



Disasters are events that disrupt the normal functioning capacity of society and result in numerous economic and physical losses that are difficult to cope with using local resources. Reference Born, Briggs and Ciraulo1 The recent disaster events have increased global awareness about the need to be prepared for disasters. However, no matter how well-prepared a country may be, it is still possible for large-scale disasters to necessitate disaster medical assistance and humanitarian aid. In the case of natural or technological disasters, there can be an immediate need for significant destruction and urgent intervention requirements. This, in turn, will require the prompt mobilization of national and international resources. Reference Russbach2
The response phase of a disaster, especially a sudden-onset one, includes saving lives, treating the injured or ill, meeting basic humanitarian needs, and addressing the immediate needs of the affected community. Reference Hay and Pascoe3 During the intervention phase, the first priority is the evacuation and rescue of individuals stranded in hazardous areas. It is essential for injured or ill individuals to receive medical assistance, which can include basic first aid measures or, in the case of severe injuries, the transfer to medical facilities. Both scenarios are typically carried out by local or national rescue teams. Medical rescue teams are specialized teams tasked with providing medical assistance in disaster areas and coordinating emergency medical services. These teams take on responsibilities such as addressing patients’ medical needs, implementing urgent medical procedures, and directing medical resources. Reference McEntire4
Globally, a wide range of tools and intervention mechanisms are used to save lives and alleviate the pain caused by natural disasters. Reference Dara, Ashton and Farmer5 Regardless of which country a disaster occurs in, it will exceed local capacity, so National Disaster Medical Systems have been established in many countries and Disaster Medical Teams have been formed under this scope. Various medical rescue teams, both national and local, are involved in many countries. Examples of medical rescue teams include DMAT (Disaster Medical Assistance Teams) and TCCT (Trauma and Critical Care Teams) in the United States, IMSURT (International Medical Surgical Response Teams); DART (Disaster Assistance Response Team) in Canada, J-DMAT (Japan-Disaster Medical Assistance Teams) in Japan, AUS-MAT (Australian Medical Assistance Teams) in Australia, and NMRT (National Medical Rescue Teams) in Turkey. Reference Shahrestanaki, Khankeh and Masoumi6,Reference Zafeirakis and Efstathiou7
In overcoming the chaotic environments caused by disasters, medical rescue teams play a vital role. However, these rescue teams face various challenges in the process of reaching disaster areas, coordinating medical interventions, and providing assistance to victims. Especially during the response phase, there may be deficiencies in search and rescue operations and medical services. These problems can result in an increase in functional damage and a decrease in buffering capacity during the response phase of a disaster. Additionally, response teams may experience significant stress and suffer from physical and mental health problems as a result of the challenges encountered during disaster situations. Failure to identify and address these issues can even lead to personnel loss. Reference Ghodsi, Sohrabizadeh and Khani Jazani8
Identifying the problems faced by medical rescue teams can be a highly effective and important method in determining ways to increase their intervention levels. Conducting a literature review is the first step in achieving this goal. In the literature, various studies have been conducted focusing on lessons learned from disasters and challenges faced in disasters. However, it has been observed that these studies mainly address management issues and do not provide a comprehensive perspective on the problems. Therefore, in this study, distinct from previous research, the challenges encountered by medical rescue teams in disaster response have been thoroughly analyzed with a specific focus and a systematic review approach, aiming to provide a different perspective to the existing literature in this field. The findings provide information to academics for future disaster research, especially in the response phase, and offer opportunities to develop a roadmap for medical rescue teams.
Methods
In this study, a systematic review of articles related to the challenges faced by medical rescue teams during response in sudden-onset disasters caused by natural, human, or technological factors has been conducted. An integrative review methodology, which is considered the most comprehensive form of research review due to its ability to bring together different perspectives on the subject, was used in this study. Reference Whittemore and Knafl9 The review process includes defining the problem, conducting a literature search, selecting and collecting data, analyzing the quality of evidence, and presenting the data. Although no protocol and record were established regarding the inclusion criteria and analysis methods of this study, this study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Reference Moher, Liberati and Tetzlaff10
Definitional Concepts
To ensure conformity with the established criteria, the PICOS framework was used. The participants of this study consist of medical rescue teams involved in disaster response (Participants). The challenges affecting the response of medical rescue teams were examined (Intervention). A comparative analysis of medical rescue teams’ challenges was carried out (Comparison). Descriptions stated by different authors also constitute outcomes (Outcomes). In this research, all studies published in English were included (Study designs).
