi, Katagiri and Mizuno2017), it is precisely for this reason that we impartially evaluated psychotic experiences along with other common conditions, namely depression and anxiety. Also, we investigated potential differences in these associations across gender because past research has suggested substantial heterogeneity (Warren et al., Reference Warren, Goldsmith and Rimes2019). Finally, we conducted mediation analysis, considering the possibility that the association between gender nonconformity and mental health may be socially produced. We explored the extent to which the association between gender nonconformity at age 12 and mental health at age 16 was mediated by a set of psychosocial factors at age 14. These include loneliness, bullying victimization, and relationships with mothers, fathers, and friends - factors upon which intervention can reduce stigmatization and ameliorate mental health challenges.
Methods
Study design and population
We used data from a population-based birth cohort (Tokyo Teen Cohort: TTC) (Ando et al., Reference Ando, Nishida, Yamasaki, Koike, Morimoto and Hoshino2019). The TTC is a multidisciplinary survey assessing the health and development of adolescents born between September 2002 and August 2004. We conducted a random sampling via the basic resident register in three municipalities in Japan: Setagaya, Mitaka, and Chofu. Data were collected at three time points when participants were at ages 12, 14, and 16. A trained interviewer visited the participants’ houses at each time point to administer self-report questionnaires to child-parent pairs and performed a semi-structured interview.
Ethical considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the Institutional Review Boards of the Tokyo Metropolitan Institute of Medical Science (12–35), the University of Tokyo (10 057), and SOKENDAI (the Graduate University for Advanced Studies; 2 012 002). Every parent provided written informed consent.
Measures
Gender nonconformity
We evaluated gender nonconformity at ages 12 and 14 as a time-varying variable. We used the Youth Self Report (YSR), a widely used measure of youth emotion and behaviors (Achenbach & Rescorla, Reference Achenbach and Rescorla2001). We assessed gender nonconformity using two items: gender nonconforming behavior and the wish to be of the other gender (Zucker, Reference Zucker2017). Each child self-reported if he or she ‘behaves like opposite gender’ and ‘wishes to be of opposite gender’ with three response options: ‘not at all’, ‘somewhat or sometimes true’, or ‘very true or often true’.
Depression (outcome)
To evaluate depression at ages 12 and 16, we used the Short Mood and Feelings Questionnaire (SMFQ), a validated 13-item self-report questionnaire (Angold, Costello, Messer, & Pickles, Reference Angold, Costello, Messer and Pickles1995; Sharp, Goodyer, & Croudace, Reference Sharp, Goodyer and Croudace2006). Children provided information on each item with three response options: ‘always’, ‘sometimes’, and ‘never’, scored with 2, 1, and 0 points, respectively. Each item was summed into a composite score (range: 0–26); a greater score suggests more severe depression. Our data at age 16 showed strong internal consistency (Cronbach's α = 0.92).
Psychotic experiences (outcome)
To examine psychotic experiences at age 16, we used the Adolescent Psychotic-like Symptom Screener (APSS), a validated seven-item self-report measure (Kelleher, Harley, Murtagh, & Cannon, Reference Kelleher, Harley, Murtagh and Cannon2011; Laurens et al., Reference Laurens, Hodgins, Maughan, Murray, Rutter and Taylor2007). The details of the measurement can be found in online Supplementary Table S1. Children provided information on each item with three response options: ‘yes, definitely’, ‘maybe’, and ‘no, never’, scored with 1, 0.5, and 0 points, respectively. Each item was summed into a composite score (range = 0–7); a greater score suggests more severe psychotic experiences. Our past report showed that the Japanese version of the APSS had acceptable internal consistency (Cronbach's α = 0.71) (Ando et al., Reference Ando, Nishida, Usami, Koike, Yamasaki, Kanata and Kasai2018).
Anxiety (outcome)
To examine anxiety levels at ages 12 and 16, we utilized the Child Behavior Checklist (CBCL), a caregiver-reported questionnaire comprising 118 items. To minimize the burden on participants, we selected 84 items from the CBCL for our survey. Out of these, 14 items were specifically designed to assess anxiety, derived from the CBCL anxiety scale (CBCL-A), which initially consisted of 16 items. Each item was rated on a three-point scale: ‘not true’, ‘somewhat or sometimes true’, and ‘very true or often true’. A total score was calculated by summing the responses for each item, with higher scores indicating higher levels of anxiety (ranging from 0 to 28). These 14 items demonstrated acceptable internal consistency (Cronbach's α = 0.78) (Iijima et al., Reference Iijima, Okumura, Yamasaki, Ando, Nakanishi, Koike and Nishida2019).
