



Introduction
Bipolar disorders (BD) are severe mental disorders that are characterised by depressed and hypomanic/manic episodes, with varying degrees of euthymia in between mood episodes. The lifetime prevalence of BD is estimated to be 1–3% (Merikangas et al., Reference Merikangas, Jin, He, Kessler, Lee, Sampson and Zarkov2011; Rowland & Marwaha, Reference Rowland and Marwaha2018). BD is subdivided based on the severity of the elevated mood into BD type I (BDI), which is characterised by manic episodes, and BD type II (BDII), which is characterised by hypomanic episodes. Psychotic symptoms, such as delusions and hallucinations, are common, particularly in manic episodes of BDI (Goodwin & Jamison, Reference Goodwin and Jamison2007). Although per their definition psychotic symptoms are incompatible with hypomania and euthymia, the prevalence of psychotic symptoms appears to vary between the other different types of mood episodes, that is, mania, mixed episodes and depression.
There are indications that psychotic BD is more severe than nonpsychotic BD, presenting with a poorer functional outcome (Bonnín et al., Reference Bonnín, Jiménez, Solé, Torrent, Radua, Reinares and Vieta2019), treatment adherence (Martinez-Aran et al., Reference Martinez-Aran, Scott, Colom, Torrent, Tabares-Seisdedos, Daban and Vieta2009) and lithium response (Hui et al., Reference Hui, Kandola, Shen, Lewis, Osborn, Geddes and Hayes2019). There are also indications of larger cognitive impairments in psychotic BD compared with nonpsychotic BD, but the findings are inconsistent (Bora, Reference Bora2018). Patients with psychotic BD also seem to have an increased suicide rate, poorer general health and more comorbid somatic illnesses (Baldessarini & Tondo, Reference Baldessarini and Tondo2020; Schaffer et al., Reference Schaffer, Isometsä, Tondo, Moreno, Sinyor, Kessing and Yatham2015). Thus, psychotic symptoms appear to be an important predictor of the clinical outcome of BD. However, the reported prevalence of psychotic symptoms in BD patients varies because of differences in sampling and other methodological issues.
To the best of our knowledge, only one previous systematic review has been published on psychotic symptoms in BD. This review dates from 2007 covering studies intil 2005, with the reported pooled lifetime prevalence of 60% mainly based on inpatient data from patients with mania (Goodwin & Jamison).
Many new studies have been published on BD since then, including information on different subtypes and on different polarities other than mania. Thus, our aim is to systematically review and meta-analyse the lifetime prevalence (‘history of psychosis’) and point prevalence (‘current psychotic symptoms’) in BD, hence differentiating between types of BD (BDI v. BDII), mood episodes (manic, depressive or mixed sample), setting (patient samples such as inpatient and outpatient settings, as well as from the general population in community samples) and diagnostic system used (ICD v. DSM) for when there are available data.
Methods
Protocol and registration
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, see online for Supplementary Material 1a & 1b: PRISMA 2020 Abstract checklist and Checklist. The search protocol was prospectively published in PROSPERO, project number CRD42017052706 (Aminoff, Melle, Ødegaard, & Onyeka, Reference Aminoff, Melle, Ødegaard and Onyeka2017).
Search strategy
A literature search was conducted with assistance from a senior librarian (MØ) at the Medical Library at the University of Oslo. We searched Medline, Embase, PsycINFO (Ovid interface) and Cochrane Library (Wiley) on 5 August 2021; no date limitation was set. The search was limited to English, Norwegian, Danish and Swedish. Both text words and subject headings were used. The search terms were variations of ‘bipolar disorder’, ‘hypomanic’, ‘manic’ or ‘cyclothymic’; combined with either ‘psychotic’, ‘psychosis’, ‘hearing voices’, ‘auditory hallucinations’, ‘paranoid behaviour’ or ‘delusion’; and ‘adults’. After removing duplicates, a total of 2807 references were included for further screening. The search is published online on Open Science Framwork (OSF) in accordance with PRISMA 2020 recommendations, see (Ødegaard & Aminoff, Reference Ødegaard and Aminoff2022).
Inclusion and exclusion criteria
The inclusion criteria for the systematic review and meta-analyses were as follows: (1) published papers containing data on patients with (BDI, BDII or BD not otherwise specified); (2) restricted to adult BD (aged 18–64 years); (3) papers written in English or a Scandinavian language and (4) studies that reported a proportion of current psychotic symptoms or history of psychotic symptoms. Psychotic symptoms were limited to hallucinations or delusions; however, there were no rules for how the presence of psychotic symptoms should be assessed; 5) we included both observational and experimental studies, all considered cross-sectional due to the nature of the data.
The exclusion criteria were as follows: studies with (1) preselected groups or matching to ensure equal proportions of psychotic and nonpsychotic BD; (2) unknown proportions of schizoaffective disorder bipolar type included in the sample; (3) unknown distribution of BDI v. BDII patients in sample; (4) too broad or narrow definition of psychotic symptoms (e.g. limited to mood-incongruent delusions or including disorganised symptoms); (5) conference abstracts; (6) papers where the presence of psychotic symptoms were not mentioned in abstract and (7) studies not subject to peer review.
Many studies did not report the age groups included. In such cases, the mean age was identified, and if the patient population based on this seemed most likely to be between 18 and 64 years, the studies were included. If the mean age was higher than 50 years, with large standard deviations of more than 15 years, the studies were excluded.
Samples and types of studies
There were no limitations regarding the type of study population; thus, the current study included a broad range of studies from a variety of settings. We also included studies that established the diagnosis in different ways, varying from standard clinical diagnoses with estimations of psychotic symptoms through chart reviews and registers to diagnostic and symptom assessment procedures using structured interviews and rating scales. Evaluation of the quality of data was, however, conducted and taken into consideration in the review process and in the analyses.
Study selection, data extraction and data analysis
The retrieved records were first screened by title and abstracts, and the full text was subsequently read for relevance using the predefined inclusion criteria, which was done independently by two of the authors (INO and SRA). Any disagreements or discrepancies were resolved through discussions until consensus was reached (six studies). If there was more than one study reporting from the same sample, we excluded the smallest or one with the least amount of descriptive information. Author SRA extracted data from each study using a data extraction form, including information about the country where the study was conducted, study characteristics, participant characteristics, diagnostic system and diagnostic procedure, type of BD, the method for assessment of psychotic symptoms and the proportion of either a history of psychosis or current psychotic symptoms or both.
Quality assessment
Quality assessment was done using the Newcastle–Ottawa Scale for cross-sectional studies (Wells et al., Reference Wells, Shea, O'Connell, Peterson, Welch, Losos and Tugwell2000), which was customised to fit the purpose of the present study. The adaptation of the scale is available online as Supplementary Material 2: Adapted Newcastle Ottawa Scale. The rating was performed by two independent raters, where the first author evaluated all studies and the co-authors IM, INO, TVL, OAA, KLR and CS each assessed a proportion of the studies. Each study was assigned a score between 0 and 7, where studies with a score of 3 or less were considered being a low quality, 4–5 moderate quality and 6–7 high quality. In the case of discrepancies between the raters, the quality ratings were discussed, and a consensus rating was assigned. Studies of low quality were included in the overall meta-analyses, but follow-up analyses were made to investigate to what extent the results changed if the low-quality studies were removed. The quality assessment can be found online in Supplementary Material 3: Quality Assessment of included studies.
Analysis
Meta-analyses were performed using Comprehensive Meta-Analysis version 3 software (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2013). The pooled lifetime and point prevalence of psychotic symptoms were calculated using random effects meta-analysis, here expressed as percentage and 95% confidence interval (CI). Heterogeneity between studies was measured using the I 2 statistic, which describes the proportion of total variance attributed to variance in the true effect (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2009).
For estimates of the point and lifetime prevalence, we performed two main meta-analyses on the samples based on DSM and ICD diagnoses separately. There were too few ICD studies for further subgroup analyses. The DSM sample was divided into subgroup analyses, whenever data were available, and this was based on the subtype of BD (BDI, BDII), patient setting (inpatient, outpatient and community setting) and symptom presentation (mania, mixed or depression).
We performed sensitivity analyses in which we removed studies of low quality, with unstructured diagnostic assessment and/or unclear age range in the studies and looked for major changes in the results.
Assessment of publication bias
Publication bias was assessed for each group of studies by visual inspection of funnel plots with trim and fill adjustment. Whenever a funnel plot showed indices of asymmetry and the Egger test was significant, we performed subgroup analyses (Borenstein et al., Reference Borenstein, Hedges, Higgins and Rothstein2009).
Results
Search results
Figure 1 shows our searches and selection of relevant papers. From the original 2807 studies, after screening by two independent researchers (SRA and INO), a total of 624 studies were selected for reading the full text, and data were finally extracted from 297 studies after reading the full-text papers. In the end, we included 78 studies.
