
Infectious disease is as old as life itself, with devastating pandemics and plagues recurring throughout history. More novel though, is the tendency to depict infectious disease as a serious security threat on a global scale. The identification of health with security was practically unheard of until the early 1990s (Elbe Reference Elbe2009; Fidler Reference Fidler2003b). Even the infamous 1918–19 Spanish Influenza, which caused millions of deaths worldwide, only started to be invoked as the epitome of a disastrous pandemic that must be prevented at all costs decades later. At the time, it was seen as part of the general misery associated with the First World War and its aftermath (Alcabes Reference Alcabes2009: 6). Now, however, for some of the world's most powerful governments and international organisations, notably the World Health Organization (WHO), rapidly spreading infectious diseases have come to be seen as ‘pressing existential threats that require urgent and extraordinary international policy responses’, thus ‘abandoning the decades-old convention of equating security with the absence of armed conflict between states’ (Elbe Reference Elbe2009: 2).
A burgeoning literature examining this securitisation of global health has considerably improved our understanding of the kinds of public health issues being discursively securitised – almost invariably, rapidly spreading infectious diseases – and who the securitising actors are. However, very few scholars have yet sought to systematically examine and explain how these diseases are managed in practice. Most scholars focus solely on the outcomes of interstate diplomacy, arguing that securitising infectious disease has generated a narrow, self-interested emphasis on ‘national security’, particularly among dominant Western states, rather than a cosmopolitan and just form of global health governance (Davies Reference Davies2010; Elbe Reference Elbe2009, Reference Elbe2010b). However, this supposed dichotomy between national security and governance overlooks the fact that, given the transboundary nature of infectious diseases, the practices associated with national security – preparedness against pandemics – have been fundamentally transformed. It is now seen to largely depend on interventions to reconfigure domestic health governance within other states so that they function as part of coordinated regional or global surveillance and containment efforts (see Calain Reference Calain2007). Given the health security literature's fixation on interstate diplomacy, it typically misses this crucial dynamic, and thereby fails to explore the factors shaping the actual implementation of international efforts to manage infectious disease (Curley and Herington Reference Curley and Herington2011).
To transcend this limitation, this chapter employs the State Transformation Approach (STA) to examine the governance of Highly Pathogenic Avian Influenza (HPAI) H5N1 in Southeast Asia. Popularly known as ‘bird flu’, H5N1 is a highly pathogenic variant of the influenza virus, typically found in poultry, but with the capacity to infect and kill humans through zoonotic (cross-species) transmission. Southeast Asia was the epicentre of the H5N1 outbreak, which occurred in the middle of the last decade. Bird-to-human, and possibly rare human-to-human, transmissions caused very high levels of mortality: 379 deaths in 638 confirmed cases as of January 2014, including in Indonesia, Thailand, Cambodia, Laos, Vietnam and Myanmar (WHO n.d.a). Public health officials’ main fear – that H5N1 would evolve to become rapidly transmissible among humans, creating a global pandemic – has not yet played out (Elbe Reference Elbe2010a: 49; Davis Reference Davis2005: 9–19)
Nonetheless, few infectious diseases have been discursively securitised by governments and international organisations as much and as often as H5N1. At the height of the panic, estimates of global deaths, if the virus were to mutate, ranged from 50 to 350 million people (Davis Reference Davis2005). During 2006, international donors pledged nearly US$2.4 billion towards managing the avian influenza threat. While much of this funding was dedicated to developing and purchasing H5N1 vaccines, substantial funds were earmarked for programmes of disease surveillance, capacity-building and response at the disease's points of origin (Scoones and Forster Reference Scoones and Scoones2010). From 2009, the sense of urgency has declined as H5N1 has not spread to new countries and human infections have decreased, leading to funding cuts for these programmes. However, H5N1 remains an important part of worldwide pandemic preparedness frameworks.
For Copenhagen School adherents, Southeast Asia's response to the H5N1 outbreaks seems puzzling. H5N1 was consistently ‘securitised’ by regional governments and in official ASEAN communiqués (ASEAN 2004b, 2007b). However, there was little concerted action to tackle the disease and no indication that it was elevated to the top of the political agenda within Southeast Asian states (Caballero-Anthony Reference Caballero-Anthony2008; Haacke and Williams Reference Haacke and Williams2008: 802–4). As chapter one showed, there is little in the Copenhagen toolkit to account for this unexpected paradox. Caballero-Anthony (Reference Caballero-Anthony2008) thus ends up urging a shift from the ‘securitisation’ of infectious disease to the ‘institutionalisation’ of a real regional response, without being able to explain why it has not already occurred.
This chapter transcends these limitations to explain the response to H5N1 in two key Southeast Asian states, Thailand and Indonesia. As the world's worst-affected territory, Indonesia received the most international funding for H5N1-related programmes: US$175 million from 2006 to 2010 (Forster Reference Forster and Scoones2010: 131; Forster and Charnoz Reference Forster and Charnoz2013: z). Thailand also suffered serious outbreaks. However, while in Thailand reported outbreaks of H5N1 in poultry are now sporadic and no human cases have emerged since 2006, in Indonesia the disease remains endemic in poultry and new human infections still occur, despite falling from fifty-five to nine cases annually between 2006 and 2012 (WHO n.d.a). Clearly, governance outcomes vary markedly, despite the fact Indonesia received the most foreign assistance. Much of this divergence is attributable to differences in the political economy of the poultry industry. In both countries, the industry had considerable influence over the scale at which the disease was managed and the effects of programmes developed to manage H5N1 in poultry.
In Thailand, much of the commercial poultry sector at the time of the first outbreak was industrialised, vertically integrated, export-oriented and politically connected. Consequently, the Thaksin government, in which industry-affiliated politicians were strongly represented, moved quickly to reassure export markets of the safety of Thai poultry. This involved centralising the response to H5N1 in the hands of the Thai national government, which stringently imposed international regulatory standards, but without involving international agencies directly. This response clearly favoured large-scale, export-oriented commercial interests: while it eventually restored their export markets, the high costs imposed on smallholders drove most out of business, further concentrating ownership in the hands of large-scale conglomerates (Safman Reference Safman and Scoones2010).
Indonesia, conversely, was subject to far greater, internationally driven rescaling efforts from the WHO and the UN Food and Agriculture Organization (FAO). Their programmes attempted to build up human and animal health services at the local level that empowered technical experts dedicated to implementing international guidelines, and to insert these into internationalised, multilevel governance mechanisms. These programmes attracted support from actors within Indonesia's central government as a means of attracting funding and restoring some authority lost during decentralisation. However, the implementation and efficacy of these governance institutions was also shaped by economic actors. Alongside a large ‘backyard’ sector – poor villagers cultivating chickens for household consumption or income – Indonesia's commercial poultry sector was far more segmented than in Thailand, and almost entirely domestically oriented (Leboeuf Reference Leboeuf2009: 49; Sumiarto and Arifin Reference Sumiarto and Arifin2008). It mainly comprised large, often transnational, corporations providing farming inputs on credit to thousands of small farms, which raised chickens, selling them to the corporations at set prices. Because corporations do not pay smallholders for dead chickens and have no export markets to lose, they were disinterested in tackling H5N1, and all sectors vigorously resisted culling (Charnoz and Forster Reference Charnoz and Forster2011). Commercial interests used their local and national political connections to resist thoroughgoing governance rescaling, deflecting it towards the ‘backyard’ sector instead. While outcomes in the ‘backyard’ sector are hailed as an ‘iconic success’ for health security governance (Perry et al. Reference Perry, Isa and Tarazona2009: 26), within the commercial sector they are negligible (Forster and Charnoz Reference Forster and Charnoz2013: ap).
The chapter proceeds as follows. The first section examines the securitisation of infectious disease and the rescaling of governance mechanisms for managing pandemic risk. The second then discusses the governance of H5N1 in Thailand and Indonesia in two subsections, respectively.
The securitisation of infectious disease
Infectious diseases and attempts to mitigate their effects are as old as human civilisation (Alcabes Reference Alcabes2009). However, since the early 1990s, infectious disease has increasingly been defined as a security problem (Fidler Reference Fidler2003b; McInnes and Lee Reference McInnes and Lee2006; Elbe Reference Elbe2009; see WHO and Heymann Reference Heymann2007). The burgeoning literature on health security is divisible into two main camps, as described in chapter one. The first, adopting a realist ontology, sees the securitisation of public health as reflecting the growing threat posed by existing and new pathogens. This literature argues that the undesirable side effects of globalisation, particularly the growing encroachment of humans on natural habitats, intensive industrial livestock farming practices, and climate change, along with the hypermobility that air travel provides for pathogens, have considerably heightened the risk of devastating pandemics (Garrett Reference Garrett1995; Dupont Reference Dupont2001: 212–27; Fidler Reference Fidler2003a; Elbe Reference Elbe2008).
However, there is simply no necessary correlation between the objective scale of a threat and the governance response to it. The infamous ‘Spanish flu’ of 1918–19 killed more people than World War I, without eliciting the kinds of discursive and governance responses observable today (Wraith and Stephenson Reference Wraith and Stephenson2009; Alcabes Reference Alcabes2009). Indeed, it generated no major revisions to the International Sanitary Regulations (ISRs), the international treaty dedicated to managing infectious disease. Conversely, viral outbreaks like SARS and H5N1 were used to promote revisions in the International Health Regulations (IHRs) – the successor to the ISRs – making the regime far more intrusive and regulatory. This is despite the fact that HPAI and SARS were only ever potential pandemics: in reality, they killed only hundreds of victims, while the Spanish flu killed tens of millions. Spanish flu claimed an estimated 4.3 million lives on the Indonesian island of Java alone (Chandra Reference Chandra2013). While H5N1 has killed fewer than 170 people across the entire Indonesian archipelago, it was subjected to vast and intrusive international intervention unimaginable in 1919.
The second camp within health security adopts the Copenhagen School approach, depicting the securitisation of infectious diseases as consequence of successful securitising moves rather than a changing threat environment. As in other subfields, scholars here have largely focused on applying the CS framework to this particular issue-area and on describing specific securitisations, identifying the actors, their discourses of threat and referent objects (e.g. Enemark Reference Enemark2009; Kelle Reference Kelle2007; Elbe Reference Elbe2009). This approach has been applied to the HPAI outbreaks. Elbe (Reference Elbe2010b), for example, shows medical professionals first securitised the disease as a political strategy to attract attention and resources to prevent a potentially devastating pandemic and to assist health systems in developing countries that had been devastated by decades of structural adjustment (also Davies Reference Davies2010). To make their case, they underscored the risk of a global pandemic, with some experts warning of up to 350 million deaths, although the WHO estimated 50 million (Davis Reference Davis2005).
