



Unhealthy dietary behaviours can be attributed in part to obesogenic food environments(Reference Swinburn, Sacks and Hall1) both at the household(Reference Ong, Ullah and Magarey2) and at the community level(Reference Swinburn, Sacks and Hall1). One of the key architects of the food environment is the government. By its laws, policies and health promotion efforts, government actions can influence the availability (trade, food composition and food provision policies), accessibility (retail policies, labelling policies), affordability (fiscal policies) and promotion (marketing, labelling and educational actions) of foods(Reference Swinburn, Sacks and Vandevijvere3) which are key determinants of food choice. Indeed, several governments have recently introduced stronger regulatory measures such as taxation of sugar-sweetened beverages(Reference Backholer, Vandevijvere and Blake4) and front-of-pack labelling(Reference Jones, Neal and Reeve5) to improve environmental determinants of dietary behaviour. Characterising, monitoring and evaluating government actions are imperative for the continued development and improvement of policies that proactively engineer our environments to support healthy eating(Reference Peeters and Backholer6). Ongoing assessment of government policies may also increase accountability and serve as a measure of progress(Reference Vandevijvere, Mackay and Swinburn7).
In Singapore, having poor dietary choices is the leading behavioural risk factor for premature death and ill health, primarily from chronic diseases such as CVD and diabetes(8). In 2017, 36·2 % of Singaporean adults were overweight, 8·7 % were obese and 8·6 % had diabetes(9). By 2050, the prevalence of diabetes is projected to reach 15·0 %(Reference Phan, Alkema and Tai10). Recognising the urgent need to more comprehensively address this rise, the Singapore government announced a War on Diabetes in 2016, with improving dietary behaviours as a key strategic focus(11,Reference Png, Yoong and Phan12) . This includes creating supportive environments by providing healthier foods in schools and limiting food marketing. Singapore is an urbanised(Reference Chia13), high-income country, with a large reliance on food importation(Reference Tortajada and Zhang14), a high prevalence of eating out primarily at small independent eateries(Reference Naidoo, van Dam and Ng15) and a history of taking robust measures to address public health issues(Reference Amul and Pang16). Comprehensively mapping and evaluating the food environment policy landscape in Singapore are critical to identify areas of strength and policy gaps that need to be addressed.
Current efforts to evaluate the implementation of food environment policies are largely driven by international organisations such as the WHO and are typically limited in scope(17). More recently, several countries have used the Healthy Food Environment Policy Index (Food-EPI) to assess national-level government policies. This tool which is rated as high quality(Reference Phulkerd, Lawrence and Vandevijvere18) evaluates government actions as compared with best practices(Reference Swinburn, Sacks and Vandevijvere3,Reference Vandevijvere, Barquera and Caceres19) . In the current study, we used the Food-EPI process and tool to evaluate Singapore government actions to create healthier food environments and to prioritise areas for future action.
Methods
We largely followed the Food-EPI methodology that has been previously described(Reference Swinburn, Vandevijvere and Kraak20). Briefly, during a 1-d workshop in March 2018, an expert panel rated Singapore government actions according to international best-practice benchmarks across forty-seven good practice indicators of the Food-EPI. These indicators map to thirteen domains, namely seven food policy domains (composition, labelling, promotion, provision, price, retail and trade) and six infrastructure support (leadership, governance, funding, monitoring and intelligence, platforms for interaction and health-in-all policies) domains. Details of the methods are publically available(Reference Tay, Whitton and van Dam21); relevant extracts of the process are provided in online Supplementary Document 1.
Evidence compilation and verification
The evidence document for Singapore was iteratively compiled with input from the government including from the Ministry of Health, Health Promotion Board, Agri-Food and Veterinary Authority, Ministry of Social and Family Development and Ministry of Trade and Industry. Singapore’s government actions for the forty-seven indicators from July 2016 onwards were obtained by reviewing government documents and Singapore newspapers, and through personal communications with government officials. We sent this information to relevant ministries for clarification and verification, and pertinent inputs were incorporated. The finalised document was shared with the experts 2 weeks prior to the workshop.