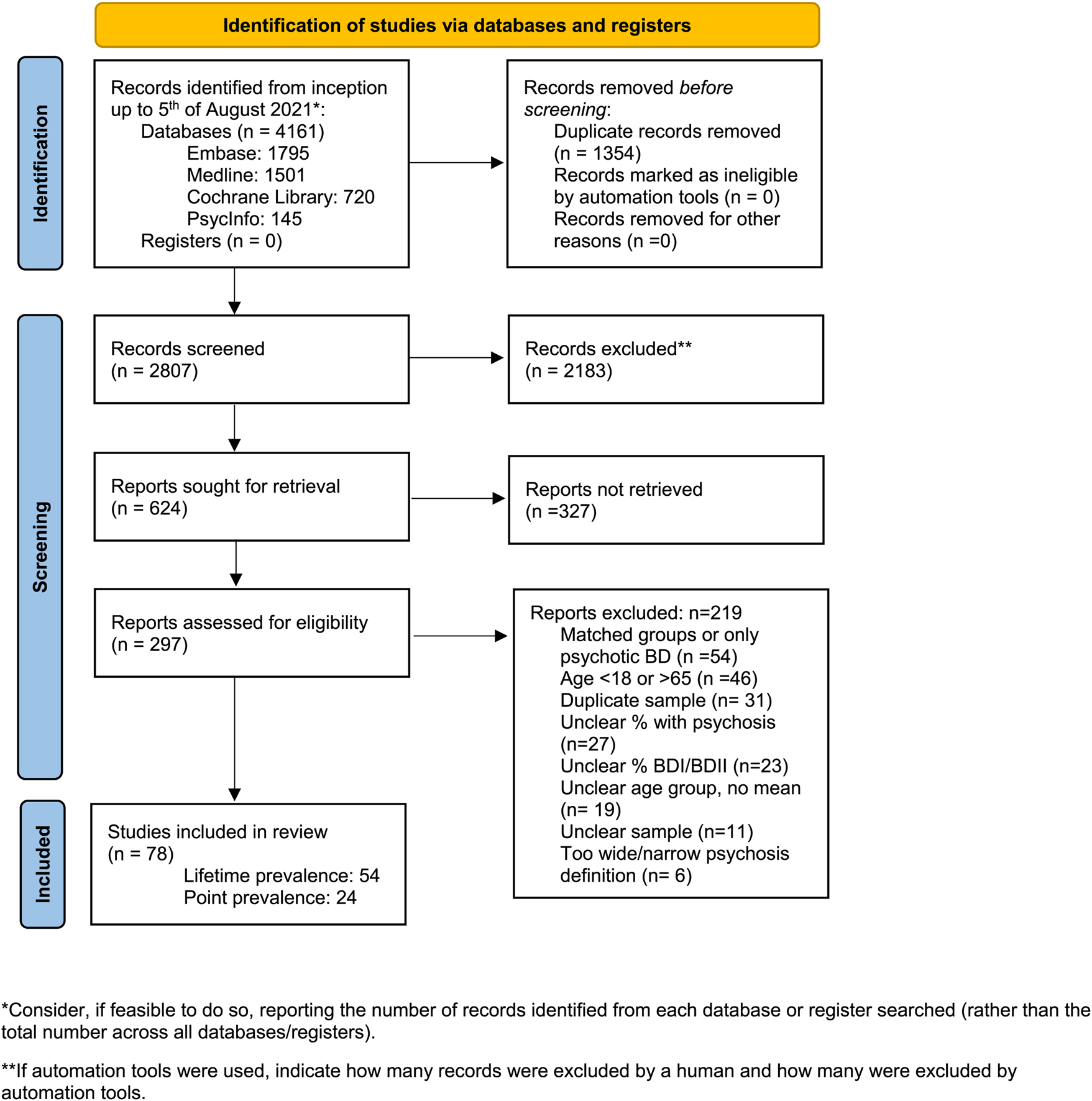
Fig. 1. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
There were 54 studies (n = 23 461) reporting data on the lifetime prevalence of psychotic symptoms in BD, for an overview of included studies see online Supplementary Material 4: Studies included in the meta-analyses of the lifetime prevalence of psychotic symptoms in bipolar disorders (Aedo et al., Reference Aedo, Murru, Sanchez, Grande, Vieta and Undurraga2018; Altindag, Yanik, & Nebioglu, Reference Altindag, Yanik and Nebioglu2006; Atagun et al., Reference Atagun, Sikoglu, Can, Ugurlu, Kaymak, Caykoylu and Ongur2018; Balzafiore et al., Reference Balzafiore, Rasgon, Yuen, Shah, Kim, Goffin and Ketter2017; Berkol, Kirli, Islam, Pinarbasi, & Ozyildirim, Reference Berkol, Kirli, Islam, Pinarbasi and Ozyildirim2016; Bolhuis et al., Reference Bolhuis, Lang, Gyllenberg, Kaariala, Veijola, Gissler and Kelleher2021; Burton et al., Reference Burton, Ryan, Kamali, Marshall, Harrington, McInnis and Tso2018; Cao et al., Reference Cao, Deng, Guan, Yang, Lin, Ma and Hu2014; Davila et al., Reference Davila, Zumarraga, Basterreche, Arrue, Zamalloa and Anguiano2006; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010, Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Ernst & Goldberg, Reference Ernst and Goldberg2004; Finseth, Morken, Andreassen, Malt, & Vaaler, Reference Finseth, Morken, Andreassen, Malt and Vaaler2012; Fuentes, Rizo-Mendez, & Jarne-Esparcia, Reference Fuentes, Rizo-Mendez and Jarne-Esparcia2016; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Goldberg et al., Reference Goldberg, Garno, Portera, Leon, Kocsis and Whiteside1999; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Grande et al., Reference Grande, Sanchez-Moreno, Sole, Jimenez, Torrent, Bonnin and Martinez-Aran2017; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Jamra et al., Reference Jamra, Schulze, Becker, Brockschmidt, Green, Alblas and Schumacher2010; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Kent et al., Reference Kent, Disner, Van Voorhis, Urosevic, Caligiuri and Sponheim2020; Kirov & Murray, Reference Kirov and Murray1999; Knorr et al., Reference Knorr, Miskowiak, Akhoj, Vinberg, Forman and Kessing2021; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Lee & Kim, Reference Lee and Kim2011; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Miller et al., Reference Miller, Do, Gershon, Wang, Hooshmand, Chang and Ketter2018; Moon et al., Reference Moon, Chang, Kim, Seo, Cha, Ha and Ha2012; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Neves, Malloy-Diniz, Barbosa, Brasil, & Correa, Reference Neves, Malloy-Diniz, Barbosa, Brasil and Correa2009; Newport et al., Reference Newport, Baldessarini, Knight, Fernandez, Morris, Viguera and Stowe2012; Ong et al., Reference Ong, Walterfang, Malhi, Styner, Velakoulis and Pantelis2012; Ortiz et al., Reference Ortiz, Bradler, Moorti, MacLean, Husain, Sanches and Mulsant2021; Østergaard, Bertelsen, Nielsen, Mors, & Petrides, Reference Østergaard, Bertelsen, Nielsen, Mors and Petrides2013; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Parker et al., Reference Parker, Graham, Hadzi-Pavlovic, McCraw, Hong and Friend2013, Reference Parker, Tavella, Ricciardi, Hadzi-Pavlovic, Alda, Hajek and Manicavasagar2020; Patterson, Sandman, Ring, Jin, & Bunney, Reference Patterson, Sandman, Ring, Jin and Bunney2009; Prabhavathy, Kuruvilla, Ravindren, Ganesh, & Midhun, Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sanchez-Morla et al., Reference Sanchez-Morla, Lopez-Villarreal, Jimenez-Lopez, Aparicio, Martinez-Vizcaino, Roberto and Santos2019; Sarrazin et al., Reference Sarrazin, Cachia, Hozer, McDonald, Emsell, Cannon and Houenou2018; Savitz et al., Reference Savitz, Dantzer, Wurfel, Victor, Ford, Bodurka and Drevets2015; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011; Talati et al., Reference Talati, Bao, Kaufman, Shen, Schaefer and Brown2013; Tost et al., Reference Tost, Ruf, Schmal, Schulze, Knorr, Vollmert and Rietschel2010; Trotti et al., Reference Trotti, Parker, Sabatinelli, Tamminga, Gershon, Keedy and Clementz2020; Tundo et al., Reference Tundo, Musetti, Benedetti, Berti, Massimetti and Dell'Osso2015; Van Der Werf-Eldering et al., Reference Van Der Werf-Eldering, Van Der Meer, Burger, Holthausen, Nolen and Aleman2011; Van Rheenen et al., Reference Van Rheenen, Lewandowski, Tan, Ospina, Ongur, Neill and Burdick2017; Yazici, Kora, Ucok, Tunali, & Turan, Reference Yazici, Kora, Ucok, Tunali and Turan1999; Yilmaz, Yavuz, Altinbas, Lordoglu, & Kurt, Reference Yilmaz, Yavuz, Altinbas, Lordoglu and Kurt2015).