Databases and Search Strategy
Database searching was conducted with the combination of the following keywords: (disaster* OR catastrophe*) AND (medical rescue* OR assistance* OR first responder* OR worker*) AND (team*) AND (response* OR intervention*) AND (problem* OR obstacle* OR challenge*). For the selection of key terms, experts in the disaster management field were consulted and the consensus of 4 researchers was taken into consideration. An extensive search was performed for relevant articles. Articles published on PubMed, Scopus, Web of Science, and Cochrane until January 2023 were received. The references of the publications obtained within the scope of the research related to the research question were accessed through the Google scholar database.
Eligibility Criteria
Inclusion Criteria
(1) Articles focusing on at least 1 challenge faced by medical rescue teams during the response phase of sudden-onset disasters caused by natural, human, or technological factors; (2) Articles that are accessible and free of charge; and (3) Articles written in English.
Exclusion Criteria
(1) Articles that do not focus on the challenges faced by medical rescue teams during the response phase of sudden-onset disasters but instead focus on slow-onset disasters; (2) Articles not written in English; (3) Articles for which the full text is not available; and (4) Articles with a high risk of bias and that did not meet the inclusion criteria were excluded.
Study Selection and Data Extraction
In the first stage, 2 researchers (A.D.K. and T.Ö.) independently reviewed the articles based on their titles and abstracts to prevent any potential bias. The researchers subsequently engaged in a thorough discussion of the articles and collectively agreed upon the selection and inclusion of studies in the final dataset. EndNote version X20 (Clarivate Analytics, Philadelphia, PA) was used to manage the screened references and eliminate any duplicate entries. In the second stage, the same researchers conducted a full-text analysis of the articles that met the inclusion criteria. In the event of any disagreement between the 2 authors, they read and discussed the articles in detail, and endeavored to reach a consensus. In the cases where they could not reach a consensus, the other researchers (C.C. and K.K.) were the final decision-makers regarding the inclusion of the article. In the last stage, data from the reviewed studies were extracted with a form created by the authors. The following information was recorded from the selected studies to describe the findings: (1) author/year; (2) title; (3) study aims; (4) methods; (5) main findings; (6) suggestions. All extracted data were reviewed by members of the research team to confirm accuracy and completeness.
Quality Appraisal
In this study, The Mixed Methods Appraisal Tool (MMAT) 2018 version was used to evaluate the quality of the included articles. The MMAT is a comprehensive assessment tool that enables the evaluation of various research designs such as quantitative, qualitative, and mixed methods studies. It consists of 5 categories, each with 5 relevant specific criteria, which include a qualitative set, a random set, a non-random set, an observational descriptive set, and a mixed method set. According to the MMAT 2018 version, it is not suggested to score based on category criteria. Instead, the tool requires a description of which criteria have been fulfilled and which have not. Reference Hong, Fàbregues and Bartlett11 During the quality assessment, the 2 researchers (A.D.K. and T.Ö.) analyzed each article according to the MMAT categories for any potential biases. Any discrepancies were resolved through negotiation or consultation with a third author. The results of the quality assessment conducted using MMAT 2018 in this systematic review included articles that met 3 to 5 (out of 5) criteria.
Data Synthesis and Analysis
Due to the heterogeneity of results and the presence of nonindependent samples, the use of statistical techniques was not feasible for analyzing the data. Reference Thomas and Harden12 For this reason, a thematic analysis framework was used to synthesize the findings from the included studies using a deductive approach based on recommendations of Braun and Clarke. Reference Braun and Clarke13 The thematic analysis was performed by the 2 authors in 6 stages: (1) familiarizing of data; (2) generating initial codes; (3) searching for themes; (4) reviewing themes; (5) defining and naming themes; and (6) producing the report.