Expert panel recruitment
In January 2018, expert panel members were recruited using purposive and snowballing methods. The panel comprised of twenty public health and nutrition experts from academia, non-governmental organisations and medical/professional associations (45·5 % response rate), with a larger proportion of women (75 %) and academics (65 %). The panel had broad representation of expertise across food policy domains with the exception of food trade. Experts were identified through purposive and snowball sampling methods by reviewing relevant peer-reviewed journal articles, local newspaper opinion pieces, name lists of national taskforces involved in developing obesity prevention policies and by recommendations. Food industry or government experts were excluded to limit potential conflicts of interest. Experts were contacted via email and those who agreed to participate were provided with a 1-h orientation session to facilitate familiarity with the Food-EPI process, the evidence document and the rating process.
Full day workshop: rating and proposing actions
There were two parts to the workshop, and the entire process was deliberative. At the workshop, for each indicator a summary of Singapore’s policy actions was first presented by two study team members. Government officials – who were present at the workshop as observers – responded to questions from the panel and provided updates on Singapore’s policy actions. Each expert then anonymously rated Singapore’s government action against international benchmarks for that specific indicator using a Likert scale from 1 to 10 (1 being ‘very little, if any’ implementation and 10 being ‘high’ implementation as compared with the benchmarks). Singapore’s policy was the best practice benchmark for two indicators: for subsidies that favour healthy food, and programmes to support the availability of healthier foods at retail food outlets. Rating was done using an audience response tool (TurningPoint ResponseCard RFLCD) which allowed live sharing of the distribution of the ratings, mean and median ratings, once all experts had rated the indicator. After rating all forty-seven indicators, participants were asked to prioritise up to ten of the forty-seven indicators anonymously based on importance and achievability for further discussion of concrete actions to be implemented by the Singapore government. The top eleven indicators were selected. The discussion was facilitated by two study team members. This session was audio-recorded and transcribed. Recommended actions were extracted from the transcripts by two researchers independently. This list was compiled and sent to the experts via email to verify for accuracy and completeness.
Data analyses
Median rating for each indicator was categorised into four implementation levels: ‘very little, if any’ (≤2·5), ‘low’ (2·6–5·0), ‘moderate’ (5·1–7·5) and ‘high’ (≥7·6). Inter-rater reliability was calculated with the Agreestat programme using the Gwet’s AC2 coefficient(Reference Gwet22). Recommended actions were classified using the Nuffield’s Ladder of intervention(23). This framework describes the spectrum of government policies to improve population health in view of their impact on an individual’s autonomy. Actions at higher rungs of the ladder are typically viewed as being more intrusive, therefore needing greater justification for implementation. As infringements on personal autonomy are often used as an argument against policy implementation(Reference Griffiths and West24), and as perceived impact on personal freedom is an important determinant of policy acceptance(Reference Diepeveen, Ling and Suhrcke25), this framework has been used to understand public sector policies in several public health fields despite its limitations(Reference Griffiths and West24). As an exploratory analysis, one of the authors who is trained in qualitative methods (Z.T.) coded the workshop transcript inductively for themes(Reference Braun and Clarke26,Reference Nowell, Norris and White27) to explore the main considerations of the expert panel for proposing actions during the discussion. The coder had no prior personal relationship with panel members or government officials but had attended modules of two panel members. The workshop transcript was first read broadly to identify key considerations, a coding framework was developed and this was subsequently applied to the entire transcript. The main themes are listed in online supplementary material, Supplemental Table 1 with examples of quotes.
Results
Overall, a large proportion of the indicators was assessed as ‘moderate’ (46·8 %) or ‘high’ (23·4 %) implementation when compared with international benchmarks (Table 1). More than a third of the infrastructure indicators received a ‘high’ or ‘at the level of best practice’ rating (33·3 %) whereas only two indicators (8·3 %) received a ‘very little or none’ implementation rating. In contrast, over a quarter (26·1 %) of the food policy indicators received ‘a very little or none’ rating. The Gwet’s AC2 inter-rater reliability coefficient was 0·71 (95 % CI 0·64, 0·78), indicating good agreement between experts on the ratings.