There were 24 studies reporting data on the point prevalence of psychotic symptoms in BD. For an overview of included studies, see online Supplementay Material 5: Studies included in the meta-analyses of the point prevalence of psychotic symptoms in bipolar disorders (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Asaad et al., Reference Asaad, Okasha, Ramy, Fekry, Zaki, Azzam and Ahmed2014; Azorin, Adida, & Belzeaux, Reference Azorin, Adida and Belzeaux2015; Azorin, Akiskal, & Hantouche, Reference Azorin, Akiskal and Hantouche2006; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Benazzi, Reference Benazzi2001; Bonnin et al., Reference Bonnin, Reinares, Hidalgo-Mazzei, Undurraga, Mur, Saez and Vieta2015; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017; Carroll, Vohs, O'Donnell, Shekhar, & Hetrick, Reference Carroll, Vohs, O'Donnell, Shekhar and Hetrick2007; Ciapparelli et al., Reference Ciapparelli, Dell'Osso, Tundo, Pini, Chiavacci, Di Sacco and Cassano2001; Fiedorowicz et al., Reference Fiedorowicz, Endicott, Leon, Solomon, Keller and Coryell2011; Goldberg & Harrow, Reference Goldberg and Harrow2004; Guven, Kesebir, Demirer, & Bilici, Reference Guven, Kesebir, Demirer and Bilici2015; Kessing, Reference Kessing2004; Kessing, Jensen, & Christensen, Reference Kessing, Jensen and Christensen2008; Levy & Weiss, Reference Levy and Weiss2010; Lindenmayer, Bossie, Kujawa, Zhu, & Canuso, Reference Lindenmayer, Bossie, Kujawa, Zhu and Canuso2008; Lundin, Bartolomeo, O'Donnell, & Hetrick, Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Novis et al., Reference Novis, Cirillo, Da Silva, Santos, Silveira, Cardoso and Cheniaux2014; Reddy, Meyer, Wittlin, Miller, & Weinstock, Reference Reddy, Meyer, Wittlin, Miller and Weinstock2017; Salem et al., Reference Salem, Ruiz, Hernandez, Wahid, Cao, Karnes and Pigott2019; Samalin et al., Reference Samalin, Llorca, Giordana, Milhiet, Yon, El-Hage and Bellivier2014; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007; Yildiz, Guleryuz, Ankerst, Ongur, & Renshaw, Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
Lifetime prevalence of psychotic symptoms in BD
The characteristics of the included studies giving data for lifetime prevalence are shown in the online Supplementary Material 4. Among these 54 studies, 26 were conducted in Europe, 17 in the Americas, 4 in Asia and 3 in Australia, and four of the studies included participants from multiple countries. The studies' quality assessment scores ranged from 2 to 7. A total of 13 (24%) studies were of low quality, 34 (63%) were of moderate quality and 7 (13%) were of high quality (Table 1).
Table 1. Results from meta-analyses of the prevalence of psychotic symptoms in bipolar disorders
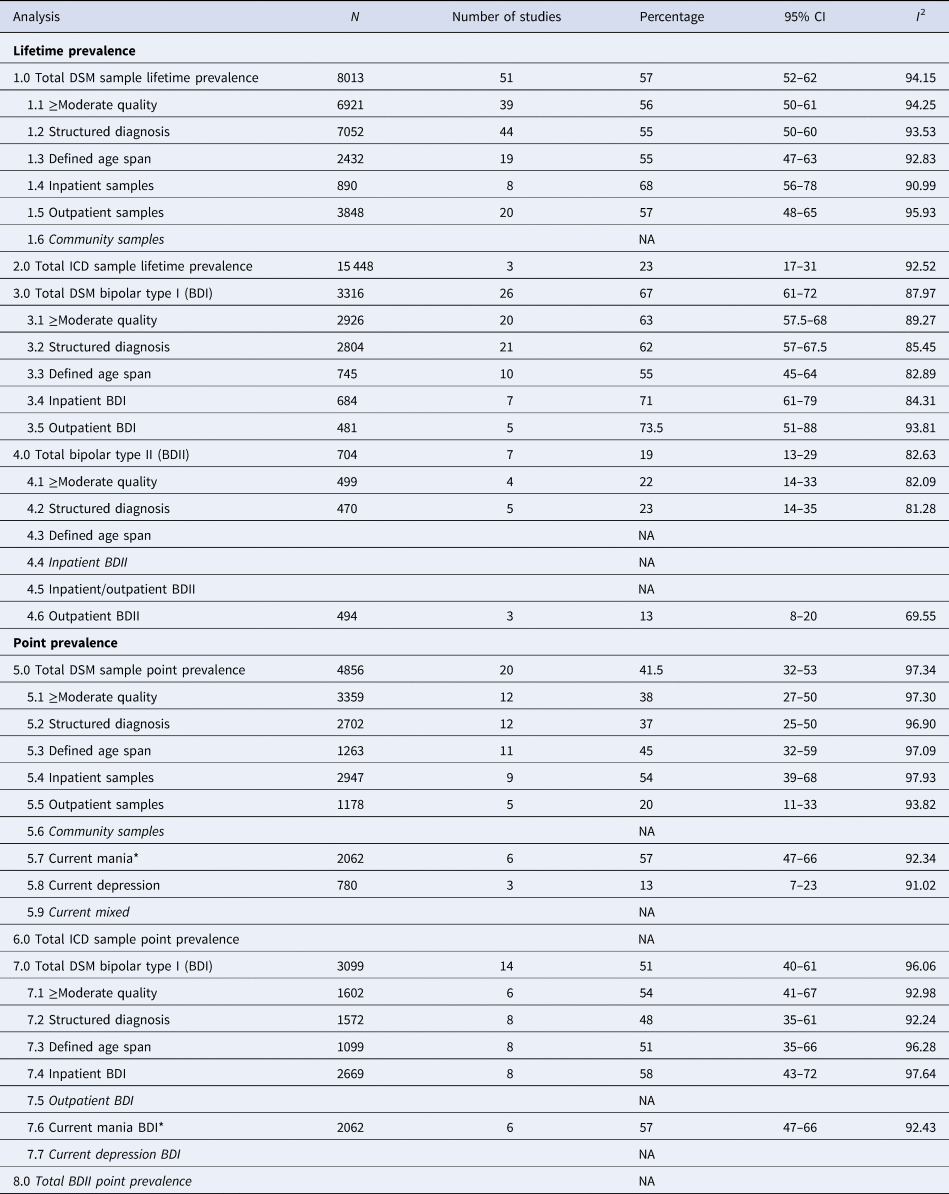
DSM, Diagnostic and Statistical Manual of Mental Disorders; ICD, International Classification of Diseases and Related Health Problems; NA, not applicable.
*Same analysis.
The pooled lifetime prevalence of psychotic symptoms in the 51 included DSM BD studies (N = 8013) was 57% (95% CI 52–62) (Aedo et al., Reference Aedo, Murru, Sanchez, Grande, Vieta and Undurraga2018; Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Atagun et al., Reference Atagun, Sikoglu, Can, Ugurlu, Kaymak, Caykoylu and Ongur2018; Balzafiore et al., Reference Balzafiore, Rasgon, Yuen, Shah, Kim, Goffin and Ketter2017; Berkol et al., Reference Berkol, Kirli, Islam, Pinarbasi and Ozyildirim2016; Burton et al., Reference Burton, Ryan, Kamali, Marshall, Harrington, McInnis and Tso2018; Cao et al., Reference Cao, Deng, Guan, Yang, Lin, Ma and Hu2014; Davila et al., Reference Davila, Zumarraga, Basterreche, Arrue, Zamalloa and Anguiano2006; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010, Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Ernst & Goldberg, Reference Ernst and Goldberg2004; Finseth et al., Reference Finseth, Morken, Andreassen, Malt and Vaaler2012; Fuentes et al., Reference Fuentes, Rizo-Mendez and Jarne-Esparcia2016; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Goldberg et al., Reference Goldberg, Garno, Portera, Leon, Kocsis and Whiteside1999; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Grande et al., Reference Grande, Sanchez-Moreno, Sole, Jimenez, Torrent, Bonnin and Martinez-Aran2017; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Jamra et al., Reference Jamra, Schulze, Becker, Brockschmidt, Green, Alblas and Schumacher2010; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Kent et al., Reference Kent, Disner, Van Voorhis, Urosevic, Caligiuri and Sponheim2020; Kirov & Murray, Reference Kirov and Murray1999; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Lee & Kim, Reference Lee and Kim2011; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Miller et al., Reference Miller, Do, Gershon, Wang, Hooshmand, Chang and Ketter2018; Moon et al., Reference Moon, Chang, Kim, Seo, Cha, Ha and Ha2012; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Neves et al., Reference Neves, Malloy-Diniz, Barbosa, Brasil and Correa2009; Newport et al., Reference Newport, Baldessarini, Knight, Fernandez, Morris, Viguera and Stowe2012; Ong et al., Reference Ong, Walterfang, Malhi, Styner, Velakoulis and Pantelis2012; Ortiz et al., Reference Ortiz, Bradler, Moorti, MacLean, Husain, Sanches and Mulsant2021; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Parker et al., Reference Parker, Graham, Hadzi-Pavlovic, McCraw, Hong and Friend2013, Reference Parker, Tavella, Ricciardi, Hadzi-Pavlovic, Alda, Hajek and Manicavasagar2020; Patterson et al., Reference Patterson, Sandman, Ring, Jin and Bunney2009; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sanchez-Morla et al., Reference Sanchez-Morla, Lopez-Villarreal, Jimenez-Lopez, Aparicio, Martinez-Vizcaino, Roberto and Santos2019; Sarrazin et al., Reference Sarrazin, Cachia, Hozer, McDonald, Emsell, Cannon and Houenou2018; Savitz et al., Reference Savitz, Dantzer, Wurfel, Victor, Ford, Bodurka and Drevets2015; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011; Talati et al., Reference Talati, Bao, Kaufman, Shen, Schaefer and Brown2013; Tost et al., Reference Tost, Ruf, Schmal, Schulze, Knorr, Vollmert and Rietschel2010; Trotti et al., Reference Trotti, Parker, Sabatinelli, Tamminga, Gershon, Keedy and Clementz2020; Tundo et al., Reference Tundo, Musetti, Benedetti, Berti, Massimetti and Dell'Osso2015; Van Der Werf-Eldering et al., Reference Van Der Werf-Eldering, Van Der Meer, Burger, Holthausen, Nolen and Aleman2011; Van Rheenen et al., Reference Van Rheenen, Lewandowski, Tan, Ospina, Ongur, Neill and Burdick2017; Yazici et al., Reference Yazici, Kora, Ucok, Tunali and Turan1999; Yilmaz et al., Reference Yilmaz, Yavuz, Altinbas, Lordoglu and Kurt2015).