This strategy clearly succeeded: few other pathogens have been described in starker terms by important governments and international organisations. In 2005, then US Senator, later President, Barack Obama wrote in the New York Times with fellow Senator Richard Lugar:
[W]hen we think of the major threats to our national security the first to come to mind are nuclear proliferation, rogue states and global terrorism. But another kind of threat lurks beyond our shores, one from nature, not humans – an avian influenza pandemic. An outbreak could cause millions of deaths, destabilize South-East Asia (its likely place of origin), and threaten the security of governments around the world
Announcing the establishment of the International Partnership on Avian and Pandemic Influenza (IPAPI) at the 2005 UN High-Level Plenary Meeting, then US President George W. Bush said: ‘It is essential we work together…to protect our citizens’ (White House 2005). The British Civil Contingencies Secretariat claimed that avian influenza is ‘as serious a threat as terrorism’ (Lean Reference Lean2005), and the disease still ranks highly on the UK's National Risk Register (Cabinet Office 2013: 7, 12). The WHO (Reference Heymann2007: 45) described H5N1 as ‘the most feared security threat’, while the World Bank (2008: 10) warned that ‘the virus remains a substantial threat to global public health security’. In 2006, a World Economic Forum report stated that ‘the global risk most preoccupying global business and political leaders is the H5N1 avian flu virus’ (WEF 2006: 2).
This discursive identification of an existential threat also translated into substantial monetary commitments, apparently confirming the CS's expectation that successful securitisation would attract emergency responses (Elbe Reference Elbe2010b). In 2005, the US government allocated US$3.8 billion in emergency funding to manage the threat of emerging and re-emerging infectious disease domestically and internationally. A total of US$334 million was earmarked for overseas programmes to combat H5N1 (State Department 2006). The justification given for this expenditure was that, ‘since pandemics are diseases without borders, the influenza virus will not respect political or geographic boundaries – a threat against one nation is a threat against the entire world’ (HHS 2005: H-60). These funds formed part of a total US$1.9 billion pledged at an international donors’ conference in Beijing in January 2006, US$1 billion of which was in grants. The European Commission pledged US$100 million in aid grants and US$20 million for research, while EU member-states individually contributed US$140 million in total (EU 2006). At another meeting in Mali in December 2006, a further US$475.9 million was allocated to the global fight against avian influenza, with the US making the biggest pledge (US$100 million), followed by Canada (US$92.5 million), the European Commission (US$88.2 million) and Japan (US$67 million) (Pellerin Reference Pellerin2006). The funds, according to the IPAPI plan, were to be used mainly for surveillance and prevention; preparedness, planning and outreach; and response and containment of avian influenza (HHS 2005: H-60). This represents a very substantial commitment of resources to tackle a single disease, considering that the WHO's total annual operating budget is typically just over US$1 billion.
Scholars exploring the securitisation of health have generated some very useful insights. They highlight the highly uneven nature of the securitisation of public health, which they attribute to the agendas and interests of governments in the global North (Davies Reference Davies2008, Reference Davies2010; McInnes and Lee Reference McInnes and Lee2006; Rushton Reference Rushton2011; Kelle Reference Kelle2007). Although concepts such as ‘global health security’ have gained traction within the WHO and elsewhere (e.g. WHO and Heymann Reference Heymann2007), the diseases identified as security threats are almost exclusively those with pandemic potential, especially those capable of ‘jumping scales’ rapidly, that is, moving from a local scale – typically in developing countries – to become global epidemics affecting wealthy states (Ali and Keil Reference Ali, Keil, Keil and Mahon2009: 195; see Rushton Reference Rushton2011: 780). The UN Secretary-General's High Level Panel on Threats, Challenges and Change (2004: 19) claims, for example, that infectious diseases should be considered a security concern because of their potentially unlimited reach, appealing to the ‘enlightened self-interest’ of Western governments: ‘the security of the most affluent State can be held hostage to the ability of the poorest State to contain an emerging disease’. However, endemic health problems, which kill millions of poor people within developing countries, such as malaria, dengue fever and tuberculosis, have generally not been securitised, nor allocated funding commensurate with the challenge.
As this book demonstrates, the argument that because new security problems easily cross borders they should concern governments and people far from their origins is not unique to infectious disease but common to all NTS issues. However, rather than recognising this commonality, health security scholars have incorrectly assumed that their field is unique and thus we are witnessing the ‘medicalisation’ of international security (Elbe Reference Elbe2010a). Instead of probing this commonality for insights into security governance more broadly, they have preferred instead to evaluate normatively the advantages and drawbacks of securitisation as a political strategy (e.g. Elbe Reference Elbe2006, Reference Elbe2010b; Davies Reference Davies2010; Enemark Reference Enemark2010). This again reflects the broader limitations of the CS, with its long-standing preoccupation with the merits of securitisation and desecuritisation (see Wæver Reference Wæver and Lipschutz1995, Reference Wæver2011; McDonald Reference McDonald2008). The CS emphasis on ‘speech acts’ has also led to an overwhelming focus on the intergovernmental level, where public pronouncements abound, rather than on how disease is governed in practice. Yet, discourse is frequently misleading; the language of ‘national security’ and ‘sovereignty’ is sometimes deployed even as extensive international intervention in domestic health governance is underway (Hameiri Reference Hameiri2014). What such interventions involve is missed when scholars confine themselves to, for example, judging that the securitisation of diseases like HIV/AIDS or H5N1 is negative because it reinforces ‘national security’ perspectives and thus zero-sum, combative logics rather than cooperation (Elbe Reference Elbe2006, Reference Elbe2010b).
Rescaling the governance of infectious disease
Fundamentally, what is missed is that because ‘national security’ in the global North is now taken to require the containment of diseases in the global South, security governance is acquiring an increasingly post-national form, involving efforts to rescale human and animal health governance where diseases originate and to integrate them within transnational regulatory frameworks for managing infectious disease. This shift, which Fidler (Reference Fidler2007) describes as a transition from international to global health governance, is reflected in the development of broad risk-management platforms for pandemic disease preparedness, such as the revised IHRs and the Pandemic Influenza Preparedness (PIP) framework, which the WHO coordinates. It is also reflected in specific attempts to contain particularly dangerous pathogens like SARS and H5N1.
The shift is clearly expressed in the evolving ISRs/IHRs (Fidler Reference Fidler2005). The first ISRs were created in 1851, following the 1830 and 1847 cholera outbreaks in Europe. Later revisions, like those issued in 1969, maintained an early focus on the management of international contact points – airports, border-crossings and ports – and only required governments to notify the WHO of outbreaks of six infectious diseases: cholera, plague, relapsing fever, smallpox, typhus and yellow fever (Fidler Reference Fidler2005). The WHO relied entirely on official information submitted by governments. However, the 2003 SARS outbreak proved an important catalyst for change. China's initial attempt to conceal the outbreaks and subsequent refusal to cooperate with the WHO for two months was widely seen to have enabled SARS to spread (Fidler Reference Fidler2003a; Abraham Reference Abraham2007; Stevenson and Cooper Reference Stevenson and Cooper2009). The international emergency response saw the WHO assume new coordinating functions vis-à-vis governments, and it unprecedentedly issued unilateral travel warnings (Kamradt-Scott Reference Kamradt-Scott2011). The World Health Assembly (WHA) subsequently demanded that the ‘inadequate’ IHRs be revised to more clearly specify the roles of governments and the WHO (Davies Reference Davies2012: 593). Accordingly, the 2005 IHRs focused attention on ensuring domestic health systems had the capacity to manage infectious diseases locally to protect health security globally. They specified the competences states must develop, including establishing disease-surveillance networks and reporting mechanisms, and installing laboratories and other core infrastructure. The revised IHRs, which are not confined to a specified list of pathogens, also authorise the WHO to obtain information from non-governmental sources and declare a Public Health Emergency of International Concern, triggering trade and travel warnings (Kamradt-Scott Reference Kamradt-Scott2011). Justified as necessary to manage the risks arising from transboundary disease, the WHO's new role is described as ‘further developing and maintaining an effective international system that is able to continuously assess the global context of public health risks and is prepared to respond rapidly to unexpected, internationally-spreading events and to contain specific public health threats’ (WHO n.d.b, emphasis added).
Crucially, this does not denote the WHO's emergence as a supranational authority, subordinating states to its will. Governments retain the right to reject WHO interventions if they wish, as some observers lament (Kamradt-Scott Reference Kamradt-Scott2011). Instead the WHO has become a locus of regulatory ‘meta-governance’, providing pandemic preparedness guidelines and standards for states to adopt in their domestic health systems, as well as a repository of public health expertise for states to draw upon when implementing the IHRs (Fidler Reference Fidler2007).
Indeed, far from developing autonomous supranational power, as constructivists might expect, the WHO's new role is substantially directed by powerful state interests. The new IHRs are not supported by additional funding to develop poor countries’ internal capacities (Bhattacharya Reference Bhattacharya2007). Rather, the WHO's core funding has declined steadily since the 1970s as donors like the US and the UK have shifted to funding specific projects on a case-by-case basis. Consequently, donors now control around eighty per cent of the WHO's total budget, as opposed to its rather meagre operating budget, deliberately bypassing the WHA, where Northern governments are outnumbered by poor developing states (Butler Reference Butler2013; Davies Reference Davies2010: 34–5; Chorev Reference Chorev2012). Donors have thereby redirected the WHO to focus on specific diseases that they find threatening to their security.
A further aspect of the rescaling of health security governance has been its expansion into hitherto disconnected policy areas, bringing in new agents and potential sources of contestation. This has partly been driven by the enhanced role of technical experts – in this case, public health experts, virologists and epidemiologists – in defining the nature of ‘threats’ within regulatory regimes. These experts are particularly concerned by zoonotic diseases, said to have comprised sixty per cent of all emerging infectious diseases from 1940 to 2004 (Scoones Reference Scoones and Scoones2010: 3). They include SARS, H5N1, H1N1 (‘swine flu’) and the Ebola, Nipah and Hendra viruses. Expert concern over this linkage between animal and human health has helped broaden health security to encompass the governance of animals, which is inevitably associated with agriculture and economic development. Since pandemic prevention and containment is now seen to require surveillance and response in wild, domestic and livestock animal populations, and because zoonosis is thought to be influenced by climate change and deforestation, the scope of ‘domestic health governance’ has expanded dramatically (see Coker et al. Reference Coker, Hunter, Rudge, Liverani and Hanvoravongchai2011). Commensurately, a bewildering array of governmental and non-governmental agencies and actors are increasingly incorporated into disease control systems, while the WHO itself cooperates with a wide range of agencies, such as the FAO, the World Organisation for Animal Health (OIE) and the World Bank, through the ‘One World, One Health’ agenda (FAO et al. 2008). This expansion of health governance has also given powerful interests associated with livestock and other agribusiness industries a strong, and often decisive, stake in the way that some infectious diseases are managed, as our cases studies now demonstrate (Vu Reference Vu2011).
