

Scientists around the world have been rushing to create a series of Covid-19 vaccines that can keep up with the many variants attested to date. Health authorities in several countries, including the USA, UK, China and Russia, have aggressively promoted their vaccine candidates. At the same time, vaccine-hesitant members of many communities and anti-vaccine activists continue to question the entire vaccine project, and some even argue that the whole virus is a scam and part of a plot to profit from developing and selling vaccines and other treatments for many years to come. In what follows, we adopt Reference Gust, Brown and SheedyGust et al.’s (2005) and Reference BrowneBrowne’s (2018) approach in considering vaccine hesitancy, vaccine scepticism and anti-vaccination as points along an attitudinal continuum rather than distinct attitudes that can be easily delineated. The spread of vaccine-hesitant and anti-vaccination narratives, moreover, must be understood against the backdrop of complex factors. One such factor is the growing mistrust of elites and experts, including official sources of medical knowledge and the institutions involved in producing and communicating this knowledge (Reference KennedyKennedy 2019). Doubts about the intentions of the World Health Organization (WHO) and the US Centers for Disease Control and Prevention, for instance, feature prominently in contemporary anti-vaccination narratives. Another factor is that concepts such as ‘evidence’ are increasingly questioned and redefined, even within parts of the medical establishment itself (Reference Greenhalgh, Howick and Maskrey NGreenhalgh et al. 2014), and their role in the construction and dissemination of knowledge is being reassessed. These and other factors combine to weave a multiplicity of intersecting and complex narratives that circulate widely in all societies and impact the acceptance of various types of pharmaceutical interventions in general and the uptake of Covid-19 vaccines in particular.
The discussion regarding potential pharmaceutical treatments became highly politicized early on in the pandemic, especially after former President Trump officially endorsed the malaria drug hydroxychloroquine in April 2020, against clear medical advice, arguing ‘I’m not a doctor. But I have common sense’ (Reference BrewsterBrewster 2020). At that point there was no prospect of any vaccines on the horizon, and with many deaths reported daily in the USA and elsewhere, even well-informed doctors began to justify Mr Trump’s hasty recommendation despite the absence of any scientific proof supporting the drug’s efficacy or safety. Dr Joshua Rosenberg, a critical care doctor at Brooklyn Hospital Center, cited ‘good reasons’ for explaining Mr Trump’s advocacy of the drug (The New York Times, reported by Reference CollinsCollins 2020 in Vox):
I certainly understand why the president is pushing it … He’s the president of the United States. He has to project hope. And when you are in a situation without hope, things go very badly. So I’m not faulting him for pushing it even if there isn’t a lot of science behind it, because it is, at this point, the best, most available option for use.
Other doctors argued that false hope can be damaging and criticized the former president and his supporters for cheerleading the drug in the absence of any proof of its efficacy (Reference CollinsCollins 2020).
The debate about vaccines and treatments thus does not only reflect tensions between science and politics and expert and non-expert discourses. It also highlights the fact that there are divergent views within the scientific community itself on when new evidence may be ready to be put into political action, and what considerations – other than the findings of randomized controlled trials – might be brought to bear on the decision. The haste with which a solution had to be found to arrest the spread of the disease, and the pressure on the medical community to produce a miracle cure, both resulted in widespread discussions about studies drawing conclusions that are premature or even fraudulent (Reference Kahn, Henry, Mastroianni, Chen and MacklinKahn et al. 2020; Reference JiangJiang 2020). This chapter explores the divergent arguments used in this debate and their various and complex value-laden underpinnings. It also engages with grassroots responses to the roll-out of Covid-19 vaccines as a case in point, drawing on historical parallels where relevant to explore some of the reasons (in Fisher’s sense of reasons and good reasons; see Chapter 3) that inform the decisions different members of the community make about the desirability or safety of vaccines.
5.1 Structural and Material (In)coherence: Science and Public Policy under Pressure
Much of the intense debate and political bickering over Covid-19 vaccines in the early months of 2021, which revolved around the use of the Oxford–AstraZeneca (Vaxzevria) vaccine, arguably undermined public trust in the safety of all vaccines that were being rolled out around the same time. A number of governments paused the roll-out of the AstraZeneca vaccine in March and April 2021 in response to a very small number of serious cases of blood clotting (thrombosis) in patients who had received the first dose.Footnote 1 Structural and material incoherence in the public health messages and recommendations that followed from the decision by some governments to halt the roll-out of AstraZeneca triggered public anxiety and confusion regarding this specific vaccine and the vaccine programme more generally.
Following the first instances of reported blood clots in Denmark and Norway, the European Medicine Agency (EMA) declared on 11 March that ‘there is currently no indication that vaccination has caused these conditions, which are not listed as side effects with this vaccine’.Footnote 2 A little less than a month later, the EMA’s safety committee (PRAC) concluded that ‘unusual blood clots with low blood platelets should be listed as very rare side effects of Vaxzevria (formerly COVID-19 Vaccine AstraZeneca)’.Footnote 3 In a statement intended for health professionals issued on the same date (7 April 2021), the EMA explicitly stated that ‘a causal relationship between the vaccination with Vaxzevria and the occurrence of thrombosis in combination with thrombocytopenia is considered plausible’ (emphasis added).Footnote 4 An updated statement on 20 May makes no mention of the ‘causal relationship’ and instead presents the connection between the two as a mere observation: ‘A combination of thrombosis and thrombocytopenia, in some cases accompanied by bleeding, has been observed very rarely following vaccination with Vaxzevria’ (emphasis added).Footnote 5
Another statement for health professionals about the safety and effectiveness of Covid-19 vaccines, this time issued by the WHO on 11 June 2021, similarly acknowledged that ‘the AstraZeneca and Janssen COVID-19 vaccines have been associated with a very rare and unusual clotting syndrome involving thromboembolic events (blood clots) with thrombocytopenia (low blood platelet count)’.Footnote 6 However, the same document implicitly raised doubt about this conclusion: ‘The overall number of reports received of blood clots in the veins or arteries (including venous thrombosis or venous thromboembolism) occurring without thrombocytopenia is no higher than the expected background population rate for the more common type of blood clots in most countries’.