Results
Descriptive Analysis of Documents
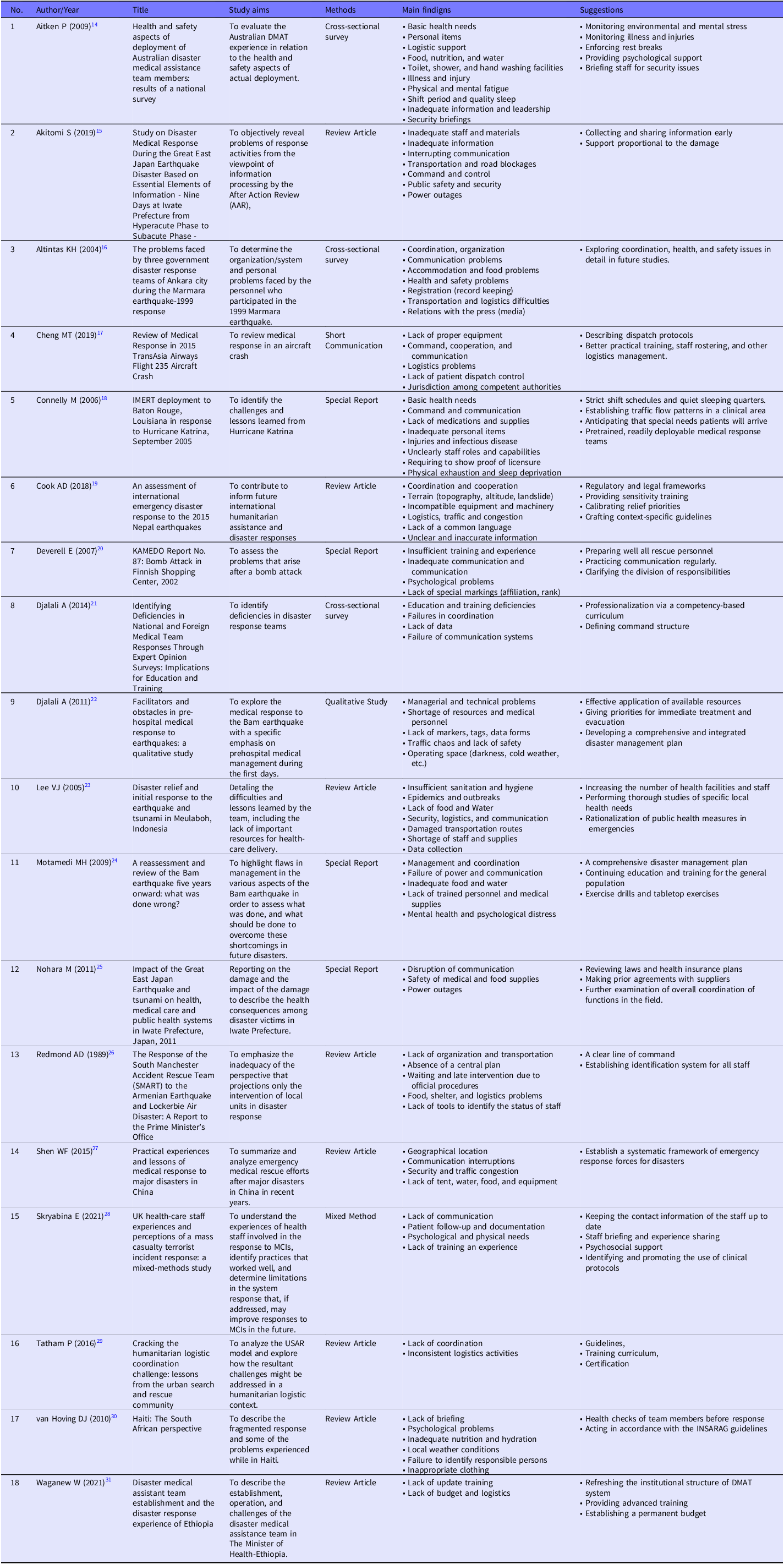
As a result of the search, a total of 353 publications were found 347 from the Web of Science, Scopus, Cochrane, and PubMed databases and 6 from the gray literature. After the duplicated articles were removed, 252 publications remained. A total of 252 articles were screened by reviewing their titles and abstracts and 210 articles were deleted, so 42 articles remained. Because 21 of them did not include any challenges faced by medical rescue teams and the full text of 3 of them could not be accessed, 18 of them were included in the findings of the study (Figure 1). The publication dates of the 18 studies included in the research findings range from 1989 to 2021. Eight of these studies are review articles, 4 are special reports, 3 are cross-sectional studies, 1 is a mixed study, 1 is a qualitative study, and 1 is a short communication (Table 1).