The governance of H5N1 in Thailand and Indonesia
Southeast Asia was the centre of the last decade's H5N1 outbreaks. This densely populated, relatively impoverished region is often seen by scientists as one of the world's worst hotspots for infectious disease outbreaks. Rising human encroachment on natural habitats and the often close proximity between humans and domestic animals are said to greatly increase the risk of zoonotic diseases. Indeed, in late 2005, the WHO declared Southeast Asia would become the ‘next ground zero’ if the H5N1 pandemic were to materialise (Caballero-Anthony Reference Caballero-Anthony2008: 508; also Thomas Reference Thomas2006: 930). Southeast Asian governments appeared to agree that H5N1 posed a serious threat. In 2004, ASEAN leaders identified avian flu as one of the region's ‘key challenges’ (ASEAN 2004b). In 2007, they labelled it one of the top three transnational threats to regional security, stability and peace (ASEAN 2007b).
However, several commentators have noted a yawning gap between this urgent rhetoric and the actual response to the H5N1 outbreaks, which appeared lacklustre. They have emphasised the region's infamous attachment to national sovereignty – centrepiece of the so-called ‘ASEAN Way’ (Acharya Reference Acharya2009a) – as rendering it unable to formulate an adequate response to H5N1, as with other transboundary problems (Caballero-Anthony Reference Caballero-Anthony2008; Haacke and Williams Reference Haacke and Williams2008; Maier-Knapp Reference Maier-Knapp2011). This is fundamentally unpersuasive. As we demonstrate, deep international interventions did occur in Southeast Asia to rescale domestic health governance as part of the broader international effort to manage the disease, usually with the active support of national government ministries (Scoones and Forster Reference Scoones and Scoones2010; Hameiri Reference Hameiri2014).
This section provides two in-depth case studies of the response to H5N1 in Thailand and Indonesia, which managed the same disease in starkly different ways and generated divergent outcomes. The securitisation of H5N1 by international organisations and donor governments was used by central governments, in different ways and with varying degrees of success, to justify particular policy responses, as well as to legitimise their uneven consequences for different societal groups. The political economy of poultry production, and the poultry industry's relationship with governments at various levels, was the principal factor shaping these trajectories. In Thailand, the dominance of an export-oriented, highly industrialised poultry industry drove a centralised policy of tight biosecurity, which rendered small farms unviable and concentrated industry ownership in conglomerate hands. The Thai government's response was apparently effective, as no new human cases have been recorded since 2006 (WHO n.d.a). Conversely, in Indonesia, a more disaggregated and domestically focused poultry industry has perverse incentives to avoid regulation. Consequently, despite extensive externally driven governance rescaling, absent in Thailand's case, the governance response is ineffective because it was deflected towards the weakest group: poor villagers raising ‘backyard’ poultry, which were actually the victims of the disease circulating in commercial farms (Forster and Charnoz Reference Forster and Charnoz2013). Consequently H5N1 remains endemic among Indonesian poultry, although human infections have declined since 2006 (Forster Reference Forster and Scoones2010).
Thailand
The Thai response to H5N1 had two important features. First, while international experts were occasionally consulted and international regulatory standards were often invoked, Thailand's central government did not permit the direct involvement of international organisations and other agencies in the management of H5N1 outbreaks but instead monopolised its governance. It thus retained discretion over the manner in, and the extent to which, ‘best-practice’ guidelines from OIE, FAO and WHO were brought to bear on different stakeholders. Second, this discretion, particularly with regards to animal health, clearly favoured the interests of Thailand's large-scale, industrialised, export-oriented and vertically integrated poultry producers, at the expense of small producers and other interests groups, like cock-fighting enthusiasts and backyard poultry holders, spurring the sector's further industrialisation and concentration (Safman Reference Safman and Scoones2010).Footnote 1
Thailand's apparent success in containing H5N1 in humans, with no new cases since 2006, is often explained by the alignment between the medical imperative of reducing contact between humans and diseased poultry and major producers’ production methods, since their large-scale, integrated farms require only limited human–poultry contact. However, though little information is available on the circulation of H5N1 in commercial farms, the persistence of localised periodic outbreaks in poultry suggests it has shifted to an endemic pattern of infection (Meyer and Preechajarn Reference Meyer and Preechajarn2006; Safman Reference Safman and Scoones2010: 179; Thomas Reference Thomas2006). Indeed, contrary to industry claims and the assumptions inherent in the FAO's classification of poultry farming sectors, some evidence suggests that large-scale farms incubate disease, which then spreads to wild birds and backyard poultry (Davis Reference Davis2005; Bingham and Hinchliffe Reference Bingham, Hinchliffe, Lakoff and Collier2008: 189; Forster and Charnoz Reference Forster and Charnoz2013).
The Thai case demonstrates clearly that the rescaling of governance is a strategic move privileging particular societal interests over others. It also demonstrates that, despite the relativisation of scale associated with transnational security problems, governments retain an important role as ‘scale managers’, determining the kinds of international interventions permitted and the interests affected by them. Rather than reflecting a die-hard commitment to ‘sovereignty’, however, how this capacity is used is determined by particular contexts of state–society relations. To understand the context here, we must examine the political economy of the most affected industry.
The political economy of poultry production in Thailand
By the time H5N1 emerged in 2003, Thailand's poultry sector had become both heavily industrialised and politically well connected, defining the basic social power relations that subsequently shaped H5N1 governance.
Thailand's poultry sector had undergone significant transformation since the 1970s. Initially it largely comprised small companies raising chickens from local stock for domestic consumption. Charoen Pokphand (CP) – then a small animal feed producer – began importing breeding stock and selling day-old chicks (DOCs) to Thai farmers, who were contracted to raise them and sell back at an agreed price, before they were marketed to consumers. As production costs fell, large-scale producers like CP became competitive in export markets. By 2003, annual Thai poultry exports reached nearly US$1 billion and the sector contributed approximately four per cent of total agricultural GDP (Safman Reference Safman and Scoones2010: 182). Independent smallholders were increasingly replaced by contract farmers, who were themselves later dispensed with as the large corporations brought production in-house, with their share of output growing from thirty-three to fifty-seven per cent from 1993 to 2003 (NaRanong Reference Ong2006).
These vertically integrated farms are typically very large facilities housing over 10,000 birds. All production and processing is handled in-house, giving the company total control over cost and quality. Because production typically occurs in biologically isolated and highly mechanised environments, it is often argued – not uncontroversially (Davis Reference Davis2005; Bingham and Hinchliffe Reference Bingham, Hinchliffe, Lakoff and Collier2008: 189) – that these facilities better address biosecurity concerns than other forms of poultry production (Safman Reference Safman and Scoones2010: 205). Indeed, the emergence and dominance of these mega-farms were driven not only by concern to achieve economies of scale, but also by stringent regulatory standards demanded by important export markets like Japan and the EU, which were more achievable in vertically integrated facilities (Delgado et al. Reference Delgado, Narrod and Tiongco2003). In 1995, for example, the EU had threatened to ban Thai poultry imports following the discovery of banned additives in chickens raised by contract farmers (Burgos et al. Reference Burgos, Otte, Pfeiffer, Metras, Kasemsuwan, Chanachai, Heft-Neal and Roland-Holst2008). This was particularly critical given exporters’ shift to pre-cooked chicken products to realise higher profits. By 2003, such products comprised around a third of poultry export revenues; after the outbreak, they became exporters’ main commodity (Safman Reference Safman and Scoones2010: 185).
The poultry industry's growth and consolidation was accompanied by enhanced political influence. The major poultry producers are very well organised, fronting highly professional lobby groups like the Thai Broiler Processing Exporters Association. The industry's power at the time of the outbreak was also enhanced by political circumstances. The administration then in office, led by billionaire businessman Thaksin Shinawatra, was highly sympathetic to the interests of the Thai bourgeoisie, particularly in export-oriented industries. Thaksin's Thai Rak Thai party came to power in 2001 on the back of popular anger over IMF-imposed austerity following the Asian financial crisis of 1997–8. Thaksin developed a populist mix of pro-business and pro-poor policies, and Thai business elites were heavily represented in his government (Pasuk and Baker Reference Pasuk and Baker2004). This included the powerful poultry industry: Thaksin's Commerce Minister, Watana Muangsook, is the son-in-law of CP founder and chief executive officer, Dhanin Chearavanont, who Forbes Magazine (2 December 2010) identifies as Thailand's wealthiest person.
Consequently it is unsurprising that ‘[a]t numerous points during the epidemic, decisions taken by Thai officialdom clearly reflected direct input from and/or collaboration with the industry lobby’ (Safman Reference Safman and Scoones2010: 182). Indeed:
While it is self-evident that any country with such a large and economically vibrant industrial poultry sector would go to great lengths to preserve and protect that sector's interests, it is not clear that Thailand's effort need have been implemented in a manner that was so costly to the smaller producers who, while economically less influential, were (and are) nevertheless quite numerous…the Thai government consistently and almost unilaterally sided with the large-scale producers, making only token concessions…to small-scale commercial and non-commercial interests
As we shall see, the tight state–industry relationship profoundly shaped the governance of H5N1 as a non-traditional security issue.
Thailand's governance response to H5N1
The Thai government's response was principally shaped by the desire to defend the export markets of the politically and economically powerful large-scale poultry producers. In pursuit of this goal, the government mobilised international regulatory standards, but concentrated power in state hands rather than permitting extensive governance rescaling through the direct involvement of international actors. This isolated opponents of the government's response from external allies who may have been more sympathetic to their plight, benefiting the large producers.
Although H5N1 first appeared in Thailand in late 2003, the Thai government officially admitted this only in January 2004, as the outbreaks became widespread and the first human victims died (Thomas Reference Thomas2006: 924–5). The government was immediately accused, both by domestic political rivals and internationally, of attempting to conceal the disease to protect Thailand's poultry exports. This was not unwarranted, since the EU and Japan – Thai poultry's biggest export markets – plus Hong Kong, the Philippines, Singapore, Myanmar and Cambodia immediately imposed import bans (Bangkok Post 24 January 2004). These were maintained for raw meat until 2008, but even cooked meat products were given only limited access to European and Japanese markets from late 2005 (Safman Reference Safman and Scoones2010: 175).