Differences in conclusions, emphases and lack of transparency about the arguments informing the debate led by international and pan-national health authorities fuelled mistrust in both scientific and political institutions, and hence exacerbated vaccine hesitancy globally. A similar pattern of conflicting statements being released at different times pervaded vaccine recommendations at the national level. In Canada, the National Advisory Committee on Immunization (NACI) was accused of creating confusion with its updated Covid-19 statement on 3 May, recommending that Canadians less likely to contract Covid-19 should consider waiting for a Pfizer or Moderna vaccine instead of opting for what was then on offer, that being AstraZeneca.Footnote 7 This contradicted previous recommendations that encouraged Canadians to take whatever vaccine is available. In its new statement, NACI maintained that it would ‘preferentially recommend authorized messenger RNA (mRNA) COVID-19 vaccines due to the excellent protection they provide and the absence of any safety signals of concern’,Footnote 8 thereby indirectly creating the impression that AstraZeneca is a second-rate and potentially dangerous vaccine. A few days later, the Ontario government announced that it will no longer offer the Oxford–AstraZeneca Covid-19 vaccine as a first dose due to the risk of rare blood clots. Prime Minister Justin Trudeau later sought to reassure Canadians that all vaccines approved for use in Canada are safe and effective by confirming the original recommendation of taking the first vaccine offered: ‘Make sure you get your shot when it’s your turn. We are continuing to recommend to everyone to get vaccinated as quickly as possible so we can get through this’.Footnote 9
Similarly, the Australian Technical Advisory Group on Immunisation (ATAGI) advised that people between the ages of 16 and 59 should preferably receive Pfizer shots, while the government maintained that the same group of people can opt for AstraZeneca after consulting their doctors. On 28 June 2021, the prime minister Scott-Morrison declared in a press conference: ‘the ATAGI advice talks about a preference for AstraZeneca to be available and made available to … those over 60. But the advice does not preclude persons under 60 from getting the AstraZeneca vaccine … So if you wish to get the AstraZeneca vaccine, then we would encourage you to … go and have that discussion with your GP [general practitioner]’.Footnote 10 These and similar declarations led both journalists and medical experts to conclude that ‘mixed messaging from the Australian government and ATAGI has created confusion – and hesitancy – about the available vaccines and their safety’ (Reference ShieldsShields 2021).
The confusion and controversies surrounding the Oxford–AstraZeneca vaccine and the importance accorded to the very rare reported cases of blood clotting also demonstrate the fundamentally anecdotal or narrative nature of medical evidence. As Reference RoneRone (2021) points out in connection with the debate about AstraZeneca,
Ultimately, science is based on empirical data and when there is not enough data, science cannot say things with certainty. When new data is available, scientists are ready to correct previous errors thus incrementing knowledge. Science has never been about absolute certainty. Nor has it pretended to be. That is its strength. But this does not sound very reassuring when one needs to take a personal decision affecting one’s own health.
The inherent uncertainty of science means that the positions taken by various national and local governments can and often do rely more on narrative proximity and identification with the individual characters than on risk calculation based on numbers. The case of the Oxford–AstraZeneca vaccine thus confirms Fisher’s claim that ‘the operative principle of narrative rationality is identification rather than deliberation’ (Fisher 1989:66). In Norway, a country with a small population and high life expectancy, the AstraZeneca vaccine was permanently suspended when five people were hospitalized for a combination of blood clots, bleeding and a low count of platelets after receiving the first dose. Three of them later died. On 15 April 2021, the Norwegian Medical Agency delivered a report to the Norwegian government that concluded the following: ‘Since there are few who die from Covid-19 in Norway, the risk of dying from taking the AstraZeneca vaccine will be greater than the risk of dying from the disease, especially for younger people’.Footnote 11 The Norwegian Medical Agency also acknowledged that there are several uncertainties with this analysis: first, that the current spread of infection informing this conclusion could change; and second, that the relative death rates are difficult to determine, given that the estimation is based on numbers from Norway and Denmark only.Footnote 12 Their conclusion was therefore not based on firm evidence alone but on ‘good reasons’, with several ‘non-scientific’ considerations taken into account. In particular, the agency’s assessment ultimately focused on what is likely to ‘ring true’ to members of the public, as evident in its final justification for suspending the AstraZeneca vaccine: ‘There is reason to believe that there is a high degree of skepticism about using the AstraZeneca vaccine in Norway and it is uncertain how many people would have accepted an offer of this vaccine now’.
It is worth noting at this point that governments and medical institutions are not the only narrators whose discourses influence public trust in specific vaccines or in vaccination in general. The high degree of scepticism acknowledged by the Norwegian Medical Agency is not triggered by the reported findings of specific trials alone but also by the impression of relative danger or safety created by a range of narratives circulating in public space, including narratives framed and reinforced by the media in different countries. Reference RoneRone (2021), for instance, explains – based on her experience of being encouraged to take the vaccine on offer by German and Czech friends but actively discouraged from doing so by friends and family in Bulgaria – that Bulgarian media’s emphasis on uncertainties surrounding vaccination and the fact that they provide space for narratives that undermine trust in vaccines, including anecdotal stories ‘insisting a person gets much better immunity if they actually get sick’, have led to a high level of scepticism in the country. For a long period at the start of the pandemic, Rone tells us, ‘all Bulgarian mainstream media invited doctors who insisted that the virus is a simple flu, masks don’t help, we need to reach herd immunity’, whereas in countries such as the UK the media tend not to emphasize uncertainties, but rather ‘the benefits of vaccinating as many people as possible, starting from the most vulnerable groups’ (Reference RoneRone 2021).
Speaking on the CTV Television Network in Canada. on 4 May 2021, the Chair of the National Advisory Committee on Immunization (NACI) in Canada, Dr Caroline Quach-Thanh, controversially admitted that risk cannot necessarily be calculated rationally: ‘If, for instance, my sister was to get the AstraZeneca vaccine and die of a thrombosis when I know that it could have been prevented and that she’s not in a high-risk area, I’m not sure I could live with it’.Footnote 13 She was later criticized for fuelling fear and hesitancy through her statement. On an epistemological level, however, her unguarded response reveals the extent to which medical discourses depend on narrative rationality but at the same time struggle to make sense of it. While trying to defend, from the point of view of scientific rationality, the NACI’s decision to advise young people to wait for the preferred vaccine, she admitted – almost by a slip of the tongue – that what ultimately matters in practice is whether the decision to take or not take a specific vaccine is consistent with – speaks to – people’s lived experience and its potential risk to loved ones, rather than its overall risk assessment. This is about whether a person embedded in space and time and emotionally connected to others can ‘live with’ a particular decision they have to make, not about assessments of risk in the disconnected and sanitized environment of the laboratory.