Of these, in 39 studies with at least moderate quality (n = 6921), the pooled prevalence was 56% (95% CI 50–61) (Aedo et al., Reference Aedo, Murru, Sanchez, Grande, Vieta and Undurraga2018; Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Balzafiore et al., Reference Balzafiore, Rasgon, Yuen, Shah, Kim, Goffin and Ketter2017; Berkol et al., Reference Berkol, Kirli, Islam, Pinarbasi and Ozyildirim2016; Burton et al., Reference Burton, Ryan, Kamali, Marshall, Harrington, McInnis and Tso2018; Cao et al., Reference Cao, Deng, Guan, Yang, Lin, Ma and Hu2014; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010; Dell'Osso et al., Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Finseth et al., Reference Finseth, Morken, Andreassen, Malt and Vaaler2012; Fuentes et al., Reference Fuentes, Rizo-Mendez and Jarne-Esparcia2016; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Goldberg et al., Reference Goldberg, Garno, Portera, Leon, Kocsis and Whiteside1999; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Grande et al., Reference Grande, Sanchez-Moreno, Sole, Jimenez, Torrent, Bonnin and Martinez-Aran2017; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Jamra et al., Reference Jamra, Schulze, Becker, Brockschmidt, Green, Alblas and Schumacher2010; Karakus & Tamam, Reference Karakus and Tamam2011; Kirov & Murray, Reference Kirov and Murray1999; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Lee & Kim, Reference Lee and Kim2011; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Miller et al., Reference Miller, Do, Gershon, Wang, Hooshmand, Chang and Ketter2018; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Neves et al., Reference Neves, Malloy-Diniz, Barbosa, Brasil and Correa2009; Newport et al., Reference Newport, Baldessarini, Knight, Fernandez, Morris, Viguera and Stowe2012; Ong et al., Reference Ong, Walterfang, Malhi, Styner, Velakoulis and Pantelis2012; Ortiz et al., Reference Ortiz, Bradler, Moorti, MacLean, Husain, Sanches and Mulsant2021; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Patterson et al., Reference Patterson, Sandman, Ring, Jin and Bunney2009; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sanchez-Morla et al., Reference Sanchez-Morla, Lopez-Villarreal, Jimenez-Lopez, Aparicio, Martinez-Vizcaino, Roberto and Santos2019; Sarrazin et al., Reference Sarrazin, Cachia, Hozer, McDonald, Emsell, Cannon and Houenou2018; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011; Talati et al., Reference Talati, Bao, Kaufman, Shen, Schaefer and Brown2013; Trotti et al., Reference Trotti, Parker, Sabatinelli, Tamminga, Gershon, Keedy and Clementz2020; Tundo et al., Reference Tundo, Musetti, Benedetti, Berti, Massimetti and Dell'Osso2015; Van Rheenen et al., Reference Van Rheenen, Lewandowski, Tan, Ospina, Ongur, Neill and Burdick2017; Yazici et al., Reference Yazici, Kora, Ucok, Tunali and Turan1999).
In the 44 studies that used structured diagnostic instruments (n = 7052), the pooled prevalence was 55% (95% CI 47–63) (Aedo et al., Reference Aedo, Murru, Sanchez, Grande, Vieta and Undurraga2018; Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Atagun et al., Reference Atagun, Sikoglu, Can, Ugurlu, Kaymak, Caykoylu and Ongur2018; Balzafiore et al., Reference Balzafiore, Rasgon, Yuen, Shah, Kim, Goffin and Ketter2017; Berkol et al., Reference Berkol, Kirli, Islam, Pinarbasi and Ozyildirim2016; Burton et al., Reference Burton, Ryan, Kamali, Marshall, Harrington, McInnis and Tso2018; Cao et al., Reference Cao, Deng, Guan, Yang, Lin, Ma and Hu2014; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010, Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Ernst & Goldberg, Reference Ernst and Goldberg2004; Finseth et al., Reference Finseth, Morken, Andreassen, Malt and Vaaler2012; Fuentes et al., Reference Fuentes, Rizo-Mendez and Jarne-Esparcia2016; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Grande et al., Reference Grande, Sanchez-Moreno, Sole, Jimenez, Torrent, Bonnin and Martinez-Aran2017; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Jamra et al., Reference Jamra, Schulze, Becker, Brockschmidt, Green, Alblas and Schumacher2010; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Kent et al., Reference Kent, Disner, Van Voorhis, Urosevic, Caligiuri and Sponheim2020; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Lee & Kim, Reference Lee and Kim2011; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Miller et al., Reference Miller, Do, Gershon, Wang, Hooshmand, Chang and Ketter2018; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Neves et al., Reference Neves, Malloy-Diniz, Barbosa, Brasil and Correa2009; Newport et al., Reference Newport, Baldessarini, Knight, Fernandez, Morris, Viguera and Stowe2012; Ong et al., Reference Ong, Walterfang, Malhi, Styner, Velakoulis and Pantelis2012; Ortiz et al., Reference Ortiz, Bradler, Moorti, MacLean, Husain, Sanches and Mulsant2021; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Patterson et al., Reference Patterson, Sandman, Ring, Jin and Bunney2009; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sanchez-Morla et al., Reference Sanchez-Morla, Lopez-Villarreal, Jimenez-Lopez, Aparicio, Martinez-Vizcaino, Roberto and Santos2019; Sarrazin et al., Reference Sarrazin, Cachia, Hozer, McDonald, Emsell, Cannon and Houenou2018; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011; Talati et al., Reference Talati, Bao, Kaufman, Shen, Schaefer and Brown2013; Tost et al., Reference Tost, Ruf, Schmal, Schulze, Knorr, Vollmert and Rietschel2010; Trotti et al., Reference Trotti, Parker, Sabatinelli, Tamminga, Gershon, Keedy and Clementz2020; Tundo et al., Reference Tundo, Musetti, Benedetti, Berti, Massimetti and Dell'Osso2015; Van Der Werf-Eldering et al., Reference Van Der Werf-Eldering, Van Der Meer, Burger, Holthausen, Nolen and Aleman2011; Van Rheenen et al., Reference Van Rheenen, Lewandowski, Tan, Ospina, Ongur, Neill and Burdick2017; Yazici et al., Reference Yazici, Kora, Ucok, Tunali and Turan1999).
In the 19 studies that stated the age span of included patients (n = 2432), the pooled prevalence was 56% (95% CI 50–61) (Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Berkol et al., Reference Berkol, Kirli, Islam, Pinarbasi and Ozyildirim2016; Davila et al., Reference Davila, Zumarraga, Basterreche, Arrue, Zamalloa and Anguiano2006; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010; Finseth et al., Reference Finseth, Morken, Andreassen, Malt and Vaaler2012; Fuentes et al., Reference Fuentes, Rizo-Mendez and Jarne-Esparcia2016; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Newport et al., Reference Newport, Baldessarini, Knight, Fernandez, Morris, Viguera and Stowe2012; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sanchez-Morla et al., Reference Sanchez-Morla, Lopez-Villarreal, Jimenez-Lopez, Aparicio, Martinez-Vizcaino, Roberto and Santos2019; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011; Tundo et al., Reference Tundo, Musetti, Benedetti, Berti, Massimetti and Dell'Osso2015; Van Der Werf-Eldering et al., Reference Van Der Werf-Eldering, Van Der Meer, Burger, Holthausen, Nolen and Aleman2011; Van Rheenen et al., Reference Van Rheenen, Lewandowski, Tan, Ospina, Ongur, Neill and Burdick2017).
Only three studies included samples based on ICD-10 diagnoses (N = 15 448). Here, the pooled lifetime prevalence was 23% (95% CI 17–31) (Bolhuis et al., Reference Bolhuis, Lang, Gyllenberg, Kaariala, Veijola, Gissler and Kelleher2021; Knorr et al., Reference Knorr, Miskowiak, Akhoj, Vinberg, Forman and Kessing2021; Østergaard et al., Reference Østergaard, Bertelsen, Nielsen, Mors and Petrides2013).
Details of the results for all meta-analyses of the prevalence of psychotic symptoms in BD are presented in Table 1.