Table 1 Distribution of rating scores for forty-seven indicators across four levels of policy implementation in Singapore

Among the food policy indicators, food subsidies to favour healthy foods received the highest median rating score of 9·0 (Fig. 1), with Singapore being the only example available as the international benchmark. Other food policy indicators assessed as ‘high’ level of implementation included policies in schools and public sector settings to promote healthy food choices. Among the infrastructure support indicators, restricting commercial influence on policy development obtained the highest median rating score of 8·5. Several indicators in the leadership domain including the presence of strong, visible, political support, food-based dietary guidelines and a comprehensive implementation plan linked to national needs received high ratings.

Fig. 1 Ratings of indicators for the food policy and infrastructure domains for Singapore by level of implementation based on median rating scores (very little, if any: 1–2·5; low: 2·6–5·0; moderate: 5·1–7·5; high: 7·6–10). The number inside the bar is the median rating score of the indicator. Indicators with a * were prioritised for further discussion. ![]() , very little, if any;
, very little, if any; ![]() , low;
, low; ![]() , moderate;
, moderate; ![]() , high. NCD, non-communicable disease
, high. NCD, non-communicable disease
Indicators that were assessed as ‘very little, if any’ and ‘low’ level of implementation (median rating score ≤5·0) were largely in the food policy area and included indicators in ‘food promotion’ domain, and in the ‘price’ domain including ‘reducing taxes on healthy foods’, ‘increasing taxes on unhealthy foods’ and ‘ensuring that food-related income support is for healthy foods’. Infrastructure support indicators that received low ratings included ‘access to government information’, ‘using systems-based approach to prevent obesity’ and ‘assessing the impacts of food and non-food policies’.
Most indicators (nine out of eleven, 82 %) prioritised for further discussion were food policy indicators, and most (ten out of eleven, 91 %) received a median rating of ≤5·0. A total of twenty-five food policy actions and six infrastructure support actions were recommended by the expert panel. Actions were largely aimed at enabling or guiding food choice (Table 2) and none involved eliminating choice (e.g., banning certain foods) or using disincentives (e.g., taxation). More intrusive actions that reduce autonomy through restriction such as advertising limits were recommended for vulnerable populations such as children. Monitoring actions were typically recommended for policies that were self-regulated such as the code for regulating advertising of foods to children or where existing evidence seemed inadequate, such as characterising the price elasticities of foods to develop fiscal policies.
Table 2 List of thirty-one proposed actions for the Singapore government classified by its impact on autonomy using the Nuffield’s Ladder of intervention