Covariates
We evaluated covariates at age 12 that might serve as potential confounders. We employed the disjunctive cause criterion to control for potential causes of the exposure, outcome, or both, excluding instrumental variables and including covariates that acted as proxies for unmeasured variables that are common causes of both the exposure and the outcome (VanderWeele, Reference VanderWeele2019). The model incorporated a range of variables at age 12, including age (months, continuous), gender (dichotomous), body mass index (continuous), IQ (continuous), neighborhood characteristics (continuous), and relationships with mother, father, and friends (continuous). Also, each mental health outcome at age 12 (continuous) was included per analysis to control for pre-existing mental health status. We included neighborhood characteristics evaluated by the Neighborhood Collective Efficacy (NCE) scale (Nakanishi et al., Reference Nakanishi, Yamasaki, Ando, Endo, Richards, Hiraiwa-Hasegawa and Nishida2022) because they possibly correlate with mental health (Fedina et al., Reference Fedina, Mushonga, Bessaha, Jun, Narita and DeVylder2021; Narita et al., Reference Narita, Knowles, Fedina, Oh, Stickley, Kelleher and DeVylder2020). The NCE is a five-item scale where respondents were asked to rate each item on a five-point Likert scale, ranging from strongly agree to strongly disagree. A higher total score indicates greater neighborhood cohesion. The details of the measurement can be found in online Supplementary Table S2. The relationships with mother, father, and friends were evaluated using the Network of Relationships Inventory, where a higher score indicates better relationships (Furman & Buhrmester, Reference Furman and Buhrmester2009). Psychotic experiences at age 12 were assessed using items from the schizophrenia section of the Diagnostic Interview Schedule for Children (Costello, Edelbrock, & Costello, Reference Costello, Edelbrock and Costello1985).
For the main analysis, we further evaluated relationships with mother, father, and friends at age 14 as time-varying confounders, which may be affected by gender nonconformity at age 12 and also confound the association between gender nonconformity at age 14 and mental health at age 16. It is often debated that variables present on the causal pathway between exposure and outcome should not be treated as confounders because adjusting for them may introduce bias. However, this characterization of confounders may not apply to time-varying variables, and g-methods such as inverse probability weighting could be used to control for these variables unbiasedly, handling exposure-confounder feedback (Hernán & Robins, Reference Hernán and Robins2020; VanderWeele, Reference VanderWeele2019). We fitted models with and without these factors at age 14 to examine how the results may change, as outlined in the statistical analysis section below.
Mediators
We evaluated multiple mediators, namely loneliness, bullying victimization, and relationships with mother, father, and friends, a priori based on subject knowledge, all of which were evaluated at ages 12 and 14. To evaluate loneliness, we used a relevant item from the SMFQ (Angold et al., Reference Angold, Costello, Messer and Pickles1995; Sharp et al., Reference Sharp, Goodyer and Croudace2006). Each child self-reported if he/she ‘feels lonely’ with three response options: ‘always’, ‘sometimes’, and ‘never’. We created a dichotomous variable, and selecting ‘always’ or ‘sometimes’ was considered loneliness. To evaluate bullying victimization, we used a relevant item from the Strengths and Difficulties Questionnaire (SDQ) (Goodman, Reference Goodman1997). Parents reported if their children are ‘picked on or bullied by other children’ with three response options: ‘not true’, ‘somewhat true’, and ‘certainly true’. We created a dichotomous variable, and selecting ‘somewhat true’ or ‘certainly true’ were considered as experiencing bullying victimization. While relationships with mother, father, and friends at age 14 were accounted for as potential confounders between gender nonconformity at age 14 and mental health at age 16 in the main analysis, these factors were included in the mediation analysis as potential mediators between gender nonconformity at age 12 and mental health at age 16. In the mediation analysis, mediators at age 12 were controlled for, in addition to the aforementioned covariates.
Statistical analysis
The directed acyclic graph of the hypothesized associations is shown in Fig. 1. To evaluate the association of gender nonconformity at ages 12 and 14 with subsequent mental health at age 16, we used inverse probability weighting and marginal structural models with robust standard errors (Hernán & Robins, Reference Hernán and Robins2020). Time-fixed and time-varying confounders were controlled for using inverse probability weighting. We obtained stabilized weights for gender nonconformity at ages 12 and 14 utilizing separate logistic models for exposures at ages 12 (adjusting for covariates at age 12) and 14 (adjusting for exposure at age 12 and covariates at ages 12 and 14). By applying this weighting, a simulated population was generated that represents what the cohort may have resembled if the covariates had been equally distributed among groups. Our outcome model included an interaction between gender nonconformity at ages 12 and 14.