Lifetime prevalence of psychotic symptoms in BDI (DSM)
A total of 26 studies (n = 3316) reported specific proportions for a history of psychosis in BDI patients, with a pooled lifetime prevalence of psychotic symptoms of 67% (95% CI 61–72) (Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Cao et al., Reference Cao, Deng, Guan, Yang, Lin, Ma and Hu2014; Davila et al., Reference Davila, Zumarraga, Basterreche, Arrue, Zamalloa and Anguiano2006; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Goldberg et al., Reference Goldberg, Garno, Portera, Leon, Kocsis and Whiteside1999; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Jamra et al., Reference Jamra, Schulze, Becker, Brockschmidt, Green, Alblas and Schumacher2010; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Kent et al., Reference Kent, Disner, Van Voorhis, Urosevic, Caligiuri and Sponheim2020; Kirov & Murray, Reference Kirov and Murray1999; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Lee & Kim, Reference Lee and Kim2011; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Ong et al., Reference Ong, Walterfang, Malhi, Styner, Velakoulis and Pantelis2012; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Parker et al., Reference Parker, Graham, Hadzi-Pavlovic, McCraw, Hong and Friend2013; Patterson et al., Reference Patterson, Sandman, Ring, Jin and Bunney2009; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sarrazin et al., Reference Sarrazin, Cachia, Hozer, McDonald, Emsell, Cannon and Houenou2018; Tost et al., Reference Tost, Ruf, Schmal, Schulze, Knorr, Vollmert and Rietschel2010; Trotti et al., Reference Trotti, Parker, Sabatinelli, Tamminga, Gershon, Keedy and Clementz2020; Yilmaz et al., Reference Yilmaz, Yavuz, Altinbas, Lordoglu and Kurt2015).
For the 20 studies (n = 2926) of at least moderate quality, the pooled prevalence was 63% (95% CI 57.5–68) (see Fig. 2).
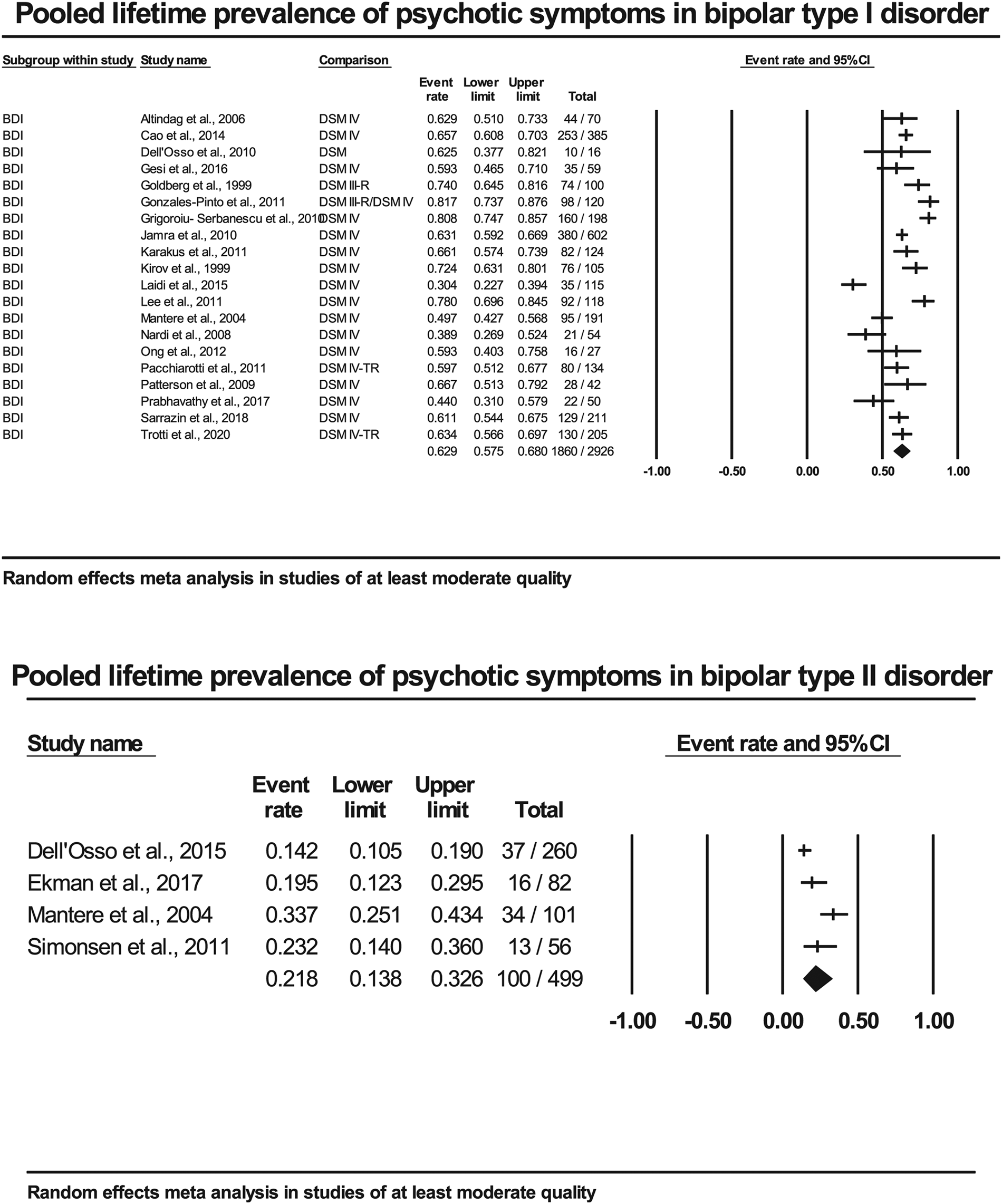
Fig. 2. Forest plots of included studies of at least moderate quality in bipolar type I and type II disorder.
For the 21 studies (n = 2804) using structured diagnostic instruments, the pooled prevalence was 62% (95% CI 57–67.5) (Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Cao et al., Reference Cao, Deng, Guan, Yang, Lin, Ma and Hu2014; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Jamra et al., Reference Jamra, Schulze, Becker, Brockschmidt, Green, Alblas and Schumacher2010; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Kent et al., Reference Kent, Disner, Van Voorhis, Urosevic, Caligiuri and Sponheim2020; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Lee & Kim, Reference Lee and Kim2011; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Ong et al., Reference Ong, Walterfang, Malhi, Styner, Velakoulis and Pantelis2012; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Patterson et al., Reference Patterson, Sandman, Ring, Jin and Bunney2009; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Sarrazin et al., Reference Sarrazin, Cachia, Hozer, McDonald, Emsell, Cannon and Houenou2018; Tost et al., Reference Tost, Ruf, Schmal, Schulze, Knorr, Vollmert and Rietschel2010; Trotti et al., Reference Trotti, Parker, Sabatinelli, Tamminga, Gershon, Keedy and Clementz2020).
For the 10 studies (n = 745) that stated their included age span, the pooled prevalence was 55% (95% CI 45–64) (Altindag et al., Reference Altindag, Yanik and Nebioglu2006; Davila et al., Reference Davila, Zumarraga, Basterreche, Arrue, Zamalloa and Anguiano2006; Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010; Gesi et al., Reference Gesi, Carmassi, Miniati, Benvenuti, Massimetti and Dell'Osso2016; Javadapour et al., Reference Javadapour, Malhi, Ivanovski, Chen, Wen and Sachdev2010; Karakus & Tamam, Reference Karakus and Tamam2011; Laidi et al., Reference Laidi, d'Albis, Wessa, Linke, Phillips, Delavest and Houenou2015; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017). Forest plots for sub analyses can be found online in Supplementary Material 6.
The pooled lifetime prevalence for the seven studies (n = 684) reporting data specifically for inpatient BDI was 71% (95% CI 61–79) (Davila et al., Reference Davila, Zumarraga, Basterreche, Arrue, Zamalloa and Anguiano2006; Goldberg et al., Reference Goldberg, Garno, Portera, Leon, Kocsis and Whiteside1999; Grigoroiu-Serbanescu et al., Reference Grigoroiu-Serbanescu, Herms, Diaconu, Jamra, Meier, Bleotu and Muhleisen2010; Lee & Kim, Reference Lee and Kim2011; Pacchiarotti et al., Reference Pacchiarotti, Mazzarini, Kotzalidis, Valenti, Nivoli, Sani and Colom2011; Prabhavathy et al., Reference Prabhavathy, Kuruvilla, Ravindren, Ganesh and Midhun2017; Tost et al., Reference Tost, Ruf, Schmal, Schulze, Knorr, Vollmert and Rietschel2010).
The pooled lifetime prevalence for the five studies (n = 481) reporting data for BDI treated in outpatient settings was 73.5% (95% CI 51–88) (Dell'Osso et al., Reference Dell'Osso, Bianchi, Del Debbio, Roncaglia, Veltri, Carlini and Piccini2010; Gonzalez-Pinto et al., Reference Gonzalez-Pinto, Barbeito, Alonso, Alberich, Haidar, Vieta and Lopez2011; Karakus & Tamam, Reference Karakus and Tamam2011; Nardi et al., Reference Nardi, Nascimento, Freire, Veras, de-Melo-Neto, Valenca and Versiani2008; Yilmaz et al., Reference Yilmaz, Yavuz, Altinbas, Lordoglu and Kurt2015).