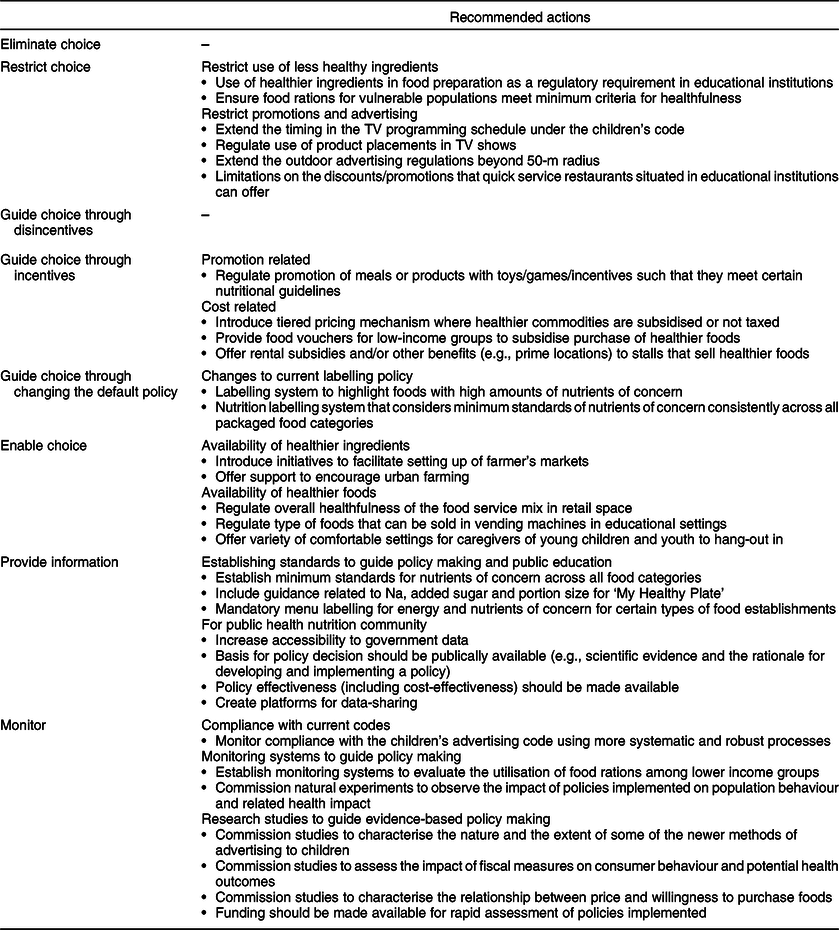
Considerations around political acceptability, opposition from industries, lack of conclusive evidence on effectiveness, operational difficulties, nature of the food retail environment in Singapore and complementary or bridging character of actions were brought up when discussing recommendations (see online supplementary material, Supplemental Table 1).
Discussion
Our findings suggest that while experts in public health nutrition in Singapore largely have a favourable view of the infrastructure support, several policy action areas remain to be more fully developed. Higher ratings for the infrastructure support domain, as compared with policy domain, have been observed in other countries(Reference Vandevijvere, Barquera and Caceres19). Global advocacy for governments to assume leadership in establishing an infrastructure to monitor and address chronic diseases and risk factors such as obesity is fairly recent(Reference Shahid and Bishop28). It is possible that with time, good infrastructure support may translate into robust policy actions. However, considering the urgency of the global obesity crisis, there is a need to better understand and strengthen facilitators that can catalyse this process.
Given its stable and uncorrupt governance(Reference Chia13) and successes in implementing strong tobacco regulatory measures(Reference Amul and Pang16), Singapore may seem to be well-positioned to take a leadership role in implementing robust food environment policy measures. Indeed, the presence of strong visible leadership and a health promotion agency with dedicated funding were seen as strengths by the panel. Nevertheless, existing pressures such as high reliance of the Singapore economy on trade(Reference Chia13) and food importation(29), its business-friendly reputation(Reference Chia13,30) and scarce land resources(Reference Chia13) may pose challenges in formulating policies for specific areas such as nutritional labelling, zoning or trade.
In line with previous studies(Reference Vandevijvere, Barquera and Caceres19), our panel recommended more rigorous policy actions such as restricting unhealthy food choices for vulnerable population groups such as children. Taxation of unhealthy foods, a regulatory measure which is increasingly adopted by other countries(Reference Backholer, Vandevijvere and Blake4), was not considered suitable for short-term implementation. This may be partly related to the perceived lack of contextualised information on price sensitivity of foods and responses to fiscal policies. Instead, the need to more clearly develop cut-offs for classifying healthfulness of packaged and cooked foods which can be used across policies or programmes was emphasised for more immediate implementation. Other policy approaches that were highlighted included better monitoring of existing policies such as the children’s advertising code which is self-regulated(31) and strengthening of policies such as front-of-pack labelling which comprises of a voluntary endorsement scheme(32).