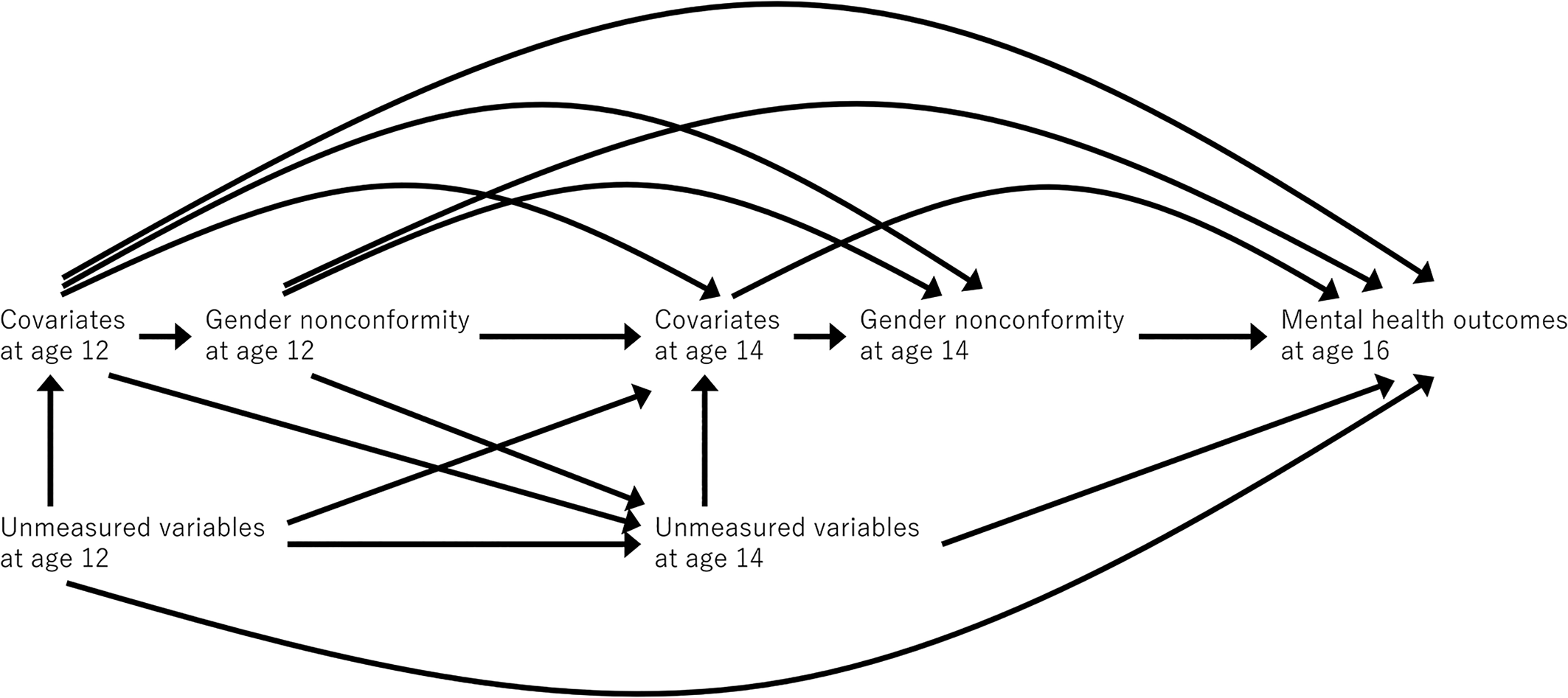
Figure 1. Directed acyclic graph for the main analysis.