There were no community sample-based studies that met our inclusion criteria.
For more details, see Table 1.
Lifetime prevalence of psychotic symptoms in BDII (DSM)
The pooled lifetime prevalence of psychotic symptoms in the seven studies (n = 704) with data on BDII was 19% (95% CI 13–29) (Atagun et al., Reference Atagun, Sikoglu, Can, Ugurlu, Kaymak, Caykoylu and Ongur2018; Dell'Osso et al., Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Moon et al., Reference Moon, Chang, Kim, Seo, Cha, Ha and Ha2012; Savitz et al., Reference Savitz, Dantzer, Wurfel, Victor, Ford, Bodurka and Drevets2015; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011).
When limiting the studies to those four studies of at least moderate quality (n = 499), the pooled lifetime prevalence for psychotic symptoms was 22% (95% CI 14–33). For more details, see Fig. 2.
The five studies (n = 470) using structured diagnostic instruments had a pooled prevalence of 23% (95% CI 14–35) (Atagun et al., Reference Atagun, Sikoglu, Can, Ugurlu, Kaymak, Caykoylu and Ongur2018; Dell'Osso et al., Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Savitz et al., Reference Savitz, Dantzer, Wurfel, Victor, Ford, Bodurka and Drevets2015; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011). Forest plots for sub analyses can be found online in Supplementary Material 6.
There were only two studies with clear information about the age span for the included patients (Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011), which is too few to meta-analyse.
There were no studies specifically of BDII in inpatient settings, while the pooled lifetime prevalence of psychotic symptoms specifically in outpatient BDII samples based on three studies (n = 494) was 13% (95% CI 8–20) (Dell'Osso et al., Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Moon et al., Reference Moon, Chang, Kim, Seo, Cha, Ha and Ha2012).
Heterogeneity was high throughout most analyses, with lower values for more selected groups, such as BDI and BDII, as expected. For more details, see Table 1.
Point prevalence of psychotic symptoms in BD
The characteristics of the studies of point prevalence are shown in the online Supplementary Material 5. Among these 24 studies, 12 were conducted in Europe, including Turkey, 10 in the Americas, 1 in Africa and 1 including participants from multiple countries. The studies' quality assessment scores ranged from 2 to 5. Of these, 9 (37.5%) studies had low quality and 15 (62.5%) had moderate quality.
The pooled point prevalence for psychotic symptoms in the 20 studies using DSM BD diagnoses (n = 4856) was 41.5% (95% CI 32–52) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Asaad et al., Reference Asaad, Okasha, Ramy, Fekry, Zaki, Azzam and Ahmed2014; Azorin et al., Reference Azorin, Akiskal and Hantouche2006, Reference Azorin, Adida and Belzeaux2015; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Benazzi, Reference Benazzi2001; Bonnin et al., Reference Bonnin, Reinares, Hidalgo-Mazzei, Undurraga, Mur, Saez and Vieta2015; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017; Carroll et al., Reference Carroll, Vohs, O'Donnell, Shekhar and Hetrick2007; Ciapparelli et al., Reference Ciapparelli, Dell'Osso, Tundo, Pini, Chiavacci, Di Sacco and Cassano2001; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Levy & Weiss, Reference Levy and Weiss2010; Lindenmayer et al., Reference Lindenmayer, Bossie, Kujawa, Zhu and Canuso2008; Lundin et al., Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Novis et al., Reference Novis, Cirillo, Da Silva, Santos, Silveira, Cardoso and Cheniaux2014; Reddy et al., Reference Reddy, Meyer, Wittlin, Miller and Weinstock2017; Salem et al., Reference Salem, Ruiz, Hernandez, Wahid, Cao, Karnes and Pigott2019; Samalin et al., Reference Samalin, Llorca, Giordana, Milhiet, Yon, El-Hage and Bellivier2014; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
Out of these 20 studies, in the 12 studies (N = 3359) of at least moderate quality, the pooled point prevalence was 38% (95% CI 27–50) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Asaad et al., Reference Asaad, Okasha, Ramy, Fekry, Zaki, Azzam and Ahmed2014; Azorin et al., Reference Azorin, Akiskal and Hantouche2006, Reference Azorin, Adida and Belzeaux2015; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Benazzi, Reference Benazzi2001; Bonnin et al., Reference Bonnin, Reinares, Hidalgo-Mazzei, Undurraga, Mur, Saez and Vieta2015; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Lundin et al., Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Novis et al., Reference Novis, Cirillo, Da Silva, Santos, Silveira, Cardoso and Cheniaux2014; Samalin et al., Reference Samalin, Llorca, Giordana, Milhiet, Yon, El-Hage and Bellivier2014).
For the 12 studies (n = 2702) using structured assessment, the pooled point prevalence was 37% (95% CI 25–50) (Asaad et al., Reference Asaad, Okasha, Ramy, Fekry, Zaki, Azzam and Ahmed2014; Azorin et al., Reference Azorin, Akiskal and Hantouche2006, Reference Azorin, Adida and Belzeaux2015; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Benazzi, Reference Benazzi2001; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017; Carroll et al., Reference Carroll, Vohs, O'Donnell, Shekhar and Hetrick2007; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Levy & Weiss, Reference Levy and Weiss2010; Lundin et al., Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
For the 11 studies (n = 1263) that gave information about the age span for the included patients, the pooled point prevalence was 45% (95% CI 32–59) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Asaad et al., Reference Asaad, Okasha, Ramy, Fekry, Zaki, Azzam and Ahmed2014; Azorin et al., Reference Azorin, Akiskal and Hantouche2006; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Levy & Weiss, Reference Levy and Weiss2010; Lundin et al., Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Novis et al., Reference Novis, Cirillo, Da Silva, Santos, Silveira, Cardoso and Cheniaux2014; Salem et al., Reference Salem, Ruiz, Hernandez, Wahid, Cao, Karnes and Pigott2019; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
There were not enough studies to meta analyse the point prevalence for ICD-based studies (Kessing, Reference Kessing2004; Kessing et al., Reference Kessing, Jensen and Christensen2008) or studies using research diagnostic criteria (Fiedorowicz et al., Reference Fiedorowicz, Endicott, Leon, Solomon, Keller and Coryell2011; Goldberg & Harrow, Reference Goldberg and Harrow2004). For more details, see Table 1.
Point prevalence of psychotic symptoms in BD according to treatment setting (DSM)
A total of nine studies (n = 2947) reporting on inpatient samples found a pooled point prevalence of 54% (95% CI 39–68) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Azorin et al., Reference Azorin, Akiskal and Hantouche2006, Reference Azorin, Adida and Belzeaux2015; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Levy & Weiss, Reference Levy and Weiss2010; Lindenmayer et al., Reference Lindenmayer, Bossie, Kujawa, Zhu and Canuso2008; Reddy et al., Reference Reddy, Meyer, Wittlin, Miller and Weinstock2017; Salem et al., Reference Salem, Ruiz, Hernandez, Wahid, Cao, Karnes and Pigott2019; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
The five studies (n = 1178) based on outpatient samples had a pooled point prevalence of 20% (95% CI 11–33) (Benazzi, Reference Benazzi2001; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017; Novis et al., Reference Novis, Cirillo, Da Silva, Santos, Silveira, Cardoso and Cheniaux2014; Samalin et al., Reference Samalin, Llorca, Giordana, Milhiet, Yon, El-Hage and Bellivier2014; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007).
Three studies (n = 780) reported data for current depressive episodes across both BDI/BDII samples, here with a pooled point prevalence of psychotic symptoms of 13% (95% CI 7–23.5) (Azorin et al., Reference Azorin, Adida and Belzeaux2015; Benazzi, Reference Benazzi2001; Caldieraro et al., Reference Caldieraro, Sylvia, Dufour, Walsh, Janos, Rabideau and Nierenberg2017). There were no studies of current psychotic symptoms in BD community samples.
For more details, see Table 1.
Point prevalence of psychotic symptoms in BDI (DSM)
The 14 studies (n = 3099) reporting data on BDI samples gave a pooled point prevalence of psychotic symptoms of 51% (95% CI 40–61) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Azorin et al., Reference Azorin, Akiskal and Hantouche2006; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Bonnin et al., Reference Bonnin, Reinares, Hidalgo-Mazzei, Undurraga, Mur, Saez and Vieta2015; Carroll et al., Reference Carroll, Vohs, O'Donnell, Shekhar and Hetrick2007; Ciapparelli et al., Reference Ciapparelli, Dell'Osso, Tundo, Pini, Chiavacci, Di Sacco and Cassano2001; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Levy & Weiss, Reference Levy and Weiss2010; Lindenmayer et al., Reference Lindenmayer, Bossie, Kujawa, Zhu and Canuso2008; Lundin et al., Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Reddy et al., Reference Reddy, Meyer, Wittlin, Miller and Weinstock2017; Salem et al., Reference Salem, Ruiz, Hernandez, Wahid, Cao, Karnes and Pigott2019; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
In the six BDI studies (n = 1602) of at least moderate quality, the pooled point prevalence was 54% (95% CI 41.5–67) (see Fig. 3).