That all vaccines – indeed, all forms of pharmaceutical and medical interventions in general – carry a certain level of risk is not disputed by the scientific community nor by policy makers. But scientific rationality tends to weigh the benefits and dangers of this risk in the abstract, whereas narrative rationality works by weighing it in the context of a life lived with others. This explains why parents may be particularly wary of vaccination in general. As Reference LarsonLarson (2020:5) explains, ‘the timing of childhood vaccines coincides with a number of childhood infections and at a time when parents are particularly focused on the evolving development of their child, thus making associations with vaccines more believable and helping to fuel the contagion of rumors’. Similarly, early signs of autism coincidentally tend to become noticeable around the same time as the measles, mumps, and rubella (MMR) vaccine is given to children, ‘when all parents are focused on first words, first steps’ (Reference LarsonLarson 2020:11). The risks that parents and other members of society associate with vaccines may thus not even be the actual risks science establishes and acknowledges, making the task of debunking them more difficult and complicated (Reference LarsonLarson 2020:37). In what follows we will further unpack some of these complexities and explore ways in which understanding how narrative rationality works may give us better insight into how to address anxieties surrounding vaccination more effectively. But first a brief word about the role of characterological coherence in influencing public confidence in vaccines.
5.2 Characterological Coherence and Public Confidence in Vaccines
We saw in Chapter 2 that characterological coherence is assessed on the basis of the perceived reliability (or otherwise) of specific characters associated with a given story. For many, therefore, the fact that Neil Ferguson – the British public figurehead for the argument supporting a strict lockdown to arrest the spread of Covid-19 – was found to have flouted the rules of lockdown to meet his lover meant that his advice on the necessity of lockdowns could no longer be trusted. In the case of vaccines and other pharmaceutical interventions, characterological coherence seems to work in more contradictory ways that are influenced by centuries of public opposition to vaccination, and by repeated attempts on the part of governments to suppress this opposition by passing laws that make certain types of vaccines mandatory. Examples include the Vaccination Acts of 1853 and 1867 in England, which made vaccination against smallpox mandatory for infants up to 3 months old and then up to 14 years old, respectively. Alongside these legal measures, institutions representing medical practitioners also have a history of censuring doctors who act in ways that undermine specific vaccination campaigns. The most recent example at the time of writing is Dr Gerard Waters, who was suspended from the medical register by the High Court of Ireland in April 2021 for refusing to vaccinate his patients against Covid-19.Footnote 14 Dr Waters, who believed the vaccine to be ‘untrustworthy and unnecessary’ (Reference CullenCullen 2021) and ‘disagreed with how quickly the vaccines had been developed’ (Reference O’ConnorO’Connor 2021), described himself as a ‘conscientious objector’, thus invoking associations with pacifism and the Christian principle ‘thou shalt not kill’, used by the Quakers in particular to justify refusal of armed service in both world wars. The framing of a narrative such as Dr Waters’s is important in influencing assessments of characterological coherence. In this case, powerful institutions are narrated as exercising their superior power against a principled individual who holds fast to his beliefs despite the adverse consequences to his career. This type of storyline appeals to particular values that many people hold dear, such as courage and integrity, which can provide ‘good reasons’ for believing dissenting rather than official, mainstream characters. The importance of such values in assessing characterological coherence is most evident in a much more high-profile case associated with anti-vaccination movements: that of Andrew Wakefield.
Andrew Wakefield is a former physician who was struck off the medical register by the UK’s General Medical Council following the publication of a 1998 co-authored article in The Lancet,Footnote 15 which posited a link between the MMR vaccine and autism. He continues to campaign against vaccination in general and has become a cause célèbre for the anti-vaccination movement, ‘a headliner for the vaccine-sceptic circuit’ as Reference OmerOmer (2020) calls him in a review of The Doctor Who Fooled the World – an unauthorized biography of Wakefield written by Brian Deer (Reference DeerDeer 2020), the investigative reporter who first broke the story about the 1998 Lancet article. For many people, Wakefield’s open censure by the medical community meant that he was no longer credible, and hence his arguments against vaccination could not be trusted. For others, as Reference LarsonLarson (2020) points out, he became a symbol of integrity, of courage in the face of persecution, lending his claims believable whatever ‘facts’ are presented against them by the scientific community. For anti-vaccine advocacy groups such as Generation Rescue who saw Wakefield in this light, he was ‘Nelson Mandela and Jesus Christ rolled up into one’ (cited in Reference LarsonLarson 2020:11). The Vaccine Resistance Movement (VRM) reinforces the impression of a Jesus Christ fighting persecution by raising donations ‘to finance his many court cases’ (Reference LarsonLarson 2020:12). This example suggests that assessments of characterological coherence are entangled, at least in some cases, with the exercise of institutional power and our tendency to admire and respect those who stand up to it. It is no coincidence, therefore, that anti-vaccination websites such as Children’s Health Defense, run by Robert F. Kennedy, Jr., feature extensive quotes from Mahatma Gandhi’s prolific writings against vaccination.Footnote 16
In the debate about Covid-19 vaccines and vaccination more generally, assessment of characterological coherence does not only apply to individuals but also to nations and institutions. Just as Reference BakanBakan (2003) asked in his famous book The Corporation, what the personality of the corporation would be if it were a person, we all have a tendency to associate various types of institutions and governments with certain qualities, on the basis of which we become more or less trusting of their discourses. In our current context, this is particularly evident in the case of countries and institutions involved in the debate on global vaccine distribution, and more specifically, the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) and its consequences for the Covid-19 response. In October 2020, India and South Africa proposed a waiver to the intellectual property (IP) regulations defined through this agreement in order to give poorer countries access to the vaccine recipes and hence facilitate local vaccine production. The waiver was supported by 62 member states of the World Trade Organization (WTO), but several wealthy countries and pan-national institutions, including the USA, the UK and the European Union, initially opposed it. While insisting that they are all committed to work with low and middle income countries to achieve ‘equitable access to vaccines across the globe’,Footnote 17 these key participants in the debate maintained that changing the IP rules would be unproductive, and as formulated in a statement by the UK government addressed to the TRIPS Council, would constitute an ‘extreme measure to address an unproven problem’.Footnote 18 Reference Dangor and SuckerDangor and Sucker (2021), members of a group of academic lawyers which included an advisor to the South African government on international relations, saw the response to the waiver as part of a more pervasive pattern of characterological incoherence that many have come to associate with wealthy countries; these tend to advocate global governance along paradoxical lines that are ultimately intended to ensure their own national interests:
… while committing to work with UN-led initiatives such as the Covid-19 Vaccine Global Access Facility (Covax), ostensibly aimed at equitable and science-led global vaccine distribution, the richer countries undermined such collective processes by practising vaccine nationalism – signing agreements with pharmaceutical companies to supply their own populations in a manner that reduces equitable access for others, often leading to forms of vaccine apartheid between countries … That the rich countries, which purport to champion global governance, acted contrary to and in a manner that undermined UN-led initiatives to create global governance bodies to allocate and distribute the vaccines based on science and ethics, underscores the sentiment in much of the global south that rich countries of the north instrumentalise the institutions of global governance in ways that are only beneficial to them.