Following the revelation, the Thai government took swift, decisive action to eliminate H5N1, vigorously publicising these efforts to reassure domestic and international consumers. Although its response resembled the emergency measures that CS adherents expect, it actually involved the ruthless application of international regulatory guidelines provided by the FAO, WHO and OIE, again illustrating how security governance has become more internationalised, bureaucratised and technical. The measures taken included: comprehensively culling poultry from all farms within a five-kilometre radius of confirmed outbreaks, disinfecting affected facilities, and restricting movement within a fifty-kilometre radius of outbreak sites. Importantly, however, this application of international ‘best practice’ was not simply neutral, but was rather enabled by and reflected the interests of the large-scale, export-oriented segment of the poultry industry. The culling policy immediately imposed a disproportionate burden on small- to medium-sized farms, where most of the sixty-two million birds culled were located (Safman Reference Safman and Scoones2010: 175). Similarly, the Thai government's follow-up measures to regularise its response to H5N1 and develop better surveillance and outbreak preparedness favoured industrial players. Three new regulatory requirements were introduced: a ban on vaccinations, controls on the movement of poultry, and the compartmentalisation of facilities. While most of Thailand's mega-farms already complied with these rules, the adjustment cost for small farmers was often unbearable. Many thus ‘decided to close down their operations entirely, making the period from 2005 to 2006 a period of significant consolidation and restructuring within the Thai poultry sector’ (Safman Reference Safman and Scoones2010: 180).
The vaccine ban is an area of major difference between the Thai and Indonesian cases; while Indonesia promoted vaccinations, the Thai government refused to permit the vaccination of birds, even of fighting cocks – a popular sport in the country. This decision was justified by invoking the OIE Manual, which recommended mass culling and disinfection rather than vaccination (Scoones and Forster Reference Scoones and Scoones2010: 26–7). The more pressing reason was that the EU and Japan had banned imports of vaccinated chicken products (Leboeuf Reference Leboeuf2009: 51). The decision prompted outrage among small-scale farmers and fighting cock owners. To manage this, the government formed a national committee to investigate the viability of vaccination in July 2004, between the first and second waves of H5N1 infection. However, again citing scientific evidence and best practice, the committee maintained the policy, claiming that vaccination, particularly if incomplete, would only spur H5N1's evolution into a more dangerous pathogen. Government and industry representatives then used these findings, along with OIE standards, to justify the vaccination ban (Safman Reference Safman and Scoones2010: 187). Despite the appearance of neutral, technical rationality, this again reflected big producers’ interests. Many large-scale farms were reportedly using the same vaccines to immunise hens used to produce eggs – which are marketed domestically, not exported – but no government ban was imposed here (McSherry and Preechajarn Reference McSherry and Preechajarn2005).
Poultry movement controls and their uneven implementation also showed how the same powerful interests shaped the design and operation of the governance regime. Again invoking OIE regulations, a June 2004 law specified that no susceptible animals could be transported from or through an area within ten kilometres of any H5N1 outbreak for ninety days without special permission from local animal health authorities. The burden of this new regulation fell heavily on small farms and cock-fighting enthusiasts since, as the mega-farms were increasingly vertically integrated, with all stages of production co-located, their need for movement was low (Safman Reference Safman and Scoones2010: 189). When movement was needed, their resources and clout meant they could more easily acquire permits than small farms and fighting cock owners, who endured long waiting periods. Cock-fighters were reduced to bribing local officials to smuggle birds through quarantine zones, though eventually a compromise was found in the form of travel ‘passports’ for their birds (Safman Reference Safman and Scoones2010: 194).
Finally, the concept of compartmentalisation also advanced the interests of large-scale producers. First introduced by the OIE in the mid 1990s, compartmentalisation allows the recognition and certification of different sectors based on distinctive production circumstances. It allowed for producers that met biosecurity and handling standards to be certified as fit to export, while denying certification to others. Pushing this approach suited large-scale producers, since they had been segmenting the poultry sector since the 1990s. To pursue this approach, the Thai government permitted a modest degree of governance rescaling, allowing the OIE to independently regulate Thai regulators from the Ministry of Agriculture. Japan and the EU accepted this approach in 2007 and 2008, respectively, and certificates were swiftly issued to CP and one other major corporation, although no raw meat has yet been sold under this scheme (Meyer and Preechajarn Reference Meyer and Preechajarn2006; Safman Reference Safman and Scoones2010: 190; Ratananakorn and Wilson Reference Ratananakorn and Wilson2011).
Thailand's response to the security threat of H5N1 was thus clearly shaped by powerful economic interests. The Thaksin government's primary goal was the defence of the politically connected industrial sector's export markets, and all other sectors’ interests were subordinated to this. Had the large-scale producers’ interests been different, the application of international regulatory standards would arguably have been far less stringent – as the case of Indonesia clearly suggests.
Indonesia
Indonesia has been hit harder by H5N1 than any other country, with the highest number of human deaths and the greatest amount of international assistance to combat the disease. Unlike Thailand, where the government largely excluded international actors while selectively implementing international regulatory standards, in Indonesia, the FAO, WHO, other UN agencies and bilateral donors have been heavily involved in designing, funding and implementing large-scale programmes of surveillance, culling, vaccination and risk communication, together with national government agencies (Lowe Reference Lowe2010). The most significant and best-funded development has been the rescaling of local animal and human health agencies to provide permanent grassroots surveillance of H5N1 outbreaks and to respond where necessary. Initiatives like the Participatory Disease Surveillance and Response (PDSR) project in animal health and the District Surveillance Officers (DSO) project in human health often created local health services and established new governance networks across the local and national scales in Indonesia, which were hitherto frequently weak or non-existent. International agencies also improved laboratories’ diagnostic facilities and the capacity of hospitals across Indonesia to treat avian flu patients. Nevertheless, although the incidence of human infections declined from its peak in 2006, people continue to be infected every year to 2013, and the disease remains endemic among poultry in Indonesia's most populous islands, Java, Sumatra, Bali and Sulawesi, with sporadic outbreaks reported elsewhere (Forster Reference Forster and Scoones2010: 131). To understand both why Indonesia's reaction to the exact same NTS threat diverged so much from Thailand's and why it was so ineffective, we must understand the specific power relations shaping the governance response, notably the very different relationship between local and national political scales and the political economy of its poultry industry.
The political economy of poultry production in Indonesia
In Indonesia, a poultry industry, which produces exclusively for domestic consumption and in which the big and dominant conglomerates profit from selling production inputs to small, independent farmers, has had little interest in applying costly international standards of biosecurity and disease eradication. Meanwhile, government decentralisation has enabled powerful players in the poultry industry to keep the governance of animal health at the local level and in the hands of industry-friendly officials.
The decentralisation of the Indonesian state, described in detail in chapter three, had two major implications for infectious disease management. First, international donors concerned with managing H5N1 have had to develop multilevel governance approaches that engaged directly with local-level governments, since significant authority had been delegated to them. This has spawned new governance networks designed to connect particular government agencies across various scales, with donors acting as coordinators. The second implication of decentralisation is that proponents and opponents of rescaling have clustered around the national and local governmental levels, respectively. Those trying to resist the international regulation associated with rescaling have sought to keep governance at the district or provincial level and in the hands of local livestock services officials (Charnoz and Forster Reference Charnoz and Forster2011). Conversely, central government ministries have selectively embraced international rescaling to benefit from additional funding and bolster the territorial and functional reach of their diminished authority (Hameiri Reference Hameiri2014; Forster and Charnoz Reference Forster and Charnoz2013). They also seek to blame decentralisation for their failures in managing H5N1. Indonesia's former health minister, Dr Siti Fadilah Supari, for example, argued:
Vietnam, as a centralised socialist country, can get high compliance on national policies and so has succeeded, for example, in implementing rapid culling of birds…In contrast, Indonesia is in transition towards a decentralized democracy after three decades of authoritarian national rule. We are still on a learning curve, and compliance of the relatively independent regional authorities with national policies is often poor
Decentralisation has also shaped the political economy of Indonesia's poultry industry. Chicken is Indonesia's favourite meat and is a very important source of protein, particularly for poorer people (Sumiarto and Arifin Reference Sumiarto and Arifin2008: 7). The poultry sector is also very significant economically. The livestock sector as a whole, of which the poultry industry is by far the biggest component, contributes about 1.8 per cent of total GDP in Indonesia and it grew at an average rate of 4.47 per cent per annum between 2001 and 2006, the period immediately before and during the H5N1 outbreaks. Poultry farms are also the largest employers within the livestock sector, which collectively employs three million people, around three per cent of the national workforce (Sumiarto and Arifin Reference Sumiarto and Arifin2008: 6).
Beyond these headline figures, however, Indonesia's industry is organised very differently to that of Thailand, and this has critically shaped the governance response to H5N1. Ostensibly, Indonesia's sector is also highly concentrated, with the ten largest poultry producers controlling all industrial production and eighty per cent of total output (Charnoz and Forster Reference Charnoz and Forster2011: 21). The largest three producers, of which the Indonesian subsidiary of Thai multinational CP is the biggest, have a combined market share of seventy per cent (Sumiarto and Arifin Reference Sumiarto and Arifin2008: 10). However, unlike Thailand, where production now largely occurs in vertically integrated mega-farms, Indonesia's situation is closer to Thailand in the 1970s and 1980s. The large-scale companies dominate the supply of farming inputs, but production is almost entirely outsourced to thousands of small and medium farms – the ‘nucleus–plasma’ arrangement also found in palm oil (see chapter three). Essentially, the ‘nucleus’ companies provide inputs on credit to the ‘plasma’ farms – or ‘Sector Three’ – which raise the chickens for 28 days, then sell them back to the ‘nucleus’ at pre-agreed prices. The large companies then market the chickens solely to domestic consumers. This structure was introduced to the sector in 1996, ostensibly to assist small, local agricultural businesses to develop. In reality, it was highly advantageous to powerful interests associated with the Suharto regime, which dominated the nucleus companies, and it helped expand centre-dominated patronage relations (see McCarthy Reference McCarthy2006 in the palm oil context). The arrangement also allows the nuclei to extract enormous profits, up to ninety per cent of which come not from retailing chickens, but rather the oligopolistic sale of inputs – primarily DOCs and feed – to Sector Three farmers, who lack alternative sources of credit to purchase them from elsewhere (USAID 2009: 19–20; Charnoz and Forster Reference Charnoz and Forster2011: 32). Sector Three farmers are thus forced into permanent dependence on the large companies and operate on tiny profit margins.