We conducted a series of sensitivity analyses for the main analysis. First, we assessed the robustness of the estimates to unmeasured confounding by analyzing E-values (VanderWeele & Ding, Reference VanderWeele and Ding2017). We examined the minimum strength of association that unmeasured confounding would need to have above and beyond the measured covariates to explain away the estimates. Second, we employed models excluding relationships with mother, father, and friends at age 14, as mentioned in the covariates section above. Third, we evaluated puberty at age 12 using Tanner Stages (Emmanuel & Bokor, Reference Emmanuel and Bokor2022), considering that a significant proportion of participants may not have reached puberty at this age. We created a dichotomous variable (Stage 1 or Stage 2–5) and included it in the model to examine how the results change. Fourth, we used dichotomous variables to evaluate depression and psychotic experiences. For depression, we used an SMFQ score of 8 as the cutpoint based on the past report (Angold et al., Reference Angold, Costello, Messer and Pickles1995). For psychotic experiences, to account for potential under-reporting, selecting ‘maybe’ or ‘yes, definitely’ for at least one item in the APSS constituted any psychotic experience. Fifth, we evaluated gender nonconformity using an item that is analogous to the criterion for gender dysphoria outlined in the DSM-5 (American Psychiatric Association, 2013). Children self-reported if they had ‘a dislike of their sexual anatomy because of the incongruence with experienced gender’, with five response options: ‘not at all’, ‘somewhat’, ‘fairly’, ‘strongly’, and ‘very strongly’.
Next, we assessed the extent to which the relationship between gender nonconformity and mental health differed depending on the participant's gender. To accomplish this, we applied inverse probability weighting and incorporated the interactions between gender nonconformity and gender, while controlling for both time-fixed and time-varying confounders. Here we analyzed mental health outcomes as both continuous and dichotomous variables.
To account for missing data, we employed multiple imputation via chained equation. We included all relevant variables, creating multiple imputed data sets using the mice R package (van Buuren & Groothuis-Oudshoorn, Reference van Buuren and Groothuis-Oudshoorn2011). Each of these data sets was separately analyzed, and the results from all imputations were combined. Since statistical software packages did not support this combining process for our analyses, we manually combined the results based on Rubin's rules (Rubin, Reference Rubin1987). Twenty imputed datasets were utilized for the main analysis, along with five datasets for the sensitivity analyses and analysis of heterogeneity across gender.