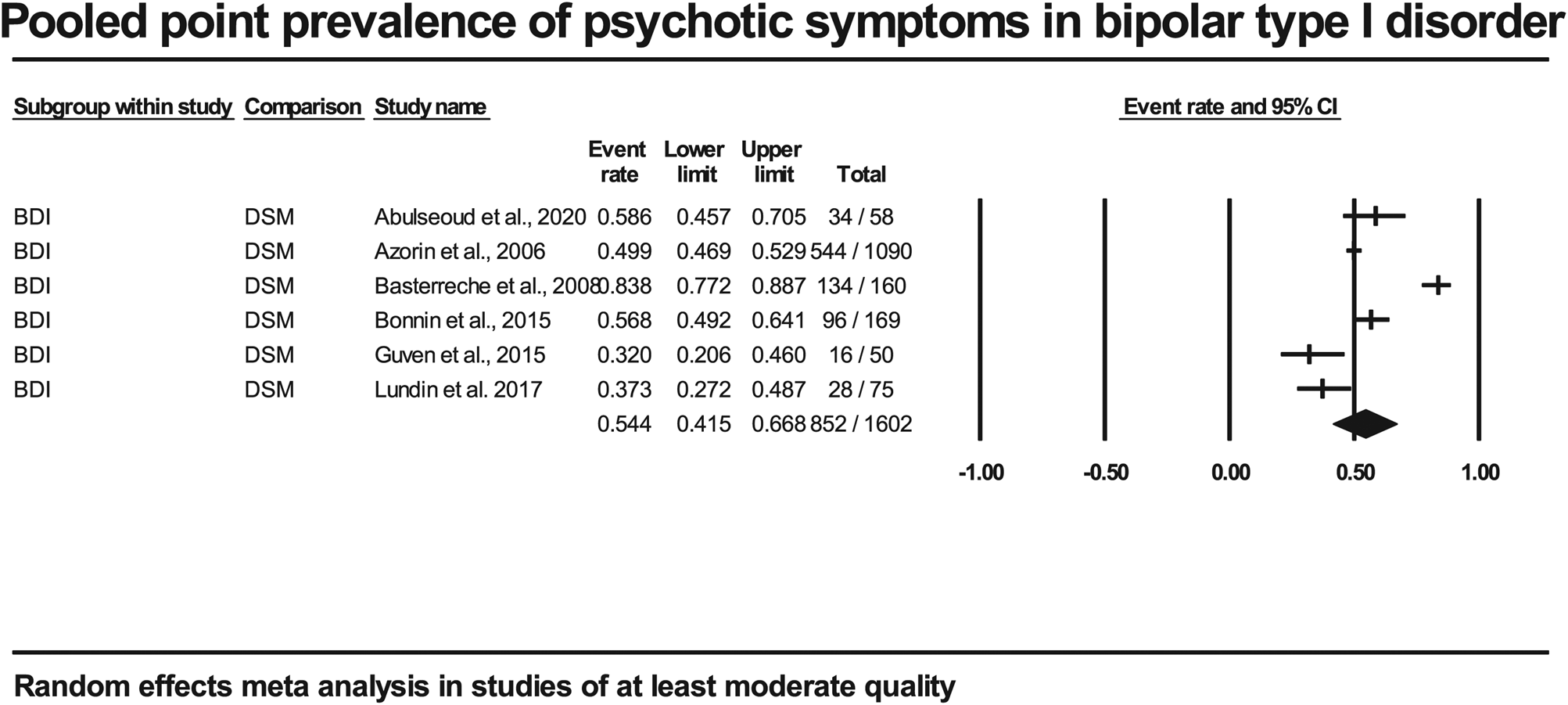
Fig. 3. Forest plot of included studies of at least moderate quality in point prevalence of psychotic symptoms in bipolar type I disorder.
In the eight BDI studies using structured assessment, there was a pooled point prevalence of 48% (95% CI 35–61) (n = 1572) (Azorin et al., Reference Azorin, Akiskal and Hantouche2006; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Carroll et al., Reference Carroll, Vohs, O'Donnell, Shekhar and Hetrick2007; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Levy & Weiss, Reference Levy and Weiss2010; Lundin et al., Reference Lundin, Bartolomeo, O'Donnell and Hetrick2018; Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
The pooled point prevalence in the eight studies (n = 2669) of psychotic symptoms in BDI inpatients was 58% (95% CI 43–72) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Azorin et al., Reference Azorin, Akiskal and Hantouche2006; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Levy & Weiss, Reference Levy and Weiss2010; Lindenmayer et al., Reference Lindenmayer, Bossie, Kujawa, Zhu and Canuso2008; Reddy et al., Reference Reddy, Meyer, Wittlin, Miller and Weinstock2017; Salem et al., Reference Salem, Ruiz, Hernandez, Wahid, Cao, Karnes and Pigott2019; Yildiz et al., Reference Yildiz, Guleryuz, Ankerst, Ongur and Renshaw2008).
There was only one study (n = 49, low quality) reporting data for outpatient BDI, here finding a prevalence of 26.5% (Schwartzmann et al., Reference Schwartzmann, Amaral, Issler, Caetano, Tamada, De Almeida and Lafer2007).
The pooled point prevalence for the six studies (n = 2062) that reported psychotic symptoms during current manic episodes was 57% (96% CI 47–66) (Abulseoud et al., Reference Abulseoud, Senormanci, Senormanci, Guclu, Schleyer and Camsari2020; Azorin et al., Reference Azorin, Adida and Belzeaux2015; Basterreche et al., Reference Basterreche, Davila, Zumarraga, Arrue, Gonzalez-Torres, Zamalloa and Guimon2008; Bonnin et al., Reference Bonnin, Reinares, Hidalgo-Mazzei, Undurraga, Mur, Saez and Vieta2015; Guven et al., Reference Guven, Kesebir, Demirer and Bilici2015; Lindenmayer et al., Reference Lindenmayer, Bossie, Kujawa, Zhu and Canuso2008).
No studies reported psychotic symptoms during depressive episodes in BDI. There were not enough studies to estimate the point prevalence of psychotic symptoms in BDI depression or in mixed episodes. For more details, see Table 1.
Point prevalence of psychotic symptoms in BDII
We found only one study (n = 199, moderate quality) reporting the proportion of current psychotic symptoms in BDII at 8.5% (Benazzi, Reference Benazzi2001).
Heterogeneity was high throughout all analyses. For more details, see Table 1.
Potential publication bias
A funnel plot of the 52 studies assessing the lifetime prevalence of psychotic symptoms in DSM-based BD visually appears symmetrical but with a small difference between the observed and imputed scores, see Supplementary Material 7: Funnel plots of studies included in the estimation of lifetime and point prevalence of psychotic symptoms in bipolar disorders. Egger's regression test for funnel plot asymmetry was significant (t = 1.96; df = 50; p = 0.05). This suggests that the possibility of publication bias cannot be ruled out. To handle possible publication bias issues, we performed repeated analyses to investigate whether the results changed when the lower-quality studies were removed. The funnel plot of the 39 DSM-based lifetime studies of at least moderate quality visually appears symmetrical, with marginal difference between the observed and imputed scores. The Egger's test for these 39 studies was no longer significant (t = 1.28; df = 38; p = 0.21) (see Supplementary Material 7). Based on this, we decided to report estimates based on studies of at least moderate quality as our main results.
A funnel plot of the 20 DSM studies assessing the point prevalence of psychotic symptoms in BD visually appears symmetrical, with no difference between the observed and imputed scores (see Supplementary Material 7). Egger's regression test for funnel plot asymmetry was non-significant (t = 0.78; df = 18; p = 0.44), suggesting a lack of evidence for publication bias.
Discussion
Main findings and implications
The present meta-analysis extends the literature about the prevalence of psychotic symptoms in BD by examining both the lifetime and point prevalence of psychotic symptoms across diagnostic subgroups, current clinical status and study settings.
The main finding of the current study is that psychotic symptoms seem to be more common in BD than previously assumed. For BDI, the pooled lifetime prevalence was 63%, and in inpatients alone, it was 71%. The diagnostic systems Diagnostic and Statistical Manual of Mental Disorders (DSM; versions IV and 5) and International Classification of Diseases and Related Health Problems, 10th version (ICD-10) have different criteria regarding the type of psychotic symptoms that are allowed to co-occur with mood episodes in a diagnosis of BD. In ICD-10, any first-rank symptoms during mood episodes would imply a schizophrenia spectrum diagnosis, including (1) delusions of control, influence or passivity, clearly referred to body or limb movements or specific thoughts, actions or sensations; or delusional perceptions; (2) hallucinatory voices giving a running commentary on the patient's behaviour or discussing him/her between themselves or other types of hallucinatory voices coming from some part of the body and/or (3) persistent delusions of other kinds that are culturally inappropriate and completely impossible (e.g. being able to control the weather, or being in communication with aliens from another world) (World Health Organization, 1992). It appears that this specification will not be part of ICD-11 (World Health Organization, 2020) so that first-rank symptoms during mood episodes will no longer exclude a BD diagnosis. In contrast, both DSM-IV and DSM-5 allow for a diagnosis of BD if the first-rank symptoms only occur during mood episodes, here with the exception of hypomania. These exclusion criteria of first-rank symptoms because an ICD-10 BD diagnosis could theoretically lead to a lower prevalence of psychotic symptoms in ICD-10 BD-samples (1992) compared with ICD-11, DSM-IV or DSM-5 (American Psychiatric Association, 2013). The previous estimates were 60% in inpatient BDI (Goodwin & Jamison, Reference Goodwin and Jamison2007).