This highly exploitative structure carries significant implications for the incidence and management of H5N1. Sector Three farms, where most production actually occurs, are usually very small, basic facilities. They typically house between 500 and 5,000 birds and cannot afford the hi-tech methods and biosecurity measures deployed by Thailand's mega-farms. Many lack adequate walls to separate chickens from the surrounding environment, protective gear for farmers, or showers they can use upon entering and exiting the facility (Sumiarto and Arifin Reference Sumiarto and Arifin2008; USAID 2009). Furthermore, under standard industry contracts, farmers are not paid for dead chickens. The large corporations consequently have little exposure to the risk of poultry deaths as a result of diseases like avian influenza – barring a mass consumer boycott, which has not happened to date – and are thus likely to be indifferent about it. Adding to the large corporations’ complacency is the fact that despite the outbreaks and mass chicken deaths, because of sharply rising demand for poultry products among Indonesians, Indonesia's poultry population actually grew by seven to fifteen per cent annually at the height of the H5N1 scare between 2006 and 2008, while industrial production as a whole has grown by nearly tenfold over the decade to 2009 (Forster and Charnoz Reference Forster and Charnoz2013: z). Conversely, hard-pressed farmers have every incentive to conceal outbreaks and even sell dead, diseased chickens via brokers. Due to widespread poverty, Indonesia has a thriving market for chickens that died of unnatural causes, which are sold at discounted prices (Brum Reference Brum2011). These perverse incentives clearly impede the management of H5N1 (see also McLeod Reference McLeod2010).
This might change if the industry became vertically integrated, as in Thailand, but a government–business pact apparently precludes this. For the central government, vertical integration is not politically palatable because, by killing off smaller farms, it would generate significant unemployment (Forster and Charnoz Reference Forster and Charnoz2013; Delima Reference Azahari2011; McGrane Reference McGrane2011). The government has thus apparently struck a bargain with the larger firms, who agreed not to vertically integrate their operations in exchange for continued protectionist measures against imports of agricultural inputs and chicken meat (Mulyanto Reference Mulyanto2011). Indeed, only 0.28 per cent of the poultry products consumed in Indonesia are imported (Sumiarto and Arifin Reference Sumiarto and Arifin2008: 6), and no chicken meat has been imported into Indonesia since 2000. Imported meat would be significantly cheaper than domestic produce, because sophisticated production technologies used in countries like Thailand reduce costs, whilst the massive profit margins extracted by Indonesia's conglomerates on farming inputs inflates them. As Ministry of Agriculture (MoA) officials put it, imports ‘are cheaper. If it comes in, the market will collapse’ (Azhar and Noeri Reference Muhammad and Widowati2011).
Accordingly, the large corporations are disinterested in either changing the industry's structure or improving biosecurity measures to help tackle H5N1, while Sector Three farmers are simply unable to do so. When the ‘nucleus’ firms were engaged by the USAID-funded Community-Based Avian Influenza Control (CBAIC), one of very few international projects to directly target the private sector, their representatives acknowledged biosecurity needed improving in Sector Three, but made few commitments to fund this. CBAIC instead focused on training farmers in basic biosecurity – washing hands, disinfecting coops – as if the main problem was the ignorance of farmers. Far more important is the fact that Sector Three farmers lack the capital to invest in biosecurity and cannot obtain loans from banks, the large corporations or the government for this purpose. The president of the Indonesian Poultry Farmers Association and Information Centre, which represents Sector Three farmers, insists:
We can control [avian influenza]. Sector Three's problem is only money…Farmers can't make the investment – why [doesn't] the government give us money?…We want soft loans. It is very hard to get credit from banks to invest in biosecurity…It is very expensive: to build a fence around ten hectares – 100,000 square metres – is one billion rupiah [$91,000]
The FAO's Eric Brum (Reference Brum2011) adds: ‘We would've expected the commercial sector to be more willing to allocate resources to ultimately control the disease, but…it's really become an industry that's built around mitigating losses from disease, as opposed to properly controlling and eliminating diseases which decrease production’.
Together, the structural environment of decentralisation and the industry's political economy have underpinned a radically different response to managing H5N1 in Indonesia to that in Thailand. The large corporations’ lack of exposure to the risks of disease and their ability to evade regulatory intervention through the decentralised health governance system has meant that the commercial sector has managed to avoid scrutiny, while poor owners of ‘backyard’ poultry bore the brunt of the regulatory response.
Indonesia's governance response to H5N1
Avian influenza was never a high priority for the Indonesian government, but with international pressure mounting and with large amounts of donor funding in the offing, the government developed a national disease mitigation plan and established governance mechanisms dedicated to this. The political economy context just described allows us to make sense of the objectives of international rescaling efforts and their highly uneven outcomes. Although some rescaling of health governance has been permitted, largely to improve central oversight of local governments, the Indonesian government nonetheless sought to deflect attention from the commercial sector, towards ‘backyard’ poultry, which was in fact a victim of the disease's circulation in farms (Forster and Charnoz Reference Forster and Charnoz2013).
The Indonesian government's response to H5N1 reflected the industry's interests from the outset. It initially sought to conceal the emergence of H5N1 in Indonesian poultry in late 2003, apparently under pressure from major industry players, who were afraid it would hit sales (Sipress Reference Sipress2005). Chicken deaths were instead attributed to Newcastle disease, which has similar symptoms as H5N1 in poultry but no zoonotic capacity. The presence of H5N1 was only admitted in January 2004, but MoA officials initially maintained that the Indonesian strain was incapable of zoonotic transmission. The central government also attempted to pass the responsibility for managing the disease to local governments (Curley and Herington Reference Curley and Herington2011: 156–7). However, after a spike in human cases in 2005, international and domestic pressure on the national government to act became overwhelming. Indonesian government officials and international consultants thus crafted the H5N1 National Strategic Work Plan (NSWP) 2006–8. This identified nine core objectives for H5N1 eradication, highlighting ‘backyard’ poultry – ‘Sector Four’ – as a particularly important vector for the disease's spread and zoonotic transmission (Perry et al. Reference Perry, Isa and Tarazona2009). Although the plan mentioned restructuring the commercial sector, this was not identified as a priority or allocated any resources. The NSWP thus embedded industry interests and the state–business pact described above.
However, the governance structures subsequently established created new networks between many national governmental agencies and funding requirements provided an entry point for international actors. A National Committee for Avian Influenza Control and Pandemic Influenza (Komnas FBPI in the Bahasa Indonesia acronym) was established to implement the NSWP. Led by the Coordinating Ministry for People's Welfare, Komnas FBPI included the ministers for health, agriculture, forestry, national planning and industry, the Coordinating Minister for Economics, the commander of the armed forces, the police chief and the chair of the Indonesian Red Cross. It had a secretariat and six task forces containing scientists and other experts, which were to provide direction on research and development, animal health, human health, vaccines, anti-viral medicines, mass communications and public information (Forster Reference Forster and Scoones2010: 145). The NSWP specified that US$322 million would be needed over three years to manage H5N1, part of which would be provided by donors (Charnoz and Forster Reference Charnoz and Forster2011: 72). International contributions were thus sought at the aforementioned Beijing meeting in January 2006. However, because operating budgets remained with relevant government bodies, it was through them that international agencies became involved.
Despite this apparent securitisation and emergency response, it is clear that the H5N1 agenda was largely driven by external rather than domestic interests, reflecting the broader orientation of ‘global health security’ towards defending societies in richer countries from disease outbreaks in the global South (Rushton Reference Rushton2011). That H5N1 was not a domestic priority is suggested by the fact that only US$57 million, or 1.7 per cent of the national health budget, was allocated to controlling the disease at the peak of the crisis in 2006–7 (Curley and Herington Reference Curley and Herington2011: 157). Similar disinterest is reflected in the bizarre claim that H5N1 was not actually zoonotic, made by Indonesia's then health minister, who stated: ‘there's no relationship between human virus and chicken virus. There's no possibility of human to human transmission because it is very different’ (Siti Reference Supari2011). Such nonsense aside, clearly H5N1 was just one problem among many facing this impoverished country. As one high-ranking Ministry of Health (MoH) bureaucrat (Anonymous 2011c) says, ‘we have so many diseases – all of the diseases are a priority’. The focus on H5N1 was donor driven, the health minister's special advisor explained (Indriyono Reference Tantoro2011). This is underscored by the government's growing disinterest in the disease after international pressure and assistance waned from 2009. Dr Emil Agustiono (Emil Reference Agustiono2011), who heads Komnas Zoonosis, which succeeded Komnas FBPI and now seeks to replicate its work across all existing and potential zoonoses, observes: ‘the previous one [had] a lot of assistance from donors. The current one [Komnas] has no donor funding…Compared with a couple of years ago, national priority is not there’. Indeed, in July 2011, more than a year after it was established, Komnas Zoonosis was entirely unfunded. Emil laments: ‘I wish the pandemic will come again so we are able to exercise our plan!…We don't have enough vaccines. We don't have enough capacity.’ The real reason why the national government embraced global health security interventions was apparently an instrumental one: to help strengthen its hand against local governments. H5N1 donor programmes helped forge new governance networks both horizontally and vertically. A senior MoH official argues this helped Indonesia's health system by networking the MoH with other ministries through Komnas FBPI and in particular facilitating better collaboration with the MoA, creating direct links at the directorate-general level and collaboration in the field, with joint investigations of suspected outbreaks (Anonymous 2011c). However, far from merely yielding technical improvements, international funding also empowered national-level agencies, relative to their local counterparts. As the minister of health's special advisor recalls, donor interventions to improve ‘pandemic preparedness…helped the centre have a bit more control over provinces and districts, particularly if we have the money…We can advocate and convince them…Resources are always a problem at the local level’ (Indriyono Reference Tantoro2011). Similar efforts to use international funding to help recentralise authority occurred within the MoA, although the ministry also invoked local governments’ resistance to explain both the policies adopted and implementation difficulties. For example, Delima Azahari (Delima Reference Azahari2011), Director-General of Agricultural Quarantine and Manager of the Emergency Centre for Transnational and Asymmetric Threats at the time of the initial outbreaks, argued: ‘Local governments were a problem. We can't do anything without the help of local governments.’
Notwithstanding this instrumental support for governance rescaling from national-level agencies, in practice, the regimes that emerged were heavily conditioned by the political economy of poultry production and resistance to rescaling at the local level. We can illustrate this by examining one programme in detail.