Finally, we applied mediation analysis methods (VanderWeele, Reference VanderWeele2015) to examine how the association between gender nonconformity at age 12 and mental health at age 16 was mediated by the aforementioned mediators at age 14. Here we only analyzed participants without missing data, as mediation analyses accounting for missing data may require additional development. To address exposure-mediator and mediator–mediator interactions (e.g. the interaction between bullying victimization and loneliness), we employed a weighting approach using an outcome model to collectively assess all mediators (VanderWeele & Vansteelandt, Reference VanderWeele and Vansteelandt2014). The details of the weighting approach can be found in online Supplementary Table S3. The weighting approach estimated the direct and indirect effects. Bootstrap confidence intervals (CIs) for these effects were obtained utilizing normal approximation. Proportion mediated on each mental health outcome was calculated as the indirect effect divided by the total effect. For the outcome measure of depression, the SMFQ includes an item for loneliness, which is included as one of the mediators; thus, we conducted a sensitivity analysis using the SMFQ, removing the loneliness item.
Results
Baseline characteristics
Table 1 shows the baseline characteristics of participants by gender nonconformity. Of 3171 participants, 704 (22.2%) had gender nonconforming behavior, while 467 (14.7%) expressed a wish to be of the other gender. Individuals with gender nonconformity exhibited elevated levels of psychotic experiences. No substantial differences were observed in the other variables between the two groups. Additionally, we did not find a substantial difference between participants with and without missing data.
Table 1. Baseline characteristics of participants by gender nonconformity
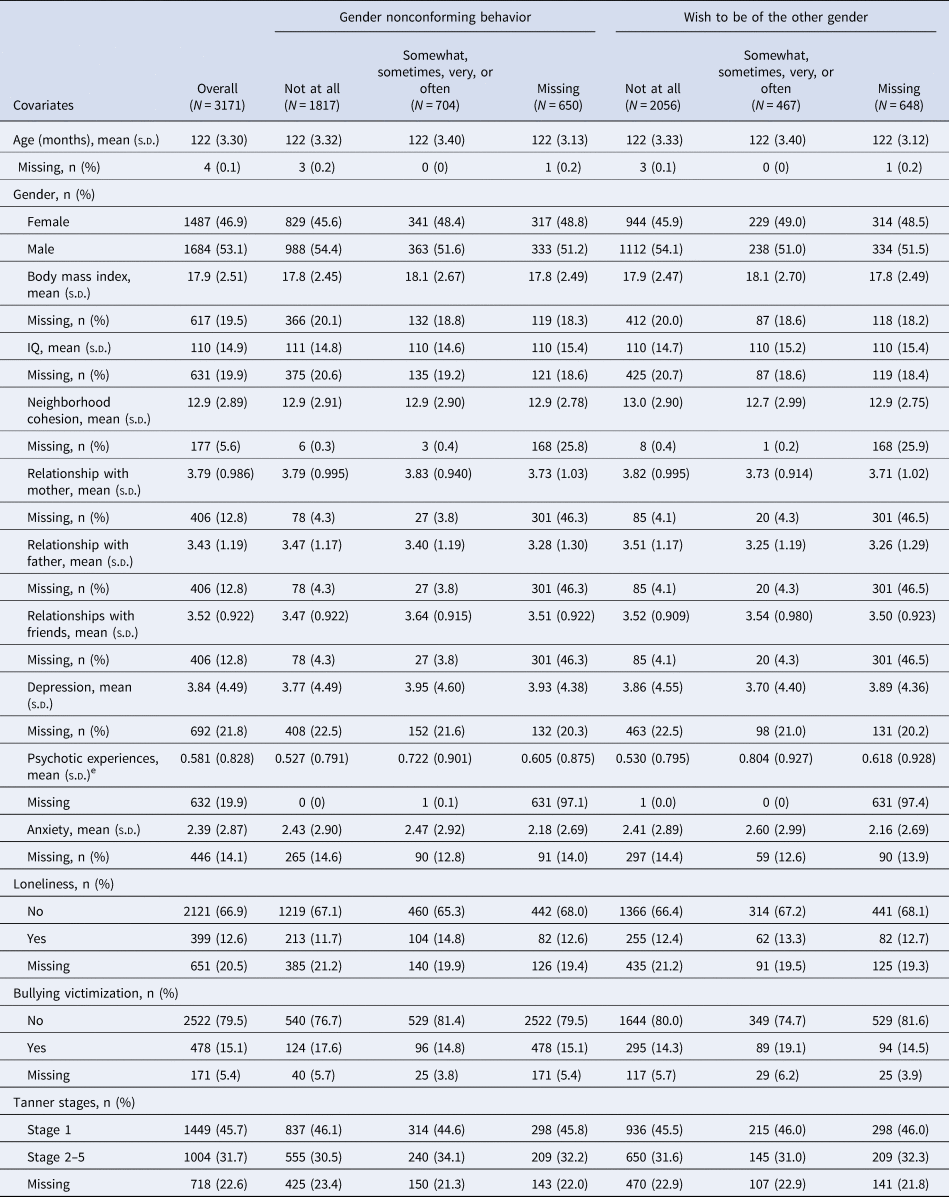
Abbreviation: SD, standard deviation.
Gender nonconformity as a time-varying variable and subsequent mental health
At age 16, 1920 (60.5%) participants completed the measure for depression, 1927 (60.8%) for psychotic experiences, and 2262 (71.3%) for anxiety. Three-hundred-fifty-six participants exhibited gender nonconforming behavior at age 12 only, 241 at age 14 only, and 109 at both ages, while 933 participants never displayed it. Also, 242 participants expressed the wish to be of the other gender at age 12 only, 307 at age 14 only, and 65 at both ages, while 1027 participants never expressed this wish. Table 2 summarizes the main analysis. The overall results suggested an association between gender nonconformity and subsequent mental health. Specifically, persistent gender nonconforming behavior at ages 12 and 14 was associated with subsequent depression (β = 2.02, 95% CI 0.85 to 3.19) and psychotic experiences (β = 0.33, 95% CI 0.14 to 0.52) at age 16. This suggests that individuals with persistent gender nonconforming behavior had a 2-point higher SMFQ score and a one-third-point higher APSS score, compared to individuals without such behavior. The association between persistent gender nonconforming behavior and anxiety did not reach statistical significance (β = 0.65, 95% CI −0.03 to 1.34). Similar findings were observed when evaluating the persistent wish to be of the other gender.
Table 2. Associations of gender nonconformity at ages 12 and 14 with subsequent mental health outcomes at age 16
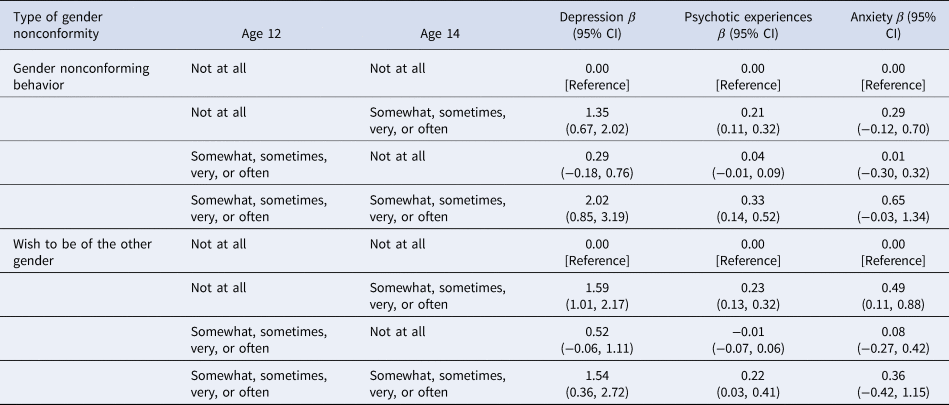
Abbreviation: CI, confidence interval.