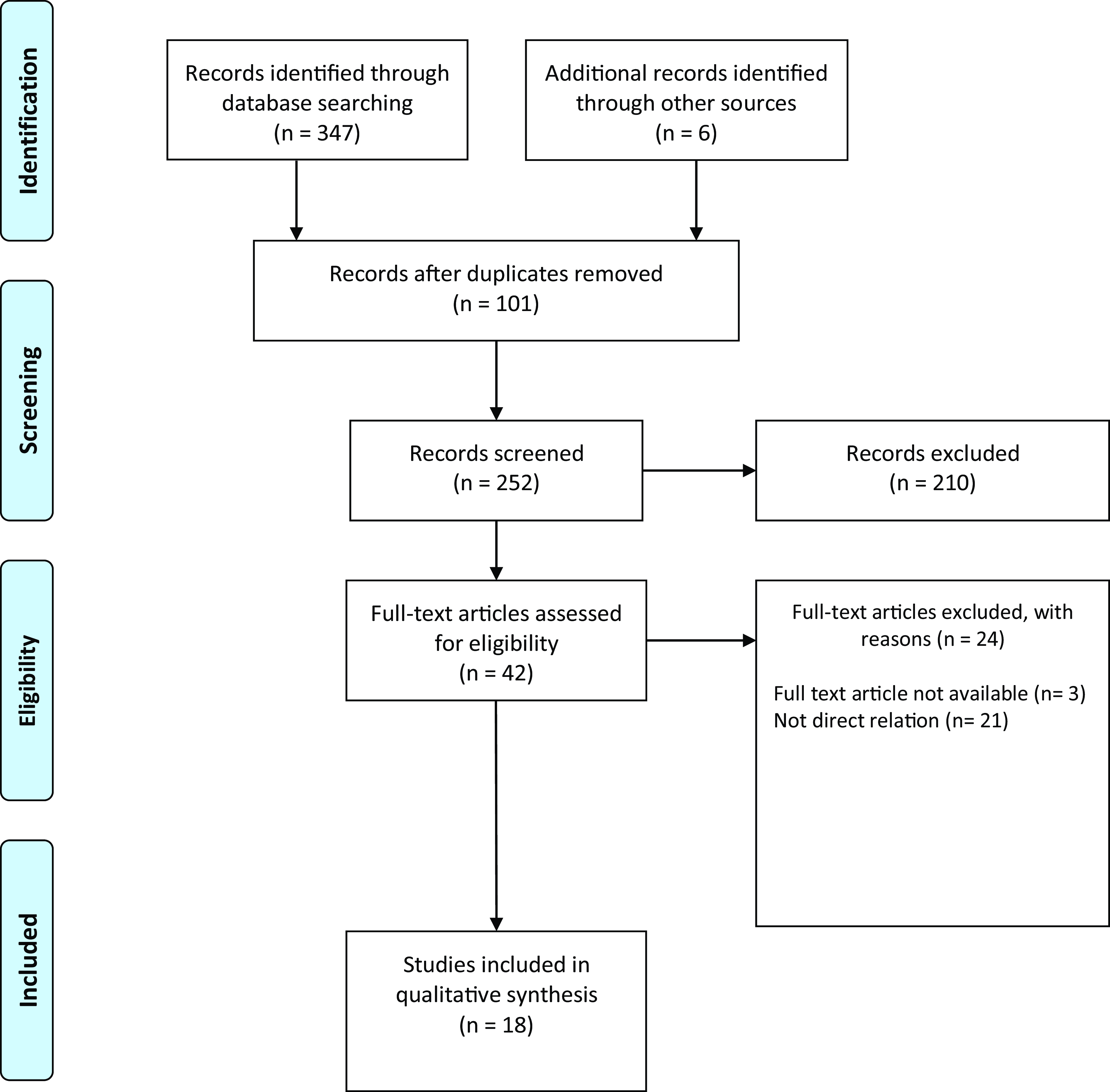
Figure 1. Flow diagram of study identification and selection process.