Reference HomerHomer (2021) offers a detailed example of the type of behaviour that underpins perceptions of characterological incoherence in relation to specific rich countries in this context:
In June, the G7 countries pledged to donate 1 billion doses to ‘poor countries’, with the UK pledging 100 million of them. Yet so far, the UK has delivered only 5.1 million doses to Covax and sent just 10.3 million abroad in total. At the same time, the UK has actually taken doses from Covax that it has a right to (many other wealthy countries have waived their right to their share). In June, the same month it made its 100-million-dose pledge, the UK received 539,000 doses from Covax, more than double the doses Covax sent to Africa in the same month.
Similarly, in an analysis of the EU’s response to the waiver, Reference Engebretsen and OttersenEngebretsen and Ottersen (2021) explain how the EU paradoxically uses ‘global collaboration’ as an argument against the global right to vaccine production. In claiming that ‘in a global pandemic only broad and equitable access to vaccines across the globe will ensure that the public health crisis can be tackled effectively, including in developing countries that have no production capacities’ (emphasis added),Footnote 19 the lack of production capacities in poor countries is presented as an indisputable fact. Global collaboration accordingly is assumed to consist of compensating for this lack by increasing vaccine access through means other than sharing the recipe with all nations. There is no room here for considering the possibility of mitigating the presumed lack by supporting the development of production capacities in poor countries. This logic ‘leads to a paradox’ some have come to associate with the character of wealthy nations: in this particular context, ‘[l]ack of efficiency and capacity in the health service in poor countries is used as an argument for globally defined measures, and against contributing to the development of capacity and improving efficiency by allowing these countries to develop vaccines and treatment programs themselves’ (Reference Engebretsen and OttersenEngebretsen and Ottersen 2021).
For some, then, arguments against sharing vaccine recipes – such as ‘IP protections provide incentives to companies to create new and groundbreaking technologies’ (Reference Lee and HoltLee and Holt 2021) – are bogus and consistent with the exploitative and dishonest character of rich countries and corporations intent on blocking the development of vaccine production capacity in poor countries. For others, it must be acknowledged, such arguments will continue to be perceived as not only rational and realistic but also as indicative of the responsible character of the governments that promote them and their laudable loyalty, above all, to their own populations. What has been negatively referred to in much of the literature and the media as ‘vaccine nationalism’ (Reference Weintraub, Bitton and RosenbergWeintraub et al. 2020; Reference EatonEaton 2021; Reference KhanKhan 2021; Reference LagmanLagman 2021; Reference Mayta, Shailaja and Nyong’oMayta et al. 2021) has thus been explained by others in pragmatic terms as a case of governments like the UK’s sensibly ‘striking deals early because, without the upfront investment from rich countries, … vaccine manufacturers would not be making any vaccine at risk’ (Reference TorjesenTorjesen 2020). The term ‘vaccine nationalism’ appeared in the late spring of 2020 and ‘is linked to agreements that reserve the bulk of emerging vaccines for a limited number of countries, traditionally in the developed world’ (Reference RutschmanRutschman 2020). The strategy adopted is not new – a similar pattern of rich countries hoarding vaccine production for their own populations was also evident in the case of the H1N1 flu in 2009 (popularly known as swine flu). But the strategy and the narratives that underpin and justify it are now a ‘hallmark of negotiations during large-scale outbreaks of vaccine-preventable diseases’ (Reference RutschmanRutschman 2020). The feminist writer Rosebell Kagumire adopts the term ‘vaccine apartheid’ (rather than ‘vaccine nationalism’): this has gained some currency and is used, along with hashtags such as #EndVaccineApartheid and #EndVaccineInjusticeInAfrica, to demand that immediate action be taken to alleviate acute Covid-19 vaccine shortages (Reference KagumireKagumire 2021). Kagumire argues that the emergence of the Omicron variant in November 2021, which was initially assumed to have originated in South Africa (see Chapter 1), revealed the colonial undertones of the policies adopted by wealthier countries. Rather than praising the South African government for its transparency and working with it to address this new source of threat, the European Union, the USA and the UK decided to impose a banket travel ban on Southern Africa and neighbouring countries. ‘At the same time’, Kagumire points out,
the emergence of ‘variants of concern’ across the world (including Europe) and growing COVID-19 death toll among unvaccinated populations have not dissuaded the West from pursuing vaccine hoarding and vaccine nationalism policies.
By privileging some human lives over others, Western countries thus arguably prolong the pandemic and impact not just the lives and livelihoods of marginalized populations, but also of those they set out to protect.
5.3 Transcendental Values and Conceptions of Freedom
Policies adopted by governments and other institutional bodies in relation to pharmaceutical interventions such as vaccination may be seen as rational, fair and reassuring by some members of the public and as intrusive, discriminatory and oppressive by others. The issue here is not simply one of assessing the structural, material and characterological coherence of a given argument and those who advocate it, though such assessment does play a role in this as in all other contexts. How individuals respond to institutional measures such as those mandating vaccination is ultimately also informed by the transcendental values to which they subscribe and that constitute the core of narrative rationality. As Reference Kaebnick and GusmanoKaebnick and Gusmano (2019) put it, ‘Before we can make a meaningful dent in the number of people who refuse to vaccinate their children, we have to accept that “because science” won’t convince anyone. At the end of the day, it’s values – beliefs about what matters, what’s important, what should guide our lives and societies – that are most important’.