Marginal structural model with weights accounted for covariate distributions between groups. The model included the interaction between gender nonconformity at ages 12 and 14. For variable selection, see the Covariates subsection of the Methods section. Missing data were handled using multiple imputation via chained equation.
Sensitivity analysis
The calculated E-values showed that some observed associations between gender nonconformity and mental health outcomes were reasonably robust to unmeasured confounders (Table 3). For instance, for the association between gender nonconforming behavior and psychotic experiences, an unmeasured confounder would need to be associated with both of them above and beyond the adjusted covariates by a risk ratio of 2.51 to fully explain away the observed association and 2.10 to shift the CI to include the null value. Results did not substantially change when excluding relationships with mother, father, and friends at age 14 (online Supplementary Table S4), including puberty at age 12 in the model (online Supplementary Table S5), and using dichotomous variables to evaluate depression and psychotic experiences at age 16 (online Supplementary Table S6). The analysis of models evaluating the dislike of their sexual anatomy indicated that this factor had an important role on subsequent mental health at age 16, specifically at age 14 and not at age 12 (online Supplementary Table S7), suggesting that it reflects different dimensions compared to gender nonconforming behavior and the wish to be of the other gender.
Table 3. Robustness to unmeasured confounding of the observed associations
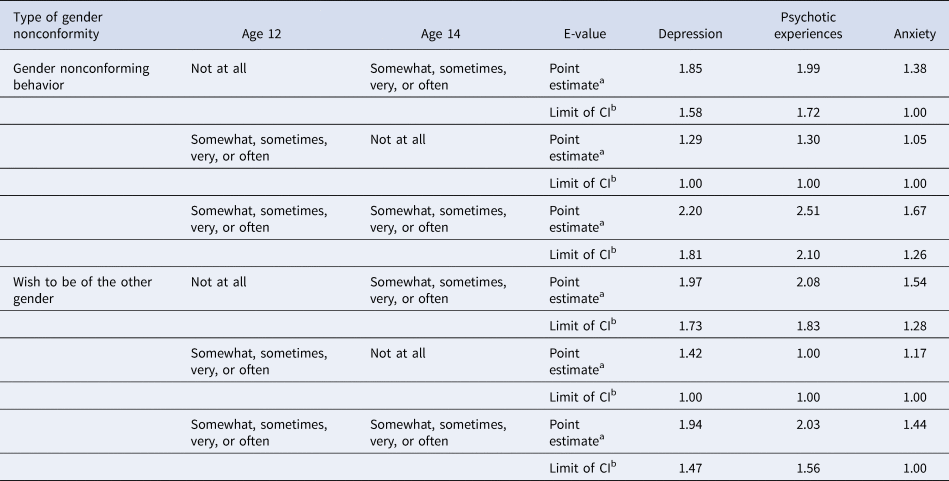
Abbreviations: CI, confidence interval.
The associations were based on the marginal structural models that included the interaction between gender nonconformity at ages 12 and 14.
a E-values for point estimates are the minimum strength of association on the risk ratio that unmeasured confounding would need to have above and beyond the adjusted covariates to explain away the estimates.
b E-values for limit of CI are the minimum strength of association on the risk ratio that unmeasured confounding would need to have above and beyond the adjusted covariates to shift the 95% CI and include the null value.
Heterogeneity across gender
The results regarding the heterogeneity across gender evaluating mental health can be found in online Supplementary Table S8 and S9. The results appeared to be inconsistent. For example, when analyzing mental health outcomes as continuous variables, the association between persistent gender nonconformity and depression appeared stronger in female participants than in male participants. However, the findings were reversed when analyzing psychotic experiences. Note that these results should be interpreted carefully, as analyses of interactions not only demand a high level of statistical power, but may also have been affected by an imbalance of power across genders and potential model misspecification, especially considering the dependency of interaction analyses on the models (Zammit, Lewis, Dalman, & Allebeck, Reference Zammit, Lewis, Dalman and Allebeck2010).