Key policy areas prioritised by the Singapore panel such as setting compositional cut-offs for nutrients of concern and improving labelling policies were also emphasised by expert panels in Malaysia(Reference Ng, Swinburn and Kelly33) and Thailand(Reference Phulkerd, Vandevijvere and Lawrence34). This highlights potential opportunities for synergies and possibly the need for supra-national governance to improve the regional food environment, particularly as Singapore imports over 90 % of food products, with Malaysia and Thailand being important trading partners(Reference Tortajada and Zhang14).
Highly rated policy indicators, namely subsidies for healthy foods and programmes for healthier foods in schools and government settings, were all related to government actions to improve the availability of healthier foods at out-of-home settings. Over 75 % of Singaporean adults eat a meal prepared out-of-home on a daily basis(Reference Naidoo, van Dam and Ng15), mostly at small independent eateries(Reference Naidoo, van Dam and Ng15), which makes conventionally proposed measures such as mandatory nutritional menu-labelling challenging. Instead voluntary approaches are used to support the use of healthier ingredients by food vendors(35), and healthier food programmes are vigorously promoted for adoption in settings such as government facilities and public schools(36) which fall under government purview. In particular, the healthier ingredient development scheme, which provides funding support to oil manufacturers to promote the use of lower-saturated oil blends to food vendors at a price that is comparable to less healthier counterparts, received the highest rating amongst all indicators. Singapore’s actions to improve the out-of-home retail food environment add to the evidence base of policies which countries facing similar challenges could consider.
The Food-EPI methodology has several strengths, including rating across a comprehensive set of indicators and the employment of an engagement process between local experts and government that facilitates transparency and dialogue. While we broadly followed the Food-EPI process, we made contextual adaptations for Singapore. Specifically, we provided an in-person orientation to each expert to familiarise them with the structure of the evidence document and the workshop. We also used a voting system to prioritise key indicators to allow for more time for further discussion.
Recommendations from local experts are more likely to be anchored in an understanding of the geo-political realities and socio-cultural values of Singaporeans. While the evidence used to rate Singapore was limited by what was publically available and by what government officials were willing to share, we mitigated this by inviting government officials to the workshop as observers to provide updates. It is possible that the presence of government officials may have influenced ratings, but this was likely limited as ratings were kept anonymous. The responses of our panel may not fully reflect those of all local experts, as our response rate though similar to those observed in other countries(Reference Vandevijvere, Barquera and Caceres19) was modest, and there was limited representation of non-academics in the panel. The thematic analysis of the discussion was exploratory in nature and may not provide a comprehensive view of the factors considered by the expert panel as they propose future actions.
This work represents the first effort to comprehensively characterise and evaluate the food environment policy space in Singapore and provides guidance to government officials and public health advocates in their efforts to improve the food environment in Singapore and other similar urban Asian environments. Our results provide unique insights into the challenges and opportunities presented in designing healthier food environments and add to ongoing global efforts to characterise and evaluate government actions to support healthier eating. Important structural recommendations such as the need for profiling the healthfulness of foods and strengthening monitoring systems have the potential for improving the robustness of policy actions across domains.
Acknowledgements
Acknowledgements: We are grateful to Helena Legido-Quigley for her advice. We wish to thank the panel experts who participated in the study and the government officials who valdiated the evidence document. Financial support: This research was supported partly by the Physical Activity and Nutrition Determinants in Asia (PANDA) Programme under the Saw Swee Hock School of Public Health, National University of Singapore and Ministry of Education-Tier 1 grant (R-608-000-164-114). The funder has no role in the design, analysis or writing of this article. Conflicts of interest: One of the co-authors (Stefanie Vandevijvere) is a deputy editor for the journal. Authorship: Z.T. and S.A.R. wrote the first draft of the manuscript; B.S., S.V., C.K.S., R.M.V.D. and S.A.R. conceptualised the project; Z.T., C.W., R.M.V.D. and S.A.R. collected data; Z.T. and S.V. analysed data. All authors provided intellectual input in the design, analysis, interpretation and presentation of study results. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the National University of Singapore. Written informed consent was obtained from all participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020003468





