



Introduction
In 2013, the National Health Service (NHS) Standard Contract for Radiotherapy acknowledged that the duration of a patient’s travel to access radiotherapy in England should not exceed 45 minutes, as this is known to impact access to radiotherapy and subsequent treatment uptake. 1 Even before this, the Welsh Government identified, via the commissioning of the Cameron Report in 1996, Reference Cameron2 that access to radiotherapy services in Wales would be different to those for patients in England. This is due primarily to differences in the physical geography and population distributions of the two countries, Reference Purden, Jackson and Lewis3 as well as a fewer number of cancer centres. For context, one-third of Wales’ population lives in a rural area, compared to just 20% of England’s population. Reference Gartner, Gibbon and Riley4 As such, based on these factors, Cameron proposed that a travel time of 60 minutes better represented the country. Reference Cameron2
Before the COVID-19 pandemic, certain groups of patients receiving radiotherapy for breast cancer would attend 15 fractions of treatment, five fractions per week, plus visits for clinics, imaging and other services supporting the radiotherapy pathway. This was based on the UK START trial, which confirmed in 2013 that 40 Gy in 15 fractions was equivalent to 50 Gy in 25 fractions in terms of local recurrence and toxicity. Reference Haviland, Owen and Dewar5 In May 2020, a few months into the COVID-19 pandemic, Murray Brunt et al. published findings of the FAST-Forward trial, identifying a five-fraction prescription of radiotherapy, delivered once per day over five treatment days, as non-inferior and as safe as the international standard of 15-fraction treatments. Reference Murray Brunt, Haviland and Wheatley6 Based on these findings, South-West Wales Cancer Centre (SWWCC) moved to a 5-fraction treatment regime, for women with operable breast cancer requiring adjuvant radiotherapy to partial or whole breast.
When considering the effect of hospital visit reduction with the centralisation of health services, and their impact on the burden of travel, two competing theories emerge: the distance bias association and the distance decay association.
Distance bias is an association between patients living further from a single health service and having better health outcomes or higher access rates than those living closer. Reference Kelly, Hulme and Farragher7 Studies supporting this association report a positive relationship between increasing travel distance and survival rates for patients on an oncology pathway. Reference Lamont, Hayreh and Pickett8,Reference Lenhard, Enterline and Crowley9 Undoubtedly, motivation to travel any distance for care is a factor that affects patient outcomes, Reference Kelly, Hulme and Farragher7 but the role of referral bias to specific centres should not be ignored. Reference Lipe, Lansigan and Gui10
Distance decay is the opposite of distance bias. It is an association between patients living closer to a service and having better outcomes or higher access rates than those living further away. Reference Kelly, Hulme and Farragher7 There is far more literature to support this theory and consistent evidence to suggest that patients following a radical oncological pathway, receiving treatment in specialised, centralised centres, had longer survival than those managed elsewhere. Reference Woo, Kyrgiou and Bryant11 Further, Williams and Drinkwater demonstrated that increasing deprivation was correlated with lower rates of access to radiotherapy, which, when combined with the findings of a 2017 eMoov audit that found hospital quality is linked to average house price in an area, indicates that those travelling from areas of higher deprivation will often be travelling further than those living in more expensive, less deprived areas. 12,Reference Williams and Drinkwater13 Further research into patient perspectives is needed, to determine any potential impact travel has on decision-making when deciding on whether to undergo radiotherapy.
The debate between local care versus specialised, centralised services is multifaceted. Still, it must be considered if visit reduction and centralisation of services is a potential for patients accessing radiotherapy services in South-West Wales. This paper investigates the impact of different treatment regimes on patient travel burden.
Patients and Methods
An anonymised sample of 1516 patients who attended SWWCC between May 2017 and July 2018 was obtained, including appointment dates and times and home postcodes. 400 patients from this sample would have been eligible for the 5-fraction regime. This was generated by a crystal report, to extract anonymised treatment type and postcode date between two dates, from Mosaiq®, the local electronic medical record and patient management software. The data output at crystal report and mapping were independently reviewed and verified by two of the authors. Data interpretation was independently reviewed by three of the authors. Ethical approval was not required for clinical service review.