Table 1. Characteristics of included studies
Thematic Analysis of Documents
In this study, the challenges faced by disaster response teams are summarized under 6 categories: organizational; individual; environmental and health; logistics; information and communication; and other factors (Figure 2).

Figure 2. Categories of challenges faced by medical rescue teams.
Organizational Factors
During the disaster response phase, command structures often lack clarity and stability. Although organizations and governments have the responsibility to create suitable conditions for medical rescue teams to fulfill their duties with minimal difficulty, these teams often encounter organizational challenges when responding to disasters. Reference Aitken, Leggat and Robertson14 Coordination problems have emerged as the most common challenge faced by medical rescue teams in the studies included in this research. Reference Akitomi, Kokogawa and Kosaka15–Reference Tatham and Spens17 The lack of coordination among various organizations involved in disaster response poses significant challenges in terms of the overall effectiveness of medical rescue and is evident at different operational levels, spanning from local to national and international contexts. Reference Djalali, Khankeh and Öhlén18 The absence of a centralized plan and the inflexibility of emergency plans prevent the establishment of a unified organizational structure. Without a unified organizational structure, emergency plans cannot be smoothly executed across various departments and different administrative areas. Reference Redmond19,Reference Shen, Jiang and Zhang20 This situation presents itself as a significant problem among rescue teams and leads to disruptions in the intervention process. Other organizational problems include conflicts of authority between central and local authorities and the absence of clear definitions for the roles and abilities of medical rescue personnel. Reference Cheng, Lin and Chou21,Reference Connelly22 The presence of diverse leadership structures hinders the successful integration of response activities, resulting in failure. Reference Djalali, Ingrassia and Corte23 Last, both a review and a cross-sectional study have reported that inadequate leadership and delays in obtaining permission for the deployment of medical rescue teams significantly diminish the overall effectiveness of interventions. Reference Akitomi, Kokogawa and Kosaka15,Reference Redmond19
Individual Factors
In the analysis of the articles, it has been emphasized that individual challenges faced by medical rescue teams during disaster intervention include not only the hardships related to pain, death, and destruction but also taxing issues such as long working hours and insufficient sleep. Reference Aitken, Leggat and Robertson14 Having education and experience in disaster response is crucial for medical rescue teams to effectively carry out their tasks during emergencies. Reference Djalali, Ingrassia and Corte23,Reference Skryabina, Betts and Reedy24 However, some medical rescue teams lack experience and education due to inadequate training exercises, insufficient experience, and the absence of advanced and refresher training sessions following basic training. Reference Deverell, Ortenwall and Almgren25–Reference Sengezer and Koç27 It is also noteworthy that some medical rescue teams cannot meet their basic needs such as food, water, and shelter in disaster situations. Reference Redmond19,Reference Shen, Jiang and Zhang20,Reference Cook, Shrestha and Htet28,Reference Nohara29 Furthermore, the absence of essential personal belongings, proper clothing, and personal protective equipment (PPE) accompanies these challenges. Some studies have indicated that medical rescue teams lack PPE, including helmets and work gloves, and do not have minimum personal equipment kits. Reference Aitken, Leggat and Robertson14,Reference Van Hoving, Smith and Kramer30 Last, being away from home and lacking sufficient information about their families are considered significant issues during disaster response for medical rescue teams, greatly impacting their morale. Reference Aitken, Leggat and Robertson14,Reference Nocera31
Environmental and Health Factors
Following a disaster, both the affected community and the disaster responders themselves suffer from health effects. The medical rescue teams, in particular, endure prolonged periods of work in the disaster-stricken area and are more susceptible due to close contact with numerous individuals. The challenges that arise, particularly in areas such as water, sanitation, hygiene, and vector control, pose a risk for medical rescue teams in conjunction with the existing limited resources. Reference Aitken, Leggat and Robertson14–Reference Altntaş and Delooz16,Reference Lee, Low and Ng32 Inadequate toilets, washing and bathing facilities, adverse weather conditions such as darkness and cold, and improper waste disposal are other issues affecting the health of medical rescue teams. Reference Connelly22,Reference Van Hoving, Smith and Kramer30,Reference Lee, Low and Ng32 Moreover, medical rescue teams are hindered by the stressful, dusty, and noisy conditions in their rest areas. At this point, the importance of providing psychosocial support for intervention and support personnel has been recognized. Reference Aitken, Leggat and Robertson14,Reference Skryabina, Betts and Reedy24
Logistics Factors