For the first time, this meta-analysis presents estimates of the pooled lifetime prevalence of psychotic symptoms in BDII. Because the diagnostic criteria do not allow for the presence of psychotic symptoms in hypomanic phases, reports of psychotic symptoms in BDII will necessarily occur in depressive episodes. We were able to identify only seven relatively small studies, indicating a lifetime prevalence of psychotic symptoms in BDII varying between 13% and 29%, depending on the type of treatment setting and study quality (Atagun et al., Reference Atagun, Sikoglu, Can, Ugurlu, Kaymak, Caykoylu and Ongur2018; Dell'Osso et al., Reference Dell'Osso, Holtzman, Goffin, Portillo, Hooshmand, Miller and Ketter2015; Ekman et al., Reference Ekman, Petrovic, Johansson, Sellgren, Ingvar and Landen2017; Mantere et al., Reference Mantere, Suominen, Leppamaki, Valtonen, Arvilommi and Isometsa2004; Moon et al., Reference Moon, Chang, Kim, Seo, Cha, Ha and Ha2012; Savitz et al., Reference Savitz, Dantzer, Wurfel, Victor, Ford, Bodurka and Drevets2015; Simonsen et al., Reference Simonsen, Sundet, Vaskinn, Birkenaes, Engh, Faerden and Andreassen2011). This estimate may be somewhat low when considering that one previous systematic review and meta-analysis on the prevalence of psychotic symptoms in major depressive disorder estimated lifetime prevalence rates of 28% in overall patient samples and 42% in inpatient samples (Jääskeläinen et al., Reference Jääskeläinen, Juola, Korpela, Lehtiniemi, Nietola, Korkeila and Miettunen2018); in addition, psychotic symptoms are believed to be more common in bipolar depression than unipolar depression (Souery et al., Reference Souery, Zaninotto, Calati, Linotte, Sentissi, Amital and Serretti2011).
The current study also demonstrates a high point prevalence of psychotic symptoms in BD: more than half (54%) of BD inpatients experience current psychotic symptoms, irrespective of the polarity of the episode. As expected, the point prevalence of psychotic symptoms in outpatients is lower than in inpatients. This is in line with the notion that psychotic symptoms are markers of a more severe episode and lower severity of patients in outpatient than inpatient settings (Azorin et al., Reference Azorin, Akiskal, Akiskal, Hantouche, Châtenet-Duchêne, Gury and Lancrenon2007). However, there is also a possibility that psychotic symptoms are independent of the severity of the affective symptoms and may by themselves contributing to a more severe episode and the need for hospitalisation (Dubovsky, Ghosh, Serotte, & Cranwell, Reference Dubovsky, Ghosh, Serotte and Cranwell2021). In addition, indications that about one in five outpatients with BD experience current psychotic symptoms suggest that clinicians working in outpatient settings should pay attention to possible psychotic symptoms, in addition to mood swings.
Another main finding is limited knowledge about psychotic symptoms in depressive episodes in BD. This was the case in both BDI and BDII and in- and outpatients. This is of clinical importance, given the potentially increased suicide risk in psychotic depression and psychotic mixed episodes (Dell'Osso et al., Reference Dell'Osso, Pini, Tundo, Sarno, Musetti and Cassano2000). More specifically, there seems to be a potential association between, for example, delusions of guilt and suicidality (Fredriksen et al., Reference Fredriksen, Schoeyen, Johannessen, Walby, Davidson and Schaufel2017; Kuperberg et al., Reference Kuperberg, Katz, Greenebaum, George, Sylvia, Kinrys and Nierenberg2021), and the potential lack of systematic investigation of such symptoms may be a problem.
We did not meet our aim of reporting the prevalence rates in community samples, either for the lifetime or point prevalence, because of a lack of studies. We found one study, which was excluded from the meta-analysis because of the advanced age of the participants. This study reported a lifetime prevalence of 11% for psychotic symptoms and point prevalence of 4% in previously undiagnosed individuals in the community meeting BD diagnostic criteria (Tuulio-Henriksson et al., Reference Tuulio-Henriksson, Perala, Saarni, Isometsa, Koskinen, Lonnqvist and Suvisaari2011).
The ICD-10-based studies are few in number and indicate considerably lower prevalence rates than DSM-based studies. There are several possible reasons for this. First most of the ICD-based studies used the standard discharge diagnosis retrieved from medical records provided by real-world clinical assessments and routine clinical reports, which may be biased by the focus of clinicians on mood disorders. If psychotic symptoms were not systematically addressed, this could lead to psychotic symptoms being under-reported. Another possible reason is that studies using ICD-10 diagnoses do not allow for first-rank psychotic symptoms in BD (including mainly 1) delusions of control, influence or passivity; 2) running commentary hallucinatory voices; and/or 3) other persistent culturally inappropriate or impossible delusions of other kinds (World Health Organization, 1992), yielding diagnoses other than BD in such cases. Because of the lack of high-quality research using standardised diagnostic instruments within the ICD framework, we do not know how common psychotic symptoms are in ICD-10-defined BD.The fact that these first-rank symptoms were allowed as per DSM-IV and 5 (American Psychiatric Association, 2013) could partly explain the discprepancies observed. Future studies based on ICD-11 (World Health Organization, 2020) for which it appears first-rank symptoms no longer exclude BD will provide further clarity.
The clinical implications of the current study indicate that clinicians treating BD should also have knowledge on how to assess and treat psychotic symptoms. Training all clinicians in outpatient services to detect and treat psychotic symptoms is resource demanding, which could be an argument for treating BD patients in specialised BD outpatient units. Indeed, such specialised units appear to reduce the need for hospitalisations, the costs related to treatment and patient satisfaction (Henry et al., Reference Henry, Godin, Courtet, Azorin, Gard, Bellivier and Etain2017; Kessing et al., Reference Kessing, Hansen, Hvenegaard, Christensen, Dam, Gluud and Wetterslev2013). Alternatively, BD patients with psychotic symptoms could be treated in units specialised in the treatment of psychotic disorders. Another possibility is to develop shared units for BD and psychotic disorders, in particular in more rural areas.
Strengths and limitations
Strengths
The present systematic review and meta-analysis on both lifetime and point prevalence of psychotic symptoms in different subtypes of BD across types of settings has addressed a gap in the literature.
Limitations
There is considerable heterogeneity in our analyses, which calls for caution in interpreting the results. BD is a highly heterogeneous disorder with large variations in symptom presentation, level of functioning and help-seeking behaviour. Because of this natural heterogeneity, it is difficult to disentangle what is a potential cause of publication bias and what is because of the natural heterogeneity of the BD population. Furthermore, most studies have reported on combined samples with BDI and BDII, without reports for diagnostic subgroups. Heterogeneity was handled using random effect models. In general, the quality of the studies reporting point prevalence was lower than for those reporting lifetime prevalence. A considerable percentage (37.5%) of the point prevalence studies were of low quality, which caution interpretability of the results. This was solved by conducting sensitivity analyses, and by reporting results based on moderate quality.
We did not include paediatric or geriatric samples, which could be of interest for further studies. Another weakness is the language restriction, so studies in languages other than English are missing (we did not include any studies in one of the Scandinavian language). We did not find any studies reporting on certain lifetime (community samples, inpatient BDII) and point prevalence subgroups (current depressive episodes in BDI, current mixed episodes, outpatient BDI and BDII in general).
Conclusion
The results from our systematic review and meta-analysis of the lifetime prevalence of psychotic symptoms in BD indicates that in BDI patient populations close to 3/4 had psychotic symptoms during their lifetime. In studies of at least moderate quality, the pooled lifetime prevalence in BDI in general was 63% and 22% in BDII. As for point prevalence, more than half of BD inpatients and BDI patients were found to be experiencing psychotic symptoms in a given episode; this number was roughly one in five in an outpatient setting. Taken together, this suggests that psychotic symptoms could be more common in BD than previously reported. However, there are not enough studies of important settings, such as community samples, and for bipolar depression in general. This lack of studies should be systematically addressed in future studies because psychotic symptoms in BD are a major risk factor for poor outcome and suicidality.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S003329172200201X
Acknowledgements
We thank the funders and co-workers for their invaluable contributions and discussions, especially Hugo Are Pripp, Margrethe Collier Høegh, Adriano Winterton and Elizabeth Ann Barrett.
Financial support
This study was supported by the Research Council of Norway (223273) and KG Jebsen Stiftelsen.
Conflict of interest
OAA has received a speaker's honorarium from Lundbeck and is a consultant for HealthLytix. The other authors have no conflicts of interest or financial disclosures to declare. The funders played no role in the study design, collection, analysis, interpretation of data, writing of the report or decision to submit the paper for publication, and they accept no responsibility for the contents.







 Open access
Open access