Several studies have determined transport accessibility levels to healthcare using Geographical Information System techniques by mapping car and public transport travel times and distances to healthcare facilities. Reference Titidezh14 Recorded data from Microsoft Excel were analysed using ArcGIS, ArcMap. Shapefiles of the British Isles were acquired from Digimap. 15 The Welsh roads shapefile was obtained from MapCruzin. 16 The Welsh population shapefile was available through the University of Edinburgh. 17 These files were used separately and together to form basemaps for the results. A generic.XLM file containing postcode data for all of Wales was used for geocoding of locations.
Patient-specific travel time data were calculated using Google Maps, using the patient’s postcode, the radiotherapy department’s postcode, and the patient’s appointment date and time. Using this information, a time range for the journey duration was predicted by Google Maps based on traffic patterns on the date and time of the appointment. To reduce the effect of any outliers, the median of the range of journey duration was used. This was recorded in an Excel spreadsheet.
An alternative site at Morriston Hospital was proposed to test the methodology for use in scenarios relating to the centralisation of services. Using the same method above, travel duration and distance were calculated for all patients to Morriston Hospital.
To estimate the best time of day to schedule patient appointments, and to reduce travel burden, a Google Maps Application Programming Interface for mass-calculation of travel duration at predetermined times of the day was used. Based on the patient’s location and travel requirements, the programme, found at Doogal.co.uk, tested departure times at 08:00, 12:00 and 16:00, simulating morning, afternoon and evening appointments. This could then be used alongside network analysis to visualise travelable distances within 60 minutes at different times of the day. To do this, iGeolise provided.KMZ files which were applied and edited using an ArcMap conversion.