Rescaling local health governance: the PDSR project
The implementation of international programmes for managing H5N1 in Indonesia reflects the political economy context of poultry production and state–industry relations that also shaped the NSWP. While ‘backyard’ poultry was subjected to considerable rescaling, through large-scale surveillance, response and public education campaigns, the commercial industry was left almost entirely untouched and its involvement in H5N1 eradication has so far been wholly voluntary.
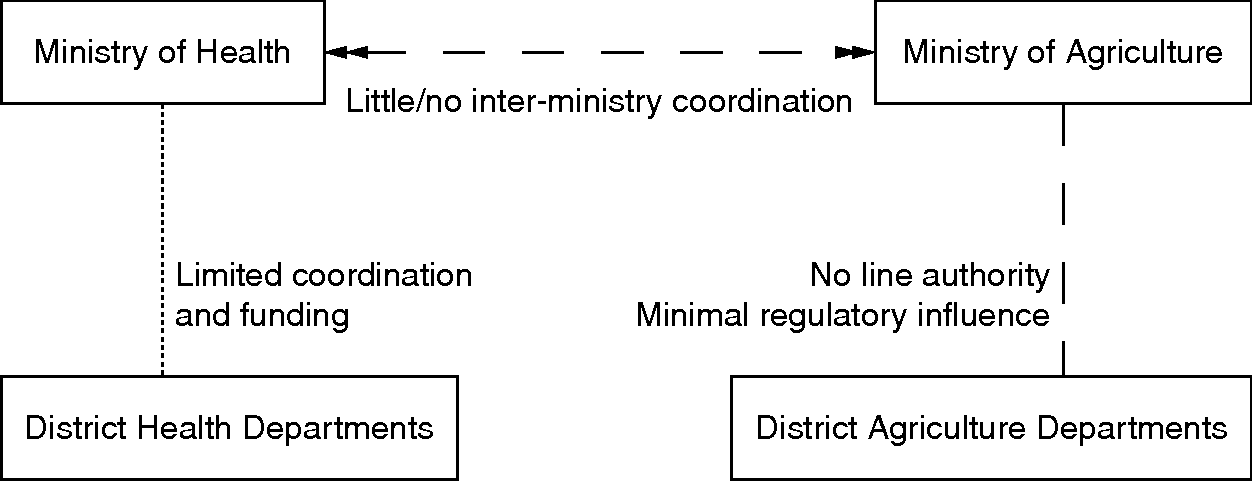
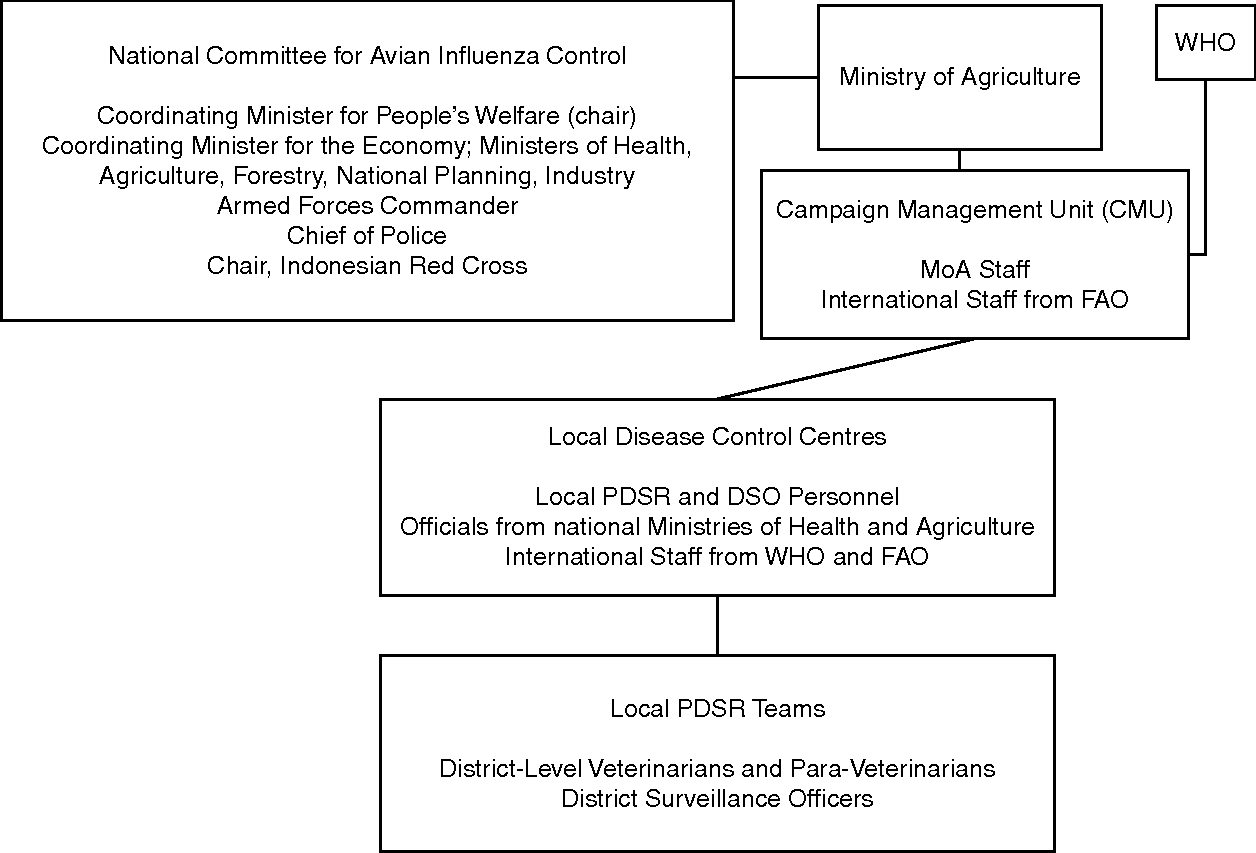
The two most significant, internationally funded projects to manage H5N1 in Indonesia were the FAO-managed PDSR and the WHO-managed DSO, with the PDSR's perceived success heavily influencing the DSO's design (see Figures 4.1 and 4.2). This section focuses mainly on PDSR since it was much bigger, with a budget of approximately US$30 million between 2005 and 2012, provided mostly by USAID and the Australian Agency of International Development (AusAID), and it clearly reveals the forces shaping the governance of this NTS threat. The PDSR and DSO both sought to shift local health governance ‘upwards’, to the regional and national levels, and ‘sideways’, into the hands of like-minded experts who would implement international regulations. This created a complex, multilevel governance system that was substantially internationalised, with rescaling occurring at multiple levels simultaneously.
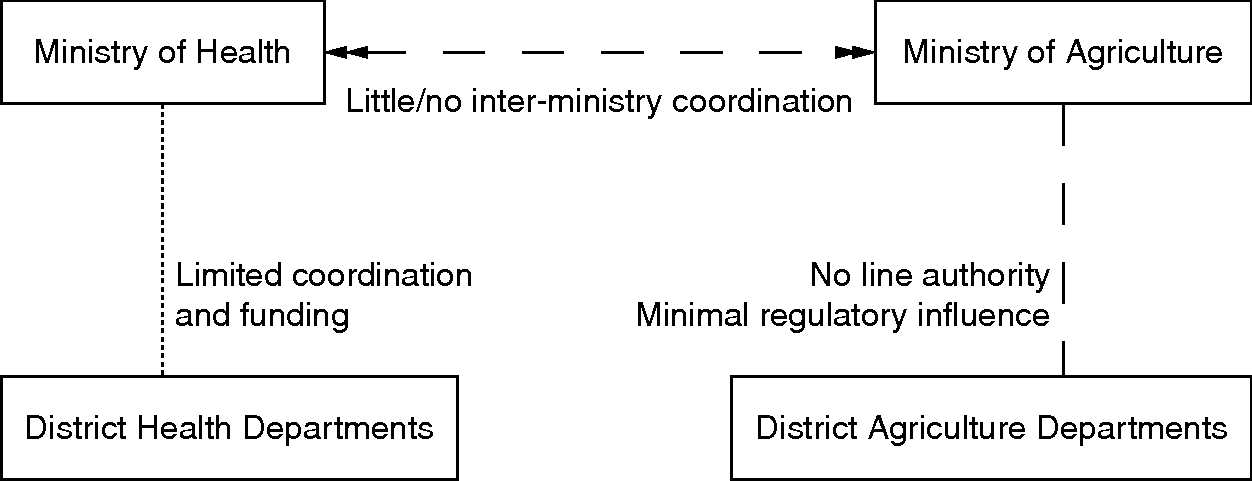
Figure 4.1 Indonesian health governance before the PDSR intervention.
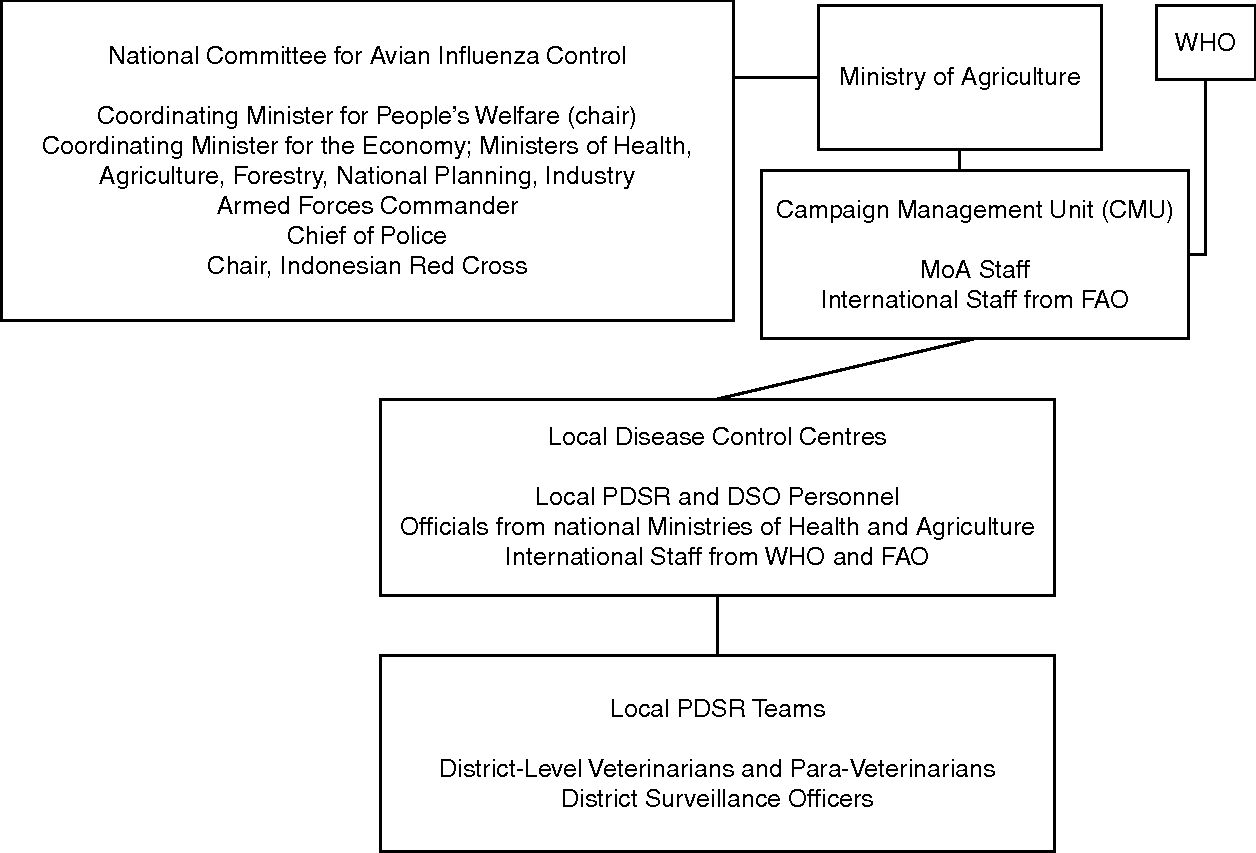
Figure 4.2 Indonesian health governance following the PDSR intervention.