One such value determines our approach to the balance between personal freedom and social responsibility that we already saw play a major role in shaping responses to restrictive measures such as lockdowns and quarantines (Chapter 4). People are generally aware of the importance of balancing personal needs and convictions with those of society at large, and can steer a course that avoids direct conflict between the two under most circumstances. The more intrusive and severe the measures adopted to control individual behaviour, however, the more likely it is for increasing numbers of people to react negatively to the intrusion into their personal lives, and – importantly – into those of others, irrespective of their own position on the subject of intrusion. Hence, for instance, a January 2021 survey of potential acceptance of a Covid-19 vaccine that involved 13,426 people in 19 countries found ‘a discrepancy between reported acceptance of a COVID-19 vaccine and acceptance if vaccination was mandated by one’s employer’. All respondents to the survey, ‘regardless of nationality’ and despite marked differences in the level of vaccine acceptance across countries, ‘reported that they would be less likely to accept a COVID-19 vaccine if it were mandated by employers’ (Reference Lazarus, Ratzan and PalayewLazarus et al. 2021:226). Similarly, Reuters reported in November 2021 that almost 50% of employees at aircraft companies based in Kansas were defying the federal mandate to be vaccinated, at the risk of losing their jobs. Importantly, the head of the Machinists union district is quoted as asserting that many employees ‘did not object to the vaccines as such … but were staunchly opposed to what they see as government meddling in personal health decisions’ (Reference Bellon and JohnsonBellon and Johnson 2021). Lazarus et al. thus conclude that their finding regarding widespread rejection of mandated vaccination ‘across all countries with both high and low reported vaccine acceptance proportions suggests that promoting voluntary acceptance is a better option for employers’ (Reference Lazarus, Ratzan and PalayewLazarus et al. 2021:226).
At the same time, the more serious a threat to the smooth running of everyday life and the survival of a community, the more likely that those in charge – including governments and employers – will intervene to control individual behaviour. Nowhere is the tension between individual freedom and overall public interest more pronounced than in the fraught history of vaccination, precisely because while ‘[s]tanding up for rights to freedom of expression, choice, and individual dignity are all healthy characteristics of democratic societies’, as Larson explains, ‘contrarian views are problematic for a technology like vaccines whose success – at least for many vaccines – depends on “herd” or population cooperation to reach herd immunity’ (Reference LarsonLarson 2020:54). Whatever the justification, historical instances of mandating vaccination invariably resulted in mass protests and anger. The latest attempts to impose vaccine passports during the Covid-19 crisis is no exception (Figure 5.1).

Figure 5.1 Worldwide Rally for Freedom, London, 21 November 2021.
Mandatory vaccination is a highly controversial topic whose history goes back to the middle of the nineteenth century and various national responses to the spread of smallpox at the time. As mentioned earlier, for example, vaccination against smallpox became compulsory in England in 1853 for all infants in their first three months of life, with the 1867 Act extending this requirement to age 14 and imposing severe penalties on parents who failed to vaccinate their children. Seen as a serious encroachment on civil liberties, resistance to these acts grew stronger over the years and eventually led to the passing of the 1898 Vaccination Act, which introduced a ‘conscience clause’ allowing parents who had serious concerns about vaccination to obtain a certificate of exemption (Reference Wolfe and SharpWolfe and Sharpe 2002). Interestingly, it was this Vaccination Act that introduced into English law the now widely used term ‘conscientious objector’, which we tend to associate with the right to refuse military conscription on grounds of freedom of conscience, thought or religious belief. It is this history, and the association of the anti-vaccination stance with the idea of challenging powerful institutions, that might explain assertions such as ‘anti-vaccination is not only a belief but a cause’ (Reference BrutonBruton 2020:63; emphasis in original).
Arguments against vaccination based on individual freedom can thus attract followers who are happy to be vaccinated themselves but because they ‘believe in the more fundamental democratic right to choose’, they see the issue from the perspective of others’ right to ‘dignity and respect’ (Reference LarsonLarson 2020:30). This is a case of ‘I disapprove of what you say, but I will defend to the death your right to say it’ – a quote often wrongly attributed to Voltaire. Even those who would not necessarily go as far as condemning mandatory vaccination or protesting against it, given the implications of vaccine hesitancy for society at large, may nevertheless feel uncomfortable with it because it encroaches on other people’s autonomy. A respiratory doctor writing as ‘Anonymous’ in The Guardian in November 2021 expresses anger at those still refusing to take the vaccine, who end up on ventilators in packed intensive care units where he or she has to fight to keep them alive. Anonymous’s patience, we are told, is ‘wearing thin’ despite accepting that a cornerstone of the way doctors protect patients’ autonomy ‘is the recognition that others may reasonably make decisions we may see as irrational or wrong’. And yet, the author continues, ‘I find the idea of NHS [UK National Health Service] and care staff being forced to be vaccinated very difficult. I know that it is the right outcome, but I dislike the means of bringing it about’ (Anonymous 2021).
Today, governments hesitate on the whole to mandate vaccination legally in the same intrusive manner, perhaps to avoid some of the more extreme responses that strategy has historically elicited. Instead, they adopt strategies that mostly do not involve passing laws as such but nevertheless restrict the freedom of the non-vaccinated in various ways while protecting the welfare of the population at large as they see it. As of July 2021, for instance, many countries in Europe – from Greece and Cyprus to Germany and Luxembourg – have been ‘obliging their residents, as well as travellers, to carry their COVID-19 passport’ to be allowed entry into any indoor public spaces such as hotels, pubs and restaurants.Footnote 20 As the number of Covid-19 cases spiked and the percentage of those vaccinated remained ‘shamefully low’ by comparison to other European countries, Austria went further by imposing a nationwide lockdown on 15 November 2021 on anyone over the age of 12 who had not received two doses of the vaccine and those who had not recently recovered from the virus. Those who fell into one of these two categories – ‘roughly 2 million people out of a population of 8.9 million’, according to the Austrian Press Agency (Reference LinnaneLinnane 2021) – could only leave their homes to fulfil a small number of essential needs (Euronews 2021). Offenders, as in the case of the smallpox mandates in the mid 1800s, were to be heavily fined. A week later, Austria decided that selective lockdowns were not working, placed the whole country under stay-at-home orders, and announced that Covid-19 vaccination would become compulsory from February 2022, ‘with large fines for those who refuse to be jabbed’ (Reference ClarkClark 2021). Other countries, like the UK, opted to allow businesses and other institutions to enact their own rules. These in turn are inclined to protect their interests by enforcing various types of restrictive measures such as those Reference Beioley, Parker, Strauss, Hancock and VenkataramakrishnanBeioley et al. (2021) label ‘no jab, no job’ contracts when reporting that ‘some companies, ranging from UK care-home operators to large multinational groups, were considering employment contracts requiring new and existing staff to have vaccinations once Britain’s adult population has been offered jabs’.