For the journey duration analysis using patient-specific appointment date/time, it is assumed that all patients travelled by car or bus. Factors such as parking, walking to RT or waiting to receive RT were not factored in, due to related data not being collected as part of the normal patient pathway. The quickest route from patient postcodes to each RT centre was selected for all patients, and it was assumed that patients were travelling from their own postcodes.
Travel to attend treatments in line with the pre-COVID-19 pandemic 15-fraction regime was then recalculated for the current post-COVID-19 pandemic 5-fraction regime, using the same anonymised sample of patient postcodes.
Results
First, a point density visualisation map was produced using patient postcodes to visualise the population density and distribution of the sample (Figure 1).
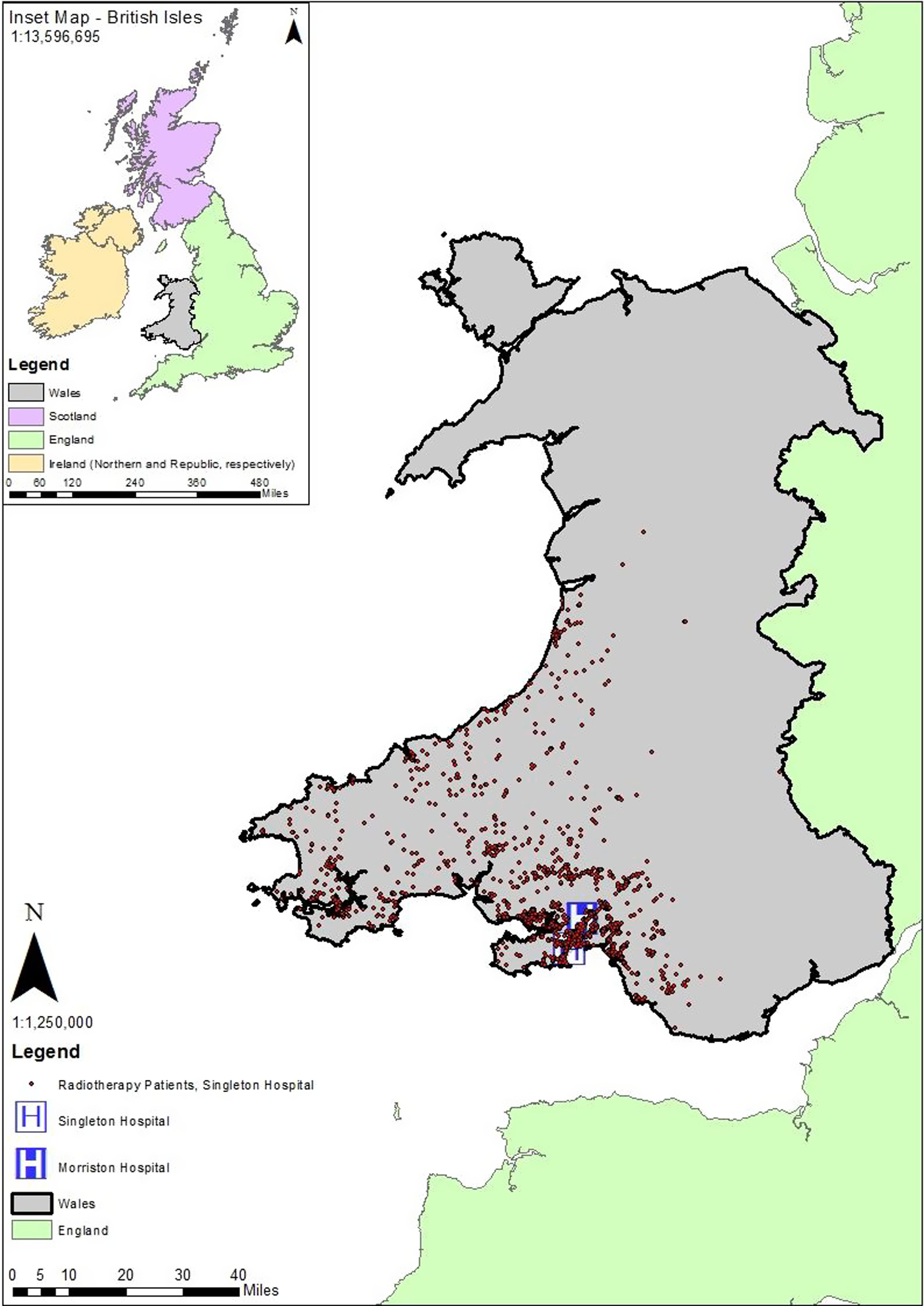
Figure 1. Point density map, depicting postcode locations of patients receiving radiotherapy at SWWCC, between May 2017 and July 2018.
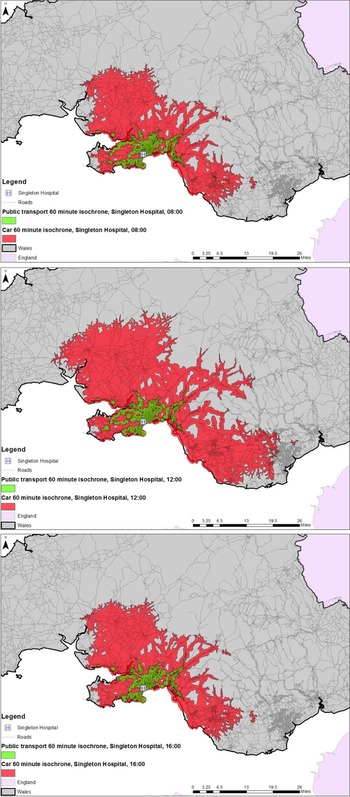
Figure 2 demonstrates the reachable area around Singleton Hospital, by car (red) and public transport (green), within the 60-minute guideline from the Cameron Report, Reference Cameron2 at 08:00, 12:00 and 16:00.

Figure 2. Isochrone maps showing the reachable area within 60 minutes of Singleton Hospital, by car and public transport at 08:00, 12:00 and 16:00.
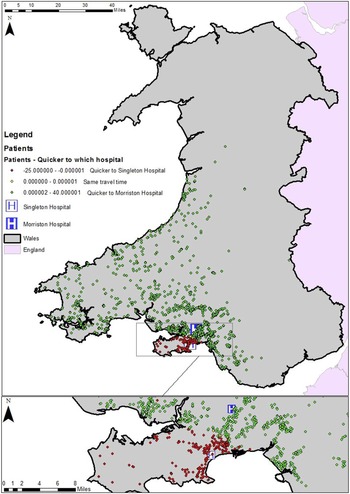
Of the 1515 patients whose journeys were mapped, 422 (28%) travelled for longer than the 60-minute recommendation of the Cameron Report. Reference Cameron2 Of the patients mapped in Figure 3, 87% (1316 patients) would have had a shorter journey by car if SWWCC had been located in Morriston Hospital (green), compared to travelling to Singleton Hospital (red). This number is reduced to 352 patients if travel to Morriston Hospital is considered. Figure 4 presents the locations of patients whose journeys would fall within the recommended travel time of the Cameron Report should the relocation of radiotherapy services to Morriston Hospital happen, which for this sample equated to an improvement of 5%. Reference Cameron2

Figure 3. Graphical representation of travel data to two sites in Swansea.