At the local level, the PDSR and DSO programmes often created health governance systems where none had hitherto existed. These programmes essentially involved training and empowering veterinarians and health officials to conduct local surveillance to detect H5N1 outbreaks and educate local populations on the risks of transmission. Although PDSR officers were officially employed by local Dinas (local government departments), until late 2011 their salaries were funded by the FAO, with local governments supposed to assume responsibility from 2012. The PDSR's scale at the local level was vast:
From January 2006 to September 2008, PDSR teams, comprising over 2000 trained veterinarians and para-veterinarians, conducted over 177300 surveillance visits, detected 6011 outbreaks of avian influenza in 324 districts, and met with over two million poultry farmers and community members…In May 2009, there were fifteen international and sixty national staff/consultants employed by FAO, with a majority of them supporting the PDSR programme
At the provincial level, Local Disease Control Centres were established. District-level PDSR staff reported suspected outbreaks to these centres, which brought local PDSR and DSO personnel together with national officials from the MoH and MoA, plus international officials from the FAO and WHO. The centres mobilised rapid response teams to investigate reported outbreaks and respond as required. They also rapidly reported their findings to the FAO and WHO. At the national level, the PDSR system was coordinated by a Campaign Management Unit (CMU) within the MoA's Directorate-General of Livestock Services, which FAO consultants helped design and staff. The CMU was meant to coordinate its activities with Komnas FBPI.
This multilevel design, with donors working with and coordinating both local- and national-level agencies, was necessitated by decentralisation. As an FAO official explained: ‘The central government has little or no outreach. We therefore work though Dinas locally’ (McGrane Reference McGrane2011). Another FAO advisor puts it more bluntly: ‘the national government has no authority to do anything…We couldn't get the national government to tell [district and provincial governments] to do it, so we had to go to the local level’ (Brum Reference Brum2011). CMU officers concurred: ‘The functional link between central, provincial and district governments was previously constrained during the decentralisation era. We can bridge the gaps’ (Azhar and Noeri Reference Muhammad and Widowati2011). Consequently, the PDSR ‘has been active in facilitating the relationship between national and local government’ (Brum Reference Brum2011), spawning new functional networks linking Indonesia's various levels of government in the management of H5N1. This was particularly important in agriculture, where since decentralisation there was little coordination between the MoA and local Dinas.
Crucially, the PDSR also sought to shift authority ‘sideways’ to empower veterinarians over other local officials. Enhancing veterinary authority was seen as essential for embedding OIE and FAO standards in local governance. Such attempts to empower technical experts are a common aspect of NTS rescaling, aimed at quarantining policymaking areas from political control. However, empowering veterinarians proved very difficult. There are few trained veterinarians in Indonesia and at every level of government they have worked under managers with backgrounds in animal husbandry or agricultural economics, who are typically more concerned with commercial aspects of livestock services than with animal health. Within the MoA, for example, animal health was until recently only a Directorate within the Directorate-General of Livestock Services. Its powerlessness within the MoA was exemplified by a turnover of four directors in three years, as the government developed its response to H5N1.
The difficulty encountered in changing this situation clearly stemmed in part from political economy constraints. One director of animal health who left the MoA was reportedly dismissed because she wanted to implement widespread culling in H5N1 outbreak areas, the OIE-sanctioned procedure for managing the disease's spread in poultry, rather than the industry's preferred vaccination policy (Charnoz and Forster Reference Charnoz and Forster2011: 91; Lowe Reference Lowe2010). Unlike in Thailand, Indonesia's big industry players preferred vaccination since, because they did not export chicken, they did not have to worry about meeting EU and Japanese regulations. Moreover, alongside pharmaceutical companies, they could actually increase their profits by producing and selling vaccines. At one point, Indonesia had thirty-five to forty poultry vaccine manufacturers, and the industry was very poorly regulated, with some farmers being sold H5N2 instead of H5N1 vaccines, for example (Suwandono Reference Agus2011; Heru Reference Setjanto2011). Vaccinating chickens is also notoriously difficult: every chicken must be vaccinated three times to acquire immunity and whole flocks must be vaccinated six times each year. It is practically impossible to vaccinate broiler chickens since they are grown for only twenty-eight days. Smaller farmers and villagers also opposed culling, since they do not receive income for dead chickens and meagre government compensation was provided infrequently. Consequently, no one supported culling apart from some government veterinarians, who were swiftly overruled.
The weakness of veterinarians was exacerbated by the absence of structures linking animal health practitioners across different levels of government. In human health, despite the localisation of about eighty per cent of the budget to the district level under decentralisation, the pre-existing line structure linking the MoH to local Dinas Kesehatan (human health departments) was largely maintained. However, this was not the case in animal health, for which there was no dedicated Dinas in almost every province and district. Animal health services were generally under departments of agricultural services (Dinas Pertanian) or livestock services (Dinas Peternakan). Furthermore, in some cases wild animals are managed by the forestry Dinas, fish by the fisheries Dinas and domestic animals by the agriculture Dinas. Generally these departments do not have veterinarian leadership, or even input. Funding for local animal health services is currently entirely at the discretion of the bupati (district regent) or mayor, who tend to view it as a dispensable service, and often there is only one vet to serve an entire district (Normile Reference Normile2007; Andri and Riana Reference Jatikusumah and Arief2011). This fragmentation and marginalisation of animal health reflects the fact that, unlike human health, agriculture is a very important source of rents and patronage resources. In the context of growing electoral competition at all levels, control of key industries has become essential to attaining and keeping political power in most Indonesian jurisdictions. Reflecting this wider pattern of inter-scalar conflict in post-decentralisation Indonesia (Hadiz Reference Hadiz2010), bupatis have sought to grab control of agriculture and isolate its governance from both interference by veterinarians and the national authorities in order to capture these resources for themselves. As Professor Wiku Adisasmito (Reference Adisasmito2011), a former member of Komnas FBPI, explains: ‘human health is more integrated vertically but in animal health this is not the case because of local economic structures’.
Like national-level officials, Indonesian veterinarians tried to exploit the rescaling of H5N1 governance to enhance their power. The Indonesian Veterinary Medical Association (IVMA) in 2004 launched a campaign to re-establish veterinary authority over livestock services across all levels of government. Veterinarians have long resented being managed by officials with no concern for animal health who forced them to support animal production services instead of regulating them. Vets typically consider themselves as ‘professional’ and ‘independent’, unlike animal husbandry experts who are seen as ‘political’ or ‘entrepreneurs’ (Charnoz and Forster Reference Charnoz and Forster2011: 49, 51). They also perceive themselves as part of a transnational professional community working to implement international guidelines for the public good. As one insisted, ‘we need authority to implement the norms of OIE’ (Charnoz and Forster Reference Charnoz and Forster2011: 47). The IVMA thus used high-profile issues like H5N1 to demand greater autonomy (Wiwiek Reference Bagja2011). The IVMA's vice president explained its objectives in terms often used by those advocating the rescaling of governance: ‘Disease knows no borders. That's why the Vet Association fights over…the animal health system, to make it at least the same as the health system…We want to be able to issue regulations from the centre [that] they [the districts] will have to work with’ (Heru Reference Setjanto2011). Similarly, other veterinarians working with international projects demanded that ‘farmers…should be forced to report’ outbreaks to enable veterinary intervention (Andri and Riana Reference Jatikusumah and Arief2011).
This campaign had some success, but in practice veterinary authority remains limited. After decades of wrangling, IVMA's efforts, combined with the threat of H5N1, finally spurred parliament to pass National Law 18/2009 on Animal Husbandry and Veterinary Hygiene in May 2009. Whilst still not up to OIE standards, the legislation transformed the DGLS into the Directorate-General of Livestock Services and Animal Health, and mandated the establishment of animal health Dinas countrywide, to be linked and coordinated nationally. The IVMA contested the law in the Constitutional Court, arguing that ambiguity in Article 68 still subjected veterinarians to discretionary control by the Minister of Agriculture. The Court ruled in its favour, deleting the ambiguity (Charnoz and Forster Reference Charnoz and Forster2011: 52). This was seen as a major victory for veterinarians. However, the law's implementation has been very slow. No implementing regulations have been issued, no funding allocated and no central veterinary authority has been created. The head of the DLGS, who was, for the first time in many years, a veterinarian, was sacked for supposed ‘incompetence’ in mid 2011 after just six months in post. Meanwhile, local governments retain considerable autonomy over animal health and, since the mandated new Dinas rely on local funding, they are at liberty to underfund them. Thus, as IVMA President Dr Wiwiek (Reference Bagja2011) observes: ‘in law, we are strong enough, but to have the law really implemented and in line with OIE guidelines, we need political will’.