This relatively less restrictive strategy can still be rejected by many on the basis of values other than that of personal freedom, including respect for personal privacy and a commitment to non-discrimination. Thus Reference Beioley, Parker, Strauss, Hancock and VenkataramakrishnanBeioley et al. (2021) go on to report that
[m]ost employers [in the UK] are wary of any mandatory requirement for staff to be vaccinated, which would mean handling sensitive medical data, and could leave them open to legal challenges on discrimination grounds if workers refused jabs because of a religious belief, pregnancy, or a health condition that could constitute a disability.
And yet, as one NHS doctor points out, mandatory vaccination has long been widely accepted in some sectors, including medicine: ‘I cannot practice medicine in this country without having mandatory vaccinations including Hepatitis B and the MMR vaccine. So why should Covid-19 be any different?’ (Reference Batt-RawdenBatt-Rawden 2021). For many, moreover, the right of individuals to decide what they do with their bodies has to be weighed against others’ right to life, and for them the value of life ultimately trumps all others. If what an individual decides to do with their bodies endangers others’ lives then they must live with the restrictions society has to impose on them. Especially with the spread of what was then termed the Indian variant of Covid-19 in the spring of 2021, some have therefore argued for very extensive measures to be adopted (Reference O’GradyO’Grady 2021):
5.4 Pure Bodies, Microchips and Genetically Modified Organisms
One of the recurring objections to vaccines in general, including Covid-19 vaccines, is that they are not ‘natural’ and as such compromise the purity of the body, a view often traced back to Gandhi’s famous writings on the subject. A hero to many, Gandhi’s Guide to Health asserts that ‘vaccination is a very dirty process’ (Reference GandhiGandhi 2016:105). Reference LarsonLarson (2020:12) suggests that Andrew Wakefield’s anti-vaccination message resonates beyond his insistence on a link between the MMR vaccine and autism. It also ‘appeals to a growing constituency of naturopathic, anti-chemical, pro-nature, alternative health audiences’ (Figure 5.2). A study conducted by epidemiologists and psychologists and reported in The New York Times in 2021 found that people who object to vaccines are ‘twice as likely to care a lot about the “purity” of their bodies and their minds’ (Reference TaverniseTavernise 2021). ‘My body is a temple’ is thus a common refrain for many who seek exemption from vaccination on religious grounds (Reference StevensonStevenson 2021). The emphasis on purity is not restricted to religious groups, however. It may have its roots in religious beliefs in some cases but in others it is ‘entirely secular’, as in the case of ‘people who care deeply about toxins in foods or in the environment’ (Reference TaverniseTavernise 2021).
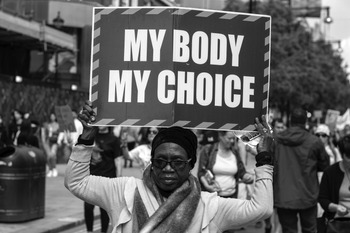
Figure 5.2 A protester in London asserts her right to making decisions concerning her body, May 2021.
A related topic concerns the use of human cells taken from aborted fetuses to test vaccines, and in some cases in their actual production. Here, it is again the question of the purity and sanctity of the human body, however underdeveloped, that informs the decision of some groups to reject specific vaccines. Thus, some US Catholic bishops described the Johnson & Johnson Covid-19 vaccine specifically as ‘morally compromised’ because what they called ‘abortion-derived cell lines’ (taken from the tissue of aborted fetuses) were used not only to test but also to develop and produce it, while others insisted that all three vaccines available in the USA (Pfizer, Moderna and Johnson & Johnson) are equally compromised for having used cell lines in the testing phase (Reference OlmsteadOlmstead 2021). For other religious groups, it is not the use of fetuses but the idea that their bodies may potentially be contaminated by certain ingredients such as pork-derived gelatin – used to stabilize vaccines – that poses a problem (Reference MilkoMilko 2020). The British Islamic Medical Association’s ‘Position Statement on the Moderna Covid-19 Vaccine’, for example, assures its audience that ‘[t]he Moderna vaccination has no components of human or animal origin. The lipid nanoparticle contains cholestorol from a plant source. There is no ethanol (alcohol) in the Moderna vaccine’.Footnote 21
A recurrent theme among some constituencies, especially on social media, is that Covid-19 vaccines contain a microchip that governments or global elites like Bill Gates intend to use for surveillance purposes (Figure 5.3), and that these intrusive measures constitute an assault not only on privacy but also on our personal health and well-being. Such beliefs are widely associated with conspiracy theories and hence dismissed outright, as an example of irrational thinking. But for many they resonate with and are as rational as arguments that are generally taken seriously by mainstream institutions, including the European Union. For instance, the concerns of activists who object to the use of genetic modification in the food and agricultural industries are generally taken seriously, despite obvious commonalities between them and those relating to genetic modification in the context of Covid-19 vaccines. Whilst mRNA vaccines can be considered a type of genetic-based therapy since they use a genetic code from Covid-19, science tells us that they do not alter our genes. But this may not sound very convincing to those who already lack trust in science, and often specifically in medical institutions because of their well-documented entanglement with politics and the neoliberal economy. Two relatively recent examples will suffice to clarify this particular source of anxiety for many people. The first is accounts of Goldman Sachs analysts weighing the economic benefits of recurring treatments vs one-shot cures and posing the question to their clients – in a report entitled ‘The Genome Revolution’ – ‘Is curing patients a sustainable business model?’ (Reference KimKim 2018). The second is ongoing concerns about the growing influence of Bill Gates’s funded Institute for Health Metrics and Evaluation (IHME), based at the University of Washington. Among other sources expressing such concerns, The Nation published a long article in December 2020 entitled ‘Are Bill Gates’s billions distorting public health data’ (Reference SchwabSchwab 2020) in which several examples are given of what the author describes as the IHME’s expanding and unquestioned dominion in the health sector. Reports of Bill Gates warning governments in November 2021 of smallpox terror attacks and calling for ‘the formation of a new billion-dollar World Health Organisation (WHO) Pandemic Task Force’ (Sky News 2021) served to further entrench the idea that global elites in general and Bill Gates in particular exercise unwarranted control over health policy.