Mediation analyses with multiple mediators
We conducted mediation analyses to estimate the proportion of the association mediated through psychosocial factors, which are factors that can be intervened upon (online Supplementary Table S10). Note that here we analyzed all mediators simultaneously using an outcome model, which enabled us to account for exposure-mediator and mediator–mediator interactions. Loneliness, bullying victimization, and relationships with mother, father, and friends emerged as important mediators of the relationship between gender nonconformity and mental health. Specifically, these psychosocial factors consistently mediated a substantial proportion of the association between gender nonconformity and depression (gender nonconforming behavior: 29.8%; wish to be of the other gender: 26.0%). As shown in online Supplementary Table S11, the sensitivity analysis excluding the loneliness item from the SMFQ demonstrated similar results (gender nonconforming behavior: 30.0%; wish to be of the other gender: 26.4%).
Discussion
Main findings
In this birth cohort study, we showed the association between gender nonconformity, measured repeatedly during adolescence, and subsequent mental health. We observed that adolescents who experienced gender nonconformity, particularly when exhibited persistently, faced worse mental health outcomes later on. The robustness of these findings was confirmed through a series of sensitivity analyses. Our results provide new evidence supporting the association between repeated measurement of gender nonconformity during adolescence, a critical period for social and emotional development, and subsequent mental health.
Heterogeneity across gender
Previous research (Warren et al., Reference Warren, Goldsmith and Rimes2019) indicated a gender difference in the association between gender nonconformity and mental health, specifically noting a significant relationship between gender nonconformity and emotional and peer problems in boys but not girls. Our examination of heterogeneity across gender yielded inconsistent results, differing from prior research. It is worth noting that while the prior research utilized the Child Activities Inventory (CAI) to assess gender nonconformity (Golombok et al., Reference Golombok, Rust, Zervoulis, Croudace, Golding and Hines2008), we employed the YSR (Achenbach & Rescorla, Reference Achenbach and Rescorla2001). Both measures assess gender nonconformity, but they differ significantly, potentially leading to divergent findings. For example, the CAI uses questionnaire assessments for toy preferences, unlike the YSR. Another possibility that deserves attention is that each gender might have had a different statistical power. In addition, the analysis of interaction is dependent on the models (Zammit et al., Reference Zammit, Lewis, Dalman and Allebeck2010), and any model misspecification could have affected the results. Taken together, the interpretation of the analysis for heterogeneity across gender should be considered carefully.
Interpretation of the findings
While our longitudinal data suggest the association between gender nonconformity and mental health, interpreting the results of such non-modifiable factor is challenging (Glymour & Spiegelman, Reference Glymour and Spiegelman2017; VanderWeele & Robinson, Reference VanderWeele and Robinson2014). Thus, we further explored the mediating role of loneliness, bully victimization, relationships with mother, father, and friends, which may be modifiable factors. Our findings indicate that these psychosocial factors may play a crucial mediating role between gender nonconformity and subsequent mental health, proposing that this association might be socially influenced. Traditionally, distress related to gender nonconformity has been approached from a medical perspective (e.g. with the controversial gender identity disorder (DSM-IV) and gender dysphoria (DSM-5) diagnoses (Beek, Cohen-Kettenis, & Kreukels, Reference Beek, Cohen-Kettenis and Kreukels2016; Davy & Toze, Reference Davy and Toze2018)). This approach tends to focus on individual-level interventions, which may provide some benefits. Indeed, a recent study demonstrated that increases in appearance congruence resulting from gender-affirmative hormones were associated with reductions in depression and anxiety (Chen et al., Reference Chen, Berona, Chan, Ehrensaft, Garofalo, Hidalgo and Olson-Kennedy2023). However, our results highlight that social intervention and change may be essential, as psychosocial factors have a key role in the association between gender nonconformity and mental health. Minority stress theory (Meyer, Reference Meyer1995) and modified labeling theory (Link, Cullen, Struening, Shrout, & Dohrenwend, Reference Link, Cullen, Struening, Shrout and Dohrenwend1989) outline mechanisms through which one's minority status (based on appearance or self-identification) can lead to social exclusion, marginalization, and poor self-esteem, all of which have been variously linked to mental health problems (Monroe & Simons, Reference Monroe and Simons1991; Pruessner, Cullen, Aas, & Walker, Reference Pruessner, Cullen, Aas and Walker2017; Selten, van der Ven, Rutten, & Cantor-Graae, Reference Selten, van der Ven, Rutten and Cantor-Graae2013). Accordingly, public health approaches that address the social experience of gender nonconforming and other marginalized youth may yield improved mental health outcomes. While an examination of potential community-level approaches to addressing marginalization and related factors is beyond the scope of this paper, some promising approaches include the Good Behavior Game for classroom management of interpersonal conflicts (Kellam et al., Reference Kellam, Mackenzie, Brown, Poduska, Wang, Petras and Wilcox2011) and multi-level approaches to stigma reduction (Rao et al., Reference Rao, Elshafei, Nguyen, Hatzenbuehler, Frey and Go2019).