However, political will to support veterinary authority has not been entirely absent; rather, it has been exercised very unevenly, reflecting the political economy context. On the one hand, government vets are still not even allowed to enter commercial premises without the owner's permission, rendering the industrial sector essentially immune from scrutiny (Andri and Riana Reference Jatikusumah and Arief2011). Conversely, veterinary authority in managing outbreaks of disease in backyard poultry has been accepted by governments at all levels. Similarly, while mass culling was rejected in favour of poultry vaccination, vaccination was only made compulsory for backyard poultry (Wiku Reference Adisasmito2011). Clearly, the empowerment of veterinarians within the transformed governance structures has been deflected away from powerful interests towards relatively powerless villagers. As Agus Suwandono (Reference Agus2011), a prominent Indonesian scientist and former Komnas FBPI member, observes: ‘regulation is regulation, but money is money’.
This outcome reflects the broader direction taken in the management of this NTS threat. As mentioned above, the NSWP had focused on backyard poultry as the source of H5N1 in Indonesia, deflecting scrutiny from the commercial sector. While the Indonesian government was clearly concerned with shifting attention away from the commercial sector, and the big players in the industry also actively sought to reassure consumers by publicly claiming H5N1 affected mostly ‘native’ birds in villages (Forster and Charnoz Reference Forster and Charnoz2013: an), the focus on the ‘backyard’ sector also reflected the common wisdom among international experts at the time, as well as international donors’ usual preference for working with the rural and urban poor and reluctance to take on big business (Perry et al. Reference Perry, Isa and Tarazona2009: 26–7; Forster and Charnoz Reference Forster and Charnoz2013). Thus, ‘international organisations…initially exercised their influence where they could – which was not in the commercial sector, nor in the [live poultry] markets’ (Charnoz and Forster Reference Charnoz and Forster2011: 90). Indeed, as long as the PDSR remained focused on Sector Four, its implementation was very smooth. In fact, it was described as an ‘iconic success in HPAI detection’ (Perry et al. Reference Perry, Isa and Tarazona2009: 26).
However, when the PDSR began to be partially redirected toward the commercial sector, the results were modest at best, reflecting how scientific expertise was marginalised when it clashed with commercial interests. This reorientation began in late 2008, as evidence accumulated of H5N1 circulating in Sector Three farms. As CMU officials reported, research showed ‘most sources of infection are in small-scale Sector Three – they have less biosecurity and vaccination and when they get cases they don't want to lose money so they sell [dead chickens] to traders – that's our challenge’ (Azhar and Noeri Reference Muhammad and Widowati2011). Heru (Reference Setjanto2011) goes further to claim that H5N1 already circulates in the breeding farms, and can be found in DOCs sold by nucleus firms to Sector Three farms, though the industry's extreme secrecy makes it very difficult to verify this. Nonetheless, action to tackle infections in the commercial sector has certainly been very limited. The PDSR launched a Commercial Poultry Veterinary Program to develop cost-effective biosecurity measures and encourage farmers to allow veterinarians to visit during H5N1 outbreaks. However, this was a small pilot conducted in only six Sector Three layer farms, participation was entirely voluntary, and farmers were disinterested for the reasons outlined earlier. On the whole, lower-level officials remain fixated on the myth that the problem is Sector Four. For example, health officials in Banten Province, near to Jakarta and home to many poultry farms – insisted that ignorant backyard farmers are to blame: ‘They keep the poultry beside the house; they don't separate it. We have regulations for Sector Four – they have to make a cage’ (Wahyu and Ritanugraini Reference Santoso and Ritanugraini2011).
Importantly, it is not simply that local governments are powerless vis-à-vis private interests; rather, reflecting their tight interrelations, they have sometimes actively disrupted efforts to transform or regulate industry. Consider the attempts to alter poultry marketing in the Jakarta Metropolitan Region. Around eighty per cent of poultry in Jakarta is sold live and butchered in open markets. In 2007, with FAO assistance, the Jakarta Provincial Government issued Province Act 4/2007. This effectively banned Jakartans from raising chickens by insisting that poultry be kept at least twenty-five metres from human dwellings – impossible in the crowded capital – and that poultry owners must register biannually with the Dinas and allow inspections (Charnoz and Forster Reference Charnoz and Forster2011). The Act also sought to close the city's 2,000 informal slaughterhouses, replacing them with twenty-five shelters and five massive slaughterhouses – four owned by the Jakarta government – which adhere to the highest biosecurity standards (Dwazil Reference Hidja2011). The FAO helped fund the transition and the training of inspectors, while FAO consultants liaised between local government and industry stakeholders, and attempted to persuade Jakarta businesses that buying chickens from registered slaughterhouses would help their reputation and create ‘a “win–win” situation’ (McGrane Reference McGrane2011). Nevertheless, the Act's implementation was delayed in April 2010 and again in December 2010, and there is currently no clear indication when, if ever, it will be properly implemented. The main stumbling block is the same provincial government that passed the Act. FAO's James McGrane (Reference McGrane2011) elaborates: ‘the pushback occurred last year from the Assistant [sic – Deputy] Governor for Economic Affairs. [It] has meant that we weren't as successful as we might've been’. Currently, FAO provides only limited assistance with market hygiene and sanitation capacity-building with more meaningful plans for market reform scrapped. While the precise constellation of industry–government interests underlying the Deputy Governor's intervention is murky, it is nonetheless significant and telling that the official responsible for economic issues was able to override the Jakarta public health and livestock Dinas and completely halt the programme's implementation.
A different approach was taken by USAID's Strategies Against Flu Emergence (SAFE) project, a follow-up to CBAIC, which was uniquely focused on the commercial sector. Like many USAID-funded programmes, SAFE bypassed government altogether, attempting instead to persuade nucleus and Sector Three operators that better biosecurity was in their material interests. SAFE also sought to convince ‘nucleus’ corporations to include biosecurity-related standards and bonuses in their contracts with small farmers. However, as explained earlier, current practices provide nucleus firms with gargantuan profits with minimal economic risk from disease, while Sector Three farms cannot afford biosecurity measures. Consequently, SAFE's efforts were both naive and fruitless. As one poultry market expert argues, the private sector is solely concerned with profit: ‘decision-making is about economic imperatives, not public health – public health people can't get that’ (Anonymous 2011d).
Thus, reflecting the political economy context, despite the supposedly urgent securitisation of H5N1 in Indonesia, the industry's involvement has remained voluntary or, where regulation was announced, as in Jakarta, it has not been implemented. Industry players only engaged with the PDSR on their terms (Forster and Charnoz Reference Forster and Charnoz2013: ap). For example, in August 2011, the CMU helped negotiate the establishment of a national committee on poultry health. It has twenty-six representatives from industry, MoA and universities and it is meant as a forum for discussing problems in the sector and possible solutions. Industry representatives only agreed to participate on the condition that discussions remained confidential. The only part of the NSWP that potentially threatened industry interests, the proposals for vertical integration, was essentially ignored because the state–business pact that underpins the existing nucleus-plasma structure remains intact. As the director of the MoH's Zoonotic Diseases Division observes, ‘restructuring the poultry industry is the only part of the national avian influenza strategy not yet done’ (Misryiah Reference Misryiah2011).
The decentralisation and political economy context in Indonesia has thus profoundly shaped the governance of H5N1, producing a highly uneven and largely ineffective governance regime. PDSR, the biggest international H5N1 project, did considerably rescale the management of H5N1, but only among backyard poultry owned by poor, relatively powerless villagers. Conversely, few inroads were made in the commercial sector. Local government resistance to efforts to establish strong animal health systems and the central government's indifference to the disease's spread in the commercial sector meant that the new, multilevel governance systems affected only the weakest societal group. Even this attenuated regime now seems in decline as donor interest wanes. Although the CMU has expanded its focus to zoonoses more broadly, at the time of writing it appeared the unit would be disbanded. The situation is worse at the provincial and district levels, where local governments were supposed to take ownership of donor projects. But given local power relations, as FAO's Eric Brum (Reference Brum2011) observes, ‘there is no advocate [for these issues] at the local level’ (also Normile Reference Normile2007). Consequently, local governments show little willingness to adequately fund the agencies established by donors. Local health officials in Banten, for example, already complain that their Local Disease Control Centre is ineffective, because ‘there's no…personnel budget, no support from national government’ (Wahyu and Ritanugraini Reference Santoso and Ritanugraini2011). While poststructuralists often suggest that donors cultivate a ‘governmentality’ that outlasts their interventions, these findings show, as in the case of haze (chapter three), that governance arrangements tend to revert to local power relations when international pressure and resources are withdrawn.
Conclusion
Infectious disease is now frequently portrayed as a dangerous security threat on a global scale. Securitisation scholars have usefully shown that the public health issues that are securitised are almost invariably rapidly spreading infectious diseases that are seen to emerge in poorer countries and have the potential ability to proliferate around the world, threatening the populations of Northern states and the global economy. But, like other Copenhagen School adherents, these scholars have not examined the factors shaping how these health security issues are managed on the ground in the countries in which they are seen to originate, instead focusing on the ‘speech acts’ of international health diplomacy. Yet, as our case studies and others show, there is often a large gap between the rhetoric of securitisation and the governance response. Copenhagen scholars can only lament this gap, blaming it on the reluctance of Southeast Asian states to relinquish their sovereignty. This argument is clearly incorrect. In our cases, Thailand was the most resistant to international intervention, yet stringently implemented international biosecurity protocols; Indonesia accepted the most intervention of any country on Earth, yet the governance regime produced was weak and uneven. It is only when attempts to govern NTS issues are analysed, via the STA, as contestation over rescaling, situated within concrete state–society and political economy contexts, that real-world outcomes can be adequately understood.
In Thailand's case, an export-oriented, politically powerful poultry sector pushed for strong and immediate action on H5N1 when it lost its export markets overnight. The Thai government then simultaneously prevented direct international involvement in the management of the disease, while selectively rescaling H5N1 governance by applying international regulatory standards to legitimise policies that favoured the conglomerates but highly disadvantaged small producers. This spurred the further centralisation and consolidation of the poultry sector, but within highly mechanised and technologically sophisticated farms, which has apparently helped curb H5N1 infections among humans significantly. In Indonesia, decentralisation and a poultry sector with a very different political economy have generated a dissimilar and uneven pattern of rescaling. On the one hand, poor villagers were subjected to considerable international intervention and surveillance through the large-scale, multilevel programmes of PDSR and DSO. On the other, the powerful commercial sector, where the disease largely circulates, was left almost entirely exempt from regulation. The critical difference made by different local contexts of NTS governance is clearly illustrated by the practice of multinational poultry industry behemoth CP, which operates in both countries. In Thailand, it endorsed stringent international regulatory standards, since its profits depended on reassuring export markets; in Indonesia, it persisted with a nucleus–plasma arrangement that actively fosters avian influenza, because its profits are best safeguarded that way.