It is reported that there is a shortage of personnel and resources among rescue teams worldwide that respond to various types of disasters. Reference Djalali, Khankeh and Öhlén18,Reference Djalali, Ingrassia and Corte23,Reference Lee, Low and Ng32,Reference Motamedi, Saghafinia and Bafarani33 Especially, the shortage of medical resources during the early phase of a disaster is an important obstacle for medical rescue teams. Reference Djalali, Khankeh and Öhlén18,Reference Djalali, Ingrassia and Corte23 The lack of compatibility among the types of equipment and machinery brought for disaster response, unfamiliarity with the use of the equipment by medical rescue teams, and clothing and equipment that do not align with the field conditions lead to disruptions in intervention activities. Reference Shen, Jiang and Zhang20,Reference Connelly22,Reference Cook, Shrestha and Htet28,Reference Motamedi, Saghafinia and Bafarani33 The arrival and unloading of vehicles filled with aid supplies without any prior notification regarding the nature of the materials, their necessity, and who will collect and distribute them further burdens the already fragile and overwhelmed rescue teams. Reference Tatham and Spens17,Reference Cook, Shrestha and Htet28 Additionally, inadequate capacity for air evacuations and severe damage to airports and highways result in rescue teams transporting patients through nonstandard methods, leading to higher mortality rates. Reference Djalali, Khankeh and Öhlén18,Reference Shen, Jiang and Zhang20,Reference Waganew and Azazh26,Reference Lee, Low and Ng32
Information and Communication Factors
During a disaster, effective information and communication play an important role in providing essential information to the staff and public. Although good communication can help to ensure an effective intervention, poor communication can disrupt or prevent an effective intervention. Reference Skryabina, Betts and Reedy24 During any disaster, there are significant communication challenges among medical rescue teams, and these challenges increase in magnitude with the scale of the disaster. Reference Redmond19 During a disaster, all regular communication channels can be lost and the mobile phone network may become unavailable. Reference Deverell, Ortenwall and Almgren25,Reference Nohara29 Inadequate communication can lead to intervention teams entering dangerous areas, an increase in security risks at the operation site, and consequently, psychological effects such as stress, anxiety, and feelings of exhaustion. Inadequate communication can lead to the rapid spread of misinformation or rumors. This can create panic in the public, further complicate the crisis, and consequently increase the workload of rescue teams. The lack of reliable information and integrated information management systems has also been identified as another significant issue. Reference Djalali, Ingrassia and Corte23,Reference Cook, Shrestha and Htet28 The disruption of information networks and the absence of a system that can collect information as expected lead to further delays in the efforts of rescue teams. Reference Akitomi, Kokogawa and Kosaka15 In addition, the disruption of information networks can also limit access to a patient’s medical history or treatment requirements. When considering the importance of data collection in disaster situations, information management and communication become crucial. In some studies, the emergence and accessibility of digital technologies have introduced a new challenge in the midst of various debated difficulties, which is the remote management of disaster relief operations. Reference Skryabina, Betts and Reedy24,Reference Cook, Shrestha and Htet28
Other Factors
In addition to the mentioned factors above, there are other significant issues, such as a lack of a common language and a shortage of interpreters, which can create difficulties in communicating with patients among medical rescue teams. In disaster situations, along with power, water, and gas outages, a shortage of gasoline can also disrupt the work of these teams. Reference Nohara29 The inability to rescue medical facilities and restore power to hospitals can lead to a heavy workload among the medical rescue teams. Reference Cook, Shrestha and Htet28 The terrain of the affected region poses a significant challenge both in terms of logistics and secondary disasters. Reference Shen, Jiang and Zhang20 As a result of challenging terrain, the physical infrastructure is often inadequate for accessing the disaster-affected areas. Many rescue teams are unfamiliar and unprepared regarding the natural environment, geography, and in some cases, altitude. Reference Cook, Shrestha and Htet28 Cultural and local norms, relations with the press, and lack of safety and security briefings were other challenges faced by rescue teams. Reference Aitken, Leggat and Robertson14,Reference Leggat34 Several instances of intrusion and disrespect to local communities by the media were reported. Reference Cook, Shrestha and Htet28
Discussion
In this study, the results of our screening diagram showed that 18 documents included challenges faced by medical rescue teams. All the studies included in the final analysis were published in the year 1989 and onward, and over 50% of them were carried out from 2011 to 2021. The challenges faced by medical rescue teams during the response phase of sudden-onset disasters are investigated at 6 levels: organizational, individual, environment and health, logistics, information and communication, and other factors.