Strengths
Our cohort study has several strengths. First, we evaluated gender nonconformity during adolescence, a critical stage of social and emotional development where evidence is limited. Second, we collected longitudinal data at three time points, enabling us to examine the repeated measures of gender nonconformity and time-varying confounders. We utilized inverse probability weighting and marginal structural models, which can handle exposure-confounder feedback that cannot be addressed through traditional outcome regression or stratification methods (Hernán & Robins, Reference Hernán and Robins2020). Additionally, our mediation analysis considered the exposure, mediator, and outcome at different time points (ages 12, 14, and 16, respectively), which is essential for providing causal interpretations but is often overlooked (VanderWeele, Reference VanderWeele2015). To mitigate confounding bias, we controlled for the prior outcome in the main analysis and the prior mediators and outcome in the mediation analysis. Lastly, a wide range of sensitivity analyses confirmed the robustness of our findings.
Limitations
Several limitations should be acknowledged here. First, we lacked information on certain potentially important factors, such as adverse childhood experiences (Stickley et al., Reference Stickley, Waldman, Ueda, Koyanagi, Sumiyoshi, Narita and Oh2020, Reference Stickley, Waldman, Sumiyoshi, Narita, Shirama, Shin and Oh2021), which should be controlled for in future studies. Also, evaluating sexual orientation would provide contextualization for the association found in the present study, as it could serve as both a confounder and a mediator, existing before or after an individual's experience of gender nonconformity. Second, measurement bias is conceivable. We utilized questionnaires to assess psychopathology, which, although validated, may not reflect the actual pathology as accurately as a clinical interview. Specifically, the self-report nature of the APSS might have led to false-positive psychotic experiences (Dominguez, Wichers, Lieb, Wittchen, & van Os, Reference Dominguez, Wichers, Lieb, Wittchen and van Os2011; Staines et al., Reference Staines, Healy, Coughlan, Clarke, Kelleher, Cotter and Cannon2022). Regarding the measurement of gender nonconformity, we used a single item from the YSR, and while validated, employing continuous variables like the CAI might provide more comprehensive information. Also, social desirability bias may have led to underreporting, although it is worth noting that the prevalence of gender nonconformity in our data was higher than in previous research (Zucker, Reference Zucker2017). Regarding the mediators, we used a single item to evaluate loneliness and bullying victimization, respectively. This approach might have led to more false negatives, potentially underestimating the mediating role, even though our findings still demonstrated a substantial proportion mediated. Third, missing data were accounted for utilizing multiple imputation via chained equation. Still, a conceivable proportion of the sample was missing, which might have resulted in biased estimates. Fourth, as mentioned above, the analysis of heterogeneity across gender should be interpreted carefully due to potential challenges. These include a possible lack of statistical power, imbalances in statistical power across gender, and potential model misspecification that could have influenced the results. Lastly, generalizability may be limited as our sample was drawn from Tokyo, a highly urbanized city, and primarily consisted of individuals of Asian ethnicity. Caution should be exercised when extending the findings to rural areas and other racial groups.
Conclusion
Persistent gender nonconformity during adolescence is associated with subsequent mental health. Psychosocial factors play a vital mediating role in this association, highlighting the essential need for social intervention and change to reduce stigmatization and ameliorate mental health challenges.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291723002623.
Acknowledgements
The authors sincerely thank all the child-parent pairs who participated in this study.
Funding statement
This work was supported by a Grant-in-Aid for Scientific Research on Innovative Areas (23118002; Adolescent Mind & Self-Regulation) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan; Japan Society for the Promotion of Science (JSPS) KAKENHI (grant numbers JP16H06395, 16H06398, 16H06399, 16K21720, 16K15566, 16H03745, 17H05931, 20H03951, 20H01777, JP20H03596, JP21H05171 and JP21H05173); the UTokyo Center for Integrative Science of Human Behavior (CiSHuB); the International Research Center for Neurointelligence (WPI-IRCN) at the University of Tokyo Institutes for Advanced Study (UTIAS), and the JST (JPMJPF2105).
Competing interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.