Figure 5.3 New Zealand Public Party leader Billy Te Kahika Jr speaks at a Human Rights Violations protest at Parliament on 6 August 2020.
At any rate, to go back to the issue of genetic modification and vaccine hesitancy, the similarity to gene therapy, which does involve modifying a patient’s genes to cure specific diseases, and resonance with the debate about the purity of the human body that this topic evokes, both provide ample reason for many to question the wisdom of vaccination. Social media platforms abound with posts such as that shown in Figure 5.4,Footnote 22 from the Twitter feed of ‘joey_di_marco’, whose profile reads:
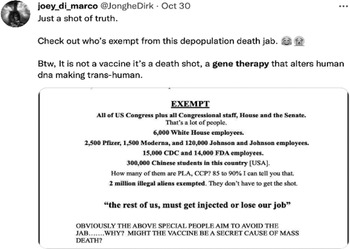
Figure 5.4 Post from the Twitter Feed of Joey di Marco, 30 October 2021
#freedomfighter #antiglobalist#truthseeker#alliantie#nature#animals#thepowerofwater#ewaranon#nietsiswathetlijkt
The idea that gene therapy is unnatural and ‘anti-human’, moreover, is far from new. Anti-GMO activists have drawn since the late 1980s on narratives that link GMOs (genetically modified organisms) with pollution, contamination or monstrousness (Reference Schurman and MunroSchurman and Munro 2009). Similar narratives have also been used by politicians, especially in Europe, where the legislation on GMOs is particularly restrictive. As Reference Christiansen, Andersen and KappelChristiansen et al. (2019) have pointed out, the restrictive rules imposed on GMOs are fundamentally based on the value of naturalness, since the organisms covered by the legislation are those ‘in which the genetic material has been altered in a way that does not occur naturally by mating and/or natural recombination’, according to the European Commission’s archived page on biotechnology.Footnote 23 In a blog post on The Daily Beast that questions this rationality and the values that underpin it, Reference AnslowAnslow (2021) thus concludes that ‘[i]n this pandemic anti-vaxxers didn’t need to discredit 200 years of vaccine efficacy, or explain away scientific consensus. They just needed to sow doubt about emerging biotechnologies, a job that had already been largely done for them by the press and politicians. Biotechnophobia was already endemic’.
Anslow’s critique of what he sees as the structurally incoherent attitudes of European politicians with regard to gene engineering is echoed by Brooks (Reference Anslow2021), an agricultural economist, who argues in a blog post on Open Access Government that European politicians show inconsistency when they queue up to praise the breakthroughs of the new vaccines:
These vaccines use the very same techniques of genetic modification (GM) or gene editing (GE) that most European politicians have spent the last 25 years preventing their citizens and farmers from having access to for the production and consumption of food, feed and fibre crops and which so-called environmental advocacy groups have opposed unequivocally.
If these politicians and advocacy groups were being consistent with their past behaviour, they would be vigorously campaigning against these vaccines’ approval and publicly stating that they personally will not be using them.
5.5 Resonance, Lived Experience and Trust
As mentioned earlier in this chapter and Chapter 3, and discussed in detail in Chapter 2, Fisher considers identification as the operative principle of the narrative paradigm (Reference FisherFisher 1987:66). A story, according to him, ‘not only says something about the world, it also implies an audience, persons who conceive of themselves in very specific ways’ (Reference FisherFisher 1987:75), and it is only when the story resonates with the ‘self-conception’ of this audience that they can and will accept it as true. Conversely, ‘if a story denies a person’s self-conception, it does not matter what it says about the world’ (Reference FisherFisher 1987:75) – it will not resonate. In order to appeal to ‘good reasons’ and ‘ring true’ for their audience, stories must thus create resonance.
What constitutes truth is ultimately a matter of trust, and that can override even direct personal experience, in this case of the symptoms of disease. For some, like Dr Samantha Batt-Rawden, first-hand experience of the disease should be enough to convince people that they need to be vaccinated (Reference Batt-RawdenBatt-Rawden 2021):
I’ve seen first hand the damage the virus can do. I’ve watched it rip through whole families after they had been mixing at Christmas. Whole generations – gone. If you had seen what I have, you would be first in line for the vaccine too.
And yet, a recent study that attempted to establish what factors determine acceptance rates of Covid-19 vaccines surprisingly found that those ‘who reported COVID-19 sickness in themselves or family members were no more likely to respond positively’ to the question of whether they would accept vaccination than those who hadn’t experienced the illness first hand. At the same time, those ‘who said that they trusted their government were more likely to accept a vaccine than those who said that they did not’ (Reference Lazarus, Ratzan and PalayewLazarus et al. 2021:226). Indeed, countries where levels of acceptance were above 80% ‘tended to be Asian nations with strong trust in central governments (China, South Korea and Singapore)’ (Reference Lazarus, Ratzan and PalayewLazarus et al. 2021:226). In France, by contrast, confidence in medical science has declined following various scandals involving the government and drug companies. ‘The most famous of these’, according to a Foreign Policy report which suggests this to be the ‘real reason France is skeptical of vaccines’, concerns ‘the diabetes drug Mediator, which was marketed as a weight loss pill and has been linked to the deaths of as many as 2,000 people’ (Reference ChabalChabal 2021). In many cases, therefore, lack of trust in Covid-19 vaccines among particular populations has less to do with the vaccines themselves than with a lack of trust in the governments, healthcare systems and pharmaceutical companies that promote them (Figure 5.5). As pointed out in a 2019 editorial in The Lancet Infectious Disease,Footnote 24 this distrust is far from irrational, even by the traditional view of rationality that we question here. The editorial argues, for instance, that reluctance to seek proper care during the Ebola outbreak in the Democratic Republic of Congo and the uncontrolled transmission that it provoked was due to a deep distrust in the government that followed from years of neglect and corruption. It concludes that ‘a belief that vaccines cause autism or that Ebola is a government ploy likely has as much to do with wider grievances and distrust of authority as with the specifics of the scientific evidence and education’. Stories of abuse of authority on the part of governments and other institutions ring true because they resonate with people’s previous experiences or with stories they have been told by their friends and family – those with whom they identify and can trust. And they have a long history: John Gibbs’s 1854 treaty against compulsory vaccination, Our Medical Liberties, complained – among other things – that the Vaccination Act of 1853 ‘was written to benefit the medical trade’, not the populace (PopMatters 2020).