The emergence of administrative problems in a situation requiring management is indeed inevitable. Dealing with unpredictability and unexpected outcomes during disaster situations makes administrative issues a significant challenge. Reference Massalou, Ichai and Mariage35,Reference El Sayed, Chami and Hitti36 At the organizational dimension, coordination, inadequate leadership, and clear delineation of personnel roles and responsibilities play a crucial role. Failure to achieve effective coordination and lack of clear authority lead to confusion among medical rescue teams, resulting in delays in response actions. Therefore, it is necessary to make various improvements regarding the organizational issues encountered by medical rescue teams. In this regard, it is recommended to address aspects such as crafting context-specific guidelines, Reference Connelly22 clarifying the division of responsibilities, Reference Cook, Shrestha and Htet28 and defining a command structure. Reference Deverell, Ortenwall and Almgren25,Reference Nohara29
Hugelius et al., in one of their studies, has outlined the challenges encountered in disaster management in 5 categories: Identifying the situation and dealing with uncertainty, balancing the mismatch between the disaster contingency plan and the reality, establishing a functional crisis organization, adapting the medical response to the actual and overall situation, and ensuring a resilient response. Reference Hugelius, Becker and Adolfsson37 However, unlike Hugelius et al., we believe that it is not accurate to solely consider the challenges in disaster management from an operational perspective. Although our study has also identified coordination issues as the most frequently encountered problem, this is related to other factors identified in our research. Indeed, if problems in environmental and health control are overlooked, if communication and information issues are not addressed, and if deficiencies in logistics activities are not prevented, these coordination problems will persist. Therefore, taking a broader perspective when looking at the problems encountered in disaster response would be more accurate.
In the individual dimension, nutrition, hydration, accommodation, training and experience, and shift period constitute the most important factors that merit special attention. In a study conducted by Ghodsi et al., it was also revealed that having appropriate training and skills, self-care, adequate sleep and rest, and proper nutrition are factors that influence resilience among volunteers. Reference Ghodsi, Sohrabizadeh and Khani Jazani8 While Ghodsi et al. evaluated physical and mental health under the individual factor, this study has assessed them under the environmental and health factor. Sanitation, hygiene, protection from vectors, immunization, weather conditions, disease, injury, and psychosocial support are other important aspects that fall under the environmental and health factors. If the health of medical rescue teams is not good, they cannot respond adequately to the disaster. Therefore, addressing the individual shortcomings of medical rescue teams, resolving personal issues, maintaining health, completing training, and meeting basic needs are crucial for effective disaster response. Especially in this regard, conducting health checks of team members before response, Reference Tatham and Spens17 monitoring environmental and mental stress, monitoring illness and injuries, enforcing rest breaks, Reference Aitken, Leggat and Robertson14 and providing psychological support Reference Shen, Jiang and Zhang20 can alleviate the burden on the medical rescue teams to some extent.
Although medical rescue teams have the best intentions to intervene in disasters, in some cases, they may lack the necessary logistical support. Delays in the delivery of aid can occur due to logistical challenges. The main causes of these logistical problems are inadequate equipment and materials, incompatible machinery, insufficient vehicles and staff, and transportation issues such as traffic and congestion. In a study describing the initial response to a tsunami, it was reported that the roads leading to airports and other major cities were significantly damaged, and there was a shortage of medical supplies for medical rescue teams during the critical period after the disaster. Reference Lee, Low and Ng32 A study describing Ethiopia’s experience in disaster response highlights that, despite the lack of budgetary resources, teams continued to be deployed in various emergency situations. The study emphasizes that the challenges faced were not only limited to budgetary constraints but also the absence of an organized logistics depot. Reference Van Hoving, Smith and Kramer30 In this context, it is recommended to calibrate relief priorities, Reference Connelly22 effectively use available resources, Reference Djalali, Ingrassia and Corte23 increase the staff number of medical rescue teams, Reference Djalali, Khankeh and Öhlén18 and establish prior agreements with suppliers Reference Motamedi, Saghafinia and Bafarani33 to address logistical challenges.