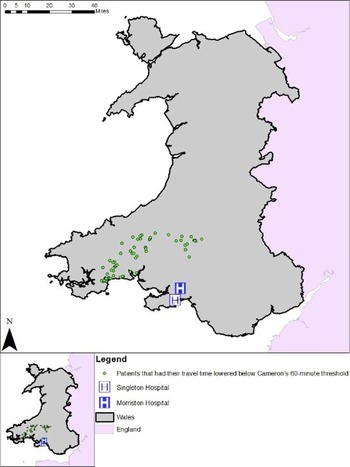
Figure 4. Map demonstrating patient postcodes which fall below the Cameron report (1996) recommendation, when travelling to Morriston Hospital.
192 patients had a shorter travel time to Singleton Hospital than they would to Morriston Hospital. Despite increased travel time to Morriston Hospital, none of these patients’ journeys was extended enough to breach the Cameron Report recommendation of 60 minutes. Reference Cameron2
The average travel time to SWWCC was 47.7 minutes by car and 118.0 minutes by public transport. Moving to the 5-fraction treatment regime saves 20 one-way trips to the hospital, resulting in an average time saving of 15.9 hours for those travelling by car and 39.3 hours for those travelling by public transport. A midday departure resulted in the shortest average journey time for those travelling by car, whereas an 8:00 departure was most efficient for public transport users. A significantly increased travel time resulted in departures at 16:00 for public transport users, requiring 12.3 extra minutes per journey compared to the 8:00 departure.
In an effort to quantify the environmental benefits associated with reduced travel, and considering NHS England’s ambition to be carbon neutral by 2040 and NHS Wales’ ambition to be carbon neutral by 2030, distances travelled were converted to carbon dioxide (CO2) emissions for travel by car. 18,19 CO2 emissions were calculated using a medium-sized petrol car averaging 30 miles per gallon, to account for varying traffic conditions. 20 Distances travelled for public transport were not calculated, as it is assumed that the public transport would still be in service. Table 1 shows the average distance travelled to attend radiotherapy treatments and related CO2 emissions.
Table 1. Average distance and CO2 emissions for patients travelling to Singleton Hospital

Discussion
The reduction in treatment fractions results in a decreased travel burden of 15.9 hours for those travelling by car and 39.3 hours for those travelling by public transport. These are considerable reductions and could encourage those who were hesitant to pursue therapy due to travel burden, to take up the treatment option, in line with the distance decay theory. Reference Kelly, Hulme and Farragher7,Reference Woo, Kyrgiou and Bryant11 Currently, SWWCC treats around 400 breast cancer patients per year with a five-fraction regime. This means that, collectively, 6360 hours of travel time are being saved each year, compared to the 15-fraction regime.
Nevertheless, the data demonstrate that relocating radiotherapy services from Singleton Hospital to Morriston Hospital would result in a significant travel time reduction for most patients currently accessing SWWCC; mean journey time per fraction would reduce by almost 10 minutes, one way. Importantly, while travel times to both Singleton and Morriston fall within the recommendation of 60 minutes made in the Cameron Report, Reference Cameron2 relocation to Morriston Hospital would also reduce travel time below the 45-minute guidance outlined in the NHS Standard Contract for Radiotherapy. 1 In the sample studied, these travel time savings total 251 hours in just one direction. Pagano et al. Reference Pagano, Di Cuonzo and Bona21 demonstrated that radiotherapy access decreased as the distance between the patient’s home and the cancer centre increased. A decrease in access was particularly notable for the older community members. More widely, Nicholl et al. Reference Nicholl, West and Goodacre22 demonstrated the effect of increased travel distances. Their study showed that an increase of 10 km (6.2 miles) in travel distance was associated with a 1% increase in mortality in emergency cases. Kelly et al. Reference Kelly, Hulme and Farragher7 demonstrated that, in northern countries within Europe, residing further from a hospital resulted in less favourable outcomes for 77% of patients.