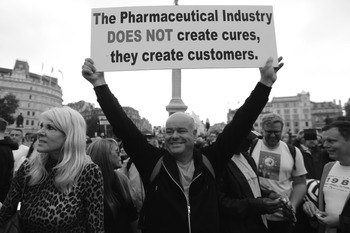
Figure 5.5 Anti-lockdown and anti-vaccine protest in London July 2021.
Reference Jamison, Quinn and FreimuthJamison et al. (2019) explored the levels of trust in pharmaceutical companies and government agencies that promote them among White and African American adults, focusing on the influenza vaccine. The study shows that pharmaceutical companies are widely distrusted: ‘Individuals suspect that the motives governing these institutions are more aligned to generating profit than serving the public good and that pharmaceutical profits corrupt the entire healthcare industry’ (Reference Jamison, Quinn and FreimuthJamison et al. 2019:92). Perhaps most importantly, the study also confirms that the racialized history of American healthcare continues to impact institutional trust among African Americans. Many researchers have documented ways in which the African American population is treated differently from White patients in the USA. Annual reports from the Agency for Healthcare Research and Quality show that 40% of the measured health quality outcomes were more negative for African Americans than the White population (AHRQ 2018). Profound distrust in the motives of health institutions among the Black population is also rooted in history. An extreme example of the kind of systemic racism this part of the population has suffered is the so-called Tuskegee Syphilis Study, which was conducted between 1932 and 1972 by the United States Public Health Service and the Centers for Disease Control and Prevention on a group of nearly 400 African Americans with syphilis. Participants were told that they were receiving free medical care; in fact, they were merely being observed for a study of untreated syphilis. Dozens died as a result (Reference KumKum 2020). In Pakistan, one of the few countries where polio has not yet been eradicated and where those attempting to administer the polio vaccine are often violently attacked, 49% of the population are reported to refuse Covid-19 vaccination (Reference SiddiquiSiddiqui 2021). This is not difficult to understand given that while hunting for Osama Bin Laden as recently as 2011 the US Central Intelligence Agency organized a fake vaccination programme against hepatitis B, beginning with poorer neighbourhoods which were more likely to be hiding their target (Reference SiddiquiSiddiqui 2021), and used that campaign as a cover to collect DNA samples that eventually confirmed his location (Reference CarrCarr 2021).
Recent studies have shown that Covid-19 vaccine hesitancy is particularly prevalent amongst Black, Asian and minority ethnic (BAME) populations, and that some of this hesitancy is ‘likely grounded in a long history of structurally racist systems which have led to health inequalities and injustices’ (Reference Forman, Shah, Jeurissen, Jit and MossialosForman et al. 2021). Even though a given Black person may never have been subjected to the kind of extreme racism described in these narratives, they will still be apprehensive about health authorities and institutions because they will see themselves as part of that group and hence a potential target of discrimination. Reference MorganMorgan (2021) shows how this kind of reasoning influenced the response among people from BAME groups when the medical authorities proposed starting the vaccine roll-out with the most vulnerable communities during the first wave of the pandemic:
This caused concern among these communities, because they are not normally at the front of the queue when it comes to the best medical treatments, particularly those in lower socioeconomic classes. Some people began to speculate that it was because it was an experimental vaccine and Black people were being used as guinea pigs.
Reference MorganMorgan (2021) concludes that for some, ‘this will have triggered alarm bells and brought up the many historical examples of Black people being used for experimental or unethical medical treatments’.
Forman et al. report that numerous surveys conducted in the UK, USA and several other countries found that respondents from historically marginalized groups, such as the BAME community, ‘are less likely to accept the [Covid-19] vaccine compared to White counterparts’ (Reference Forman, Shah, Jeurissen, Jit and MossialosForman et al. 2021:561); they suggest that this is at least due to ‘distrust of the medical profession’ that is ‘grounded in a long history of structurally racist systems which have led to health inequalities and injustices’ (Reference Forman, Shah, Jeurissen, Jit and MossialosForman et al. 2021:561). Native Americans are similarly reported to have grave concerns about vaccination. These concerns are rooted in a parallel history of discrimination that featured, among other things, the sterilization of at least 25% of all Native women of childbearing age in the 1970s (Reference TheobaldTheobald 2019). No wonder, with such a history, that resistance against polio vaccines which extended into an 11-months boycott in Nigeria was fuelled by rumours that ‘vaccines from the West were sterilizing children, particularly in light of the post-911 war on terrorism interpreted as a war on Muslims’ (Reference LarsonLarson 2020:xxx). Israel eventually admitted in 2013 that it had been ‘sterilizing’ Jewish immigrants from Ethiopia, without their knowledge or consent, by injecting them every three months with Depo-Provera, a highly effective and long-lasting contraceptive (Reference DawberDawber 2013). The women thought they were being inoculated. Reference LarsonLarson (2020) confirms that there is a persistent association of vaccines in general with attempts to sterilize various populations, although the vaccine against tetanus tends to cause more apprehension given that it focuses primarily on girls and pregnant women.
The obvious overlap among the various issues raised throughout this chapter aside, what they all demonstrate is that our decision to trust or mistrust a given source of evidence is guided by what we have called, following Fisher, narrative rationality. It is narrative rationality – rather than scientific ‘proof’ – that determines whether or not the evidence itself is accepted as reliable and acted upon accordingly. The argument at the end of the day is not between science and heresy, or rational human beings and conspiracy theorists, but between trust and non-trust, between identification and non-identification, in the course of a complex life lived with diverse others.






 Open access
Open access