The factors of considerable significance in the information and communication dimension are data collection, accurate information sharing, and network interruptions. Proper planning and intervention are possible through accurate data collection, rapid dissemination of information, and the availability of functional communication tools. While a small glitch in communication and information can create a risk for the safety of medical rescue teams, effective communication and information flow can mitigate adverse medical outcomes. To prevent information and communication issues, it is recommended to keep the contact information of the staff up to date, Reference Shen, Jiang and Zhang20 regularly practice communication, Reference Cook, Shrestha and Htet28 and collect and share information early. Reference Aitken, Leggat and Robertson14
Finally, other factors such as power outages, cultural and local norms, media relations, terrain, safety and security briefings that are not mentioned in the above dimensions, also include significant challenges faced by medical rescue teams. Aitken et al. highlighted that security issues, including briefings, evacuation plans, and exit strategies are major issues for deployed team members and need to be addressed in mission planning. Reference Aitken, Leggat and Robertson14
Limitations
The absence of a standardized method for reporting and evaluating crisis management, coupled with the reliance on lessons learned and shared experiences to formulate disaster response recommendations, underscores the need for a comprehensive synthesis in evidence development. Reference Gerdin, Clarke and Allen38,Reference Steigenberger39 Therefore, this study was inspired by the integrative review methodology. Like most reviews, the lack of access to all potentially related documents, including those that have not been published yet, was one of the limitations of the study. In addition, the inclusion of only English language articles led to missing some resources in other languages. Furthermore, this study did not encompass articles concerning slow-onset disasters, such as pandemics. Examining articles that tackle the difficulties encountered in slow-onset disasters will enhance our current understanding of disaster medical management.
Conclusions
The literature review revealed a limited number of studies addressing the challenges faced by medical rescue teams, and these studies were found to be insufficient in addressing the encountered difficulties comprehensively. Some studies focused only on organizational problems, while others only addressed health issues. In order for medical rescue teams to provide better care to disaster victims and effectively manage disaster events, there is a need for studies that are conducted on various factors and provide an integrated perspective on these problems. The findings of this review categorize the challenges faced by medical rescue teams into 6 factors and provide evidence that can be used by institutions, organizations, and governments.
Among the studies included in the findings, organizational challenges have been identified as the most prevalent factor that medical rescue teams encounter. Despite the frequent incidence of disasters, the persistence of organizational problems indicates a failure to learn from these disasters. To effectively manage disasters, it is necessary to ensure uninterrupted and continuous organization. However, when an organizational problem arises, it leads to the emergence of other challenges. Reference El Sayed, Chami and Hitti36 These organizational factors contribute to medical rescue teams encountering individual and health-related issues, disruptions in logistical activities, and communication and other problems. Additionally, these issues are also evaluated as factors that medical rescue teams encounter.
Failure to acknowledge or address the challenges and problems faced by medical rescue teams can hinder institutions and organizations from achieving their pre-established objectives, ultimately leading to inadequate services for those affected by the disaster. Additionally, medical rescue teams themselves may encounter various complications and may opt to prioritize their own physical and mental well-being by stepping away from their responsibilities.
In this study, each of the 6 categorized difficulty factors is likened to a gear in a mechanism where 1 problem triggers other problems. For example, a problem in the logistics of aid supplies can further disrupt coordination, burden medical rescue teams with heavy workloads, cause fatigue among medical rescue teams due to the heavy workload, and lead to errors in information sharing due to mental exhaustion. Therefore, we argue that taking a comprehensive approach by using the ‘ECOLIO’ (Environmental and health; Communication and information, Organizational, Logistics, Individual, and Other factors) approach to address the challenges faced by medical rescue teams in disaster response can help prevent the problems caused by these factors in the future.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2023.217
Author contribution
Ahmet Doğan Kuday: conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft. Tuğba Özcan: conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft. Cüneyt Çalışkan: conceptualization, supervision, writing – review and editing, revision. Kerem Kınık: writing – review and editing.