In terms of distance travelled, despite the exemplar relocation of services to Morriston Hospital, the mean distance travelled to access radiotherapy services at SWWCC would still be 10 miles further than the average single journey for centres in England. Reference Coombs, Coombs and Vaidya23 It also does not solve potential stressors relating to parking for appointments once the patients have arrived, or the need for patients to factor in extra time if travelling by public transport, to account for waiting and cancelled or delayed services. In fact, the Welsh Deputy Minister for Climate Change stated in March 2022 that public transport services in Wales were not good enough, elaborating that, despite transport accounting for 20% of the country’s carbon emissions, bus networks are not robust enough to ensure reliable and sustainable access to services. Reference Waters24
When public transport is compared to travel by private car, total travel burden to access radiotherapy services at Singleton Hospital doubles. Travel to Morriston Hospital by public transport would increase travel burden even further, amounting to three times the burden of travel by car. These significant increases in travel times are thought to be due to the poor public transport links in South Wales and may be a more frequent issue due to the population distribution of Wales. One-third of all those living in Wales live in a rural setting. 25 The majority of patients coming into Swansea would need to change transport in the city centre, either at the central bus station or the train station. Often, their first bus would travel close to either hospital but would not stop there. This was more pronounced for travel by public transport to Morriston Hospital, in which patients would need to take a bus into the city centre, followed by a bus back out again. In a very small number of cases, patients lived on a direct bus route between the two hospitals, meaning their travel burden was minimally impacted by a change in treatment location. Finally, this does not consider the potential need for a taxi to the nearest bus stop, adding another leg to the journey.
These findings are supported by Robineau, Reference Robineau26 who also found that journeys by public transport result in travel times that are double what they would be by car, for rural populations. In their 2017 report, 27 Age UK surveyed people aged 65 and older, finding that 24% were worried that there was no access to their local hospital via public transport. For those with access to public transportation, the main reported worries were the need to take more than one bus to arrive. That said, some have argued that using an outcome-based referral, to centralised specialist units improves the quality of patient care. In other fields of medicine, Wouters et al. Reference Wouters, Karim-Kos and le Cessie28 demonstrated a reduction in postoperative morbidity and length of stay, with mortality falling from 12 to 4%. They found that the hospitals with the highest procedural volume showed the biggest improvement in outcome, after centralisation.
Regarding CO2 emissions associated with travel to patient appointments, when compared to a 15-fraction treatment regime, the 5-fraction FAST-Forward regime results in an average CO2 emissions reduction of 9.1 kg per hospital visit. In total, the reduction in CO2 emissions for the patients studied would equate to taking 29 cars off the road each year. 29 This demonstrates that moving to a 5-fraction treatment regime not only benefits patients via reduction in travel burden but also moves the NHS closer to its target of being carbon neutral by 2040. 18
Regarding scheduling appointments based on patient travel and location, the data show that there is value in tailoring appointment times to patient needs. It has already been established that elderly patients are less likely to receive recommended radical radiotherapy, with reluctance to travel being a key component, Reference McAleese, Baluch and Drinkwater30 so any further measures, such as video appointments, e-learning and other remote offerings, should be reviewed, as the potential for further reduction in travel burden could sway the decision of some towards treatment. Data on patient views of parking and walking to appointments could also be collected, to provide a more holistic view of travel burdens associated with radiotherapy.
Conclusion
Updating treatment techniques based on the findings of the FAST-Forward Trial in 2020 has resulted in a considerable reduction in travel burden for patients attending SWWCC for radiotherapy. Access to radiotherapy services in South-West Wales is mixed, with some areas experiencing large travel burdens. Relocation of radiotherapy services from Singleton Hospital to Morriston Hospital would reduce the travel burden for those travelling by car. Still, it would drastically increase the burden for those needing public transport. More should be done to reduce the number of hospital visits patients must make without reducing the quality of care they receive. Further research should explore the potential for a reduction in hospital visits at other points of the patient pathway, for example, by utilising online or remote resources. Patient views should be central to further research and any subsequent changes in practice.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.


 Open access
Open access