



Introduction
Chronic kidney disease (CKD) is a serious public health issue worldwide; the global estimated prevalence is 11–13 %, with the majority of cases at early stages(Reference Hill, Fatoba and Oke1). Strategies to reduce burden and costs related to CKD include the prevention and management of those patients at risk or with early renal function decline(Reference Obrador, Mahdavi-Mazdeh and Collins2).
Appropriate nutritional care has been recognised as a key factor in this endeavour. Dietitians can help to manage early CKD and prevent CKD onset in high-risk groups (i.e. diabetes mellitus and hypertension) by providing dietary advice to weight reduction, decrease blood pressure, glycaemic control, improve lipid profile, reduction of microalbuminuria/proteinuria and provide advice on healthy eating strategies(Reference Kramer3,Reference Ikizler, Burrowes and Byham-gray4) . Nevertheless, gaps in knowledge regarding CKD prevention and early treatment in high-risk groups were reported among these health professionals. A previous study showed that only 23 % of dietitians self-reported having adequate knowledge to provide nutritional care in early CKD; furthermore, solely 10 % of them identified diet contribution to initial kidney damage(Reference Márquez-Herrera, Cueto-Manzano and Cortés-Sanabria5).
In order to provide a complete, safe and suitable care as part of multidisciplinary team, it is crucial that dietitians comprehend the role of nutrition management in the prevention and early treatment of CKD(Reference Anderson and Nguyen6); therefore, they need to know how to implement knowledge, i.e. possess clinical competence (CC), which combines knowledge, skills and attitudes in clinical situations(Reference Miller7). Educational interventions designed to increase CC of family physicians in the management of early CKD already have demonstrated a positive effect on kidney function; however, variables related to healthy eating and lifestyle need the intervention of a qualified dietitian to help delay CKD progression(Reference Cortés-Sanabria, Cabrera-Pivaral and Cueto-Manzano8).
A first step to measure and improve CC among dietitians, particularly in primary health care, is having an adequate instrument to determine it and identify knowledge gaps for a better tailoring of resources. There are no studies determining the CC of dietitians with regard to improving patients’ kidney function and preventing kidney disease progression. It is necessary to develop a tool to assess the skill of acquiring information from a variety of human and laboratory sources, to analyse and interpret these data, and finally to translate such findings into a rational diagnostic and/or management plan(Reference Miller7). Therefore, the aim of the present study was to develop and validate a test to evaluate dietitian's CC about nutritional care of patients with early CKD.
Subjects and methods
Study design
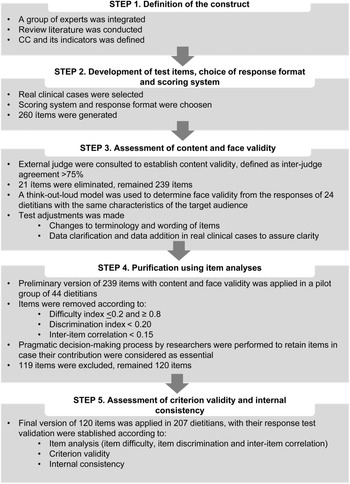
A descriptive validation study was carried out. The test development and validation consisted of five steps: steps 1 and 2 included the process of initial test development to measure CC about early CKD among dietitians, steps 3 and 4 lead to a preliminary test that finally was subjected to validation in step 5 (Fig. 1). Methodology to develop and evaluate nutrition knowledge questionnaire proposed by Trakman et al. (Reference Trakman, Forsyth and Hoye9) was used as a guide to achieve the objective of the present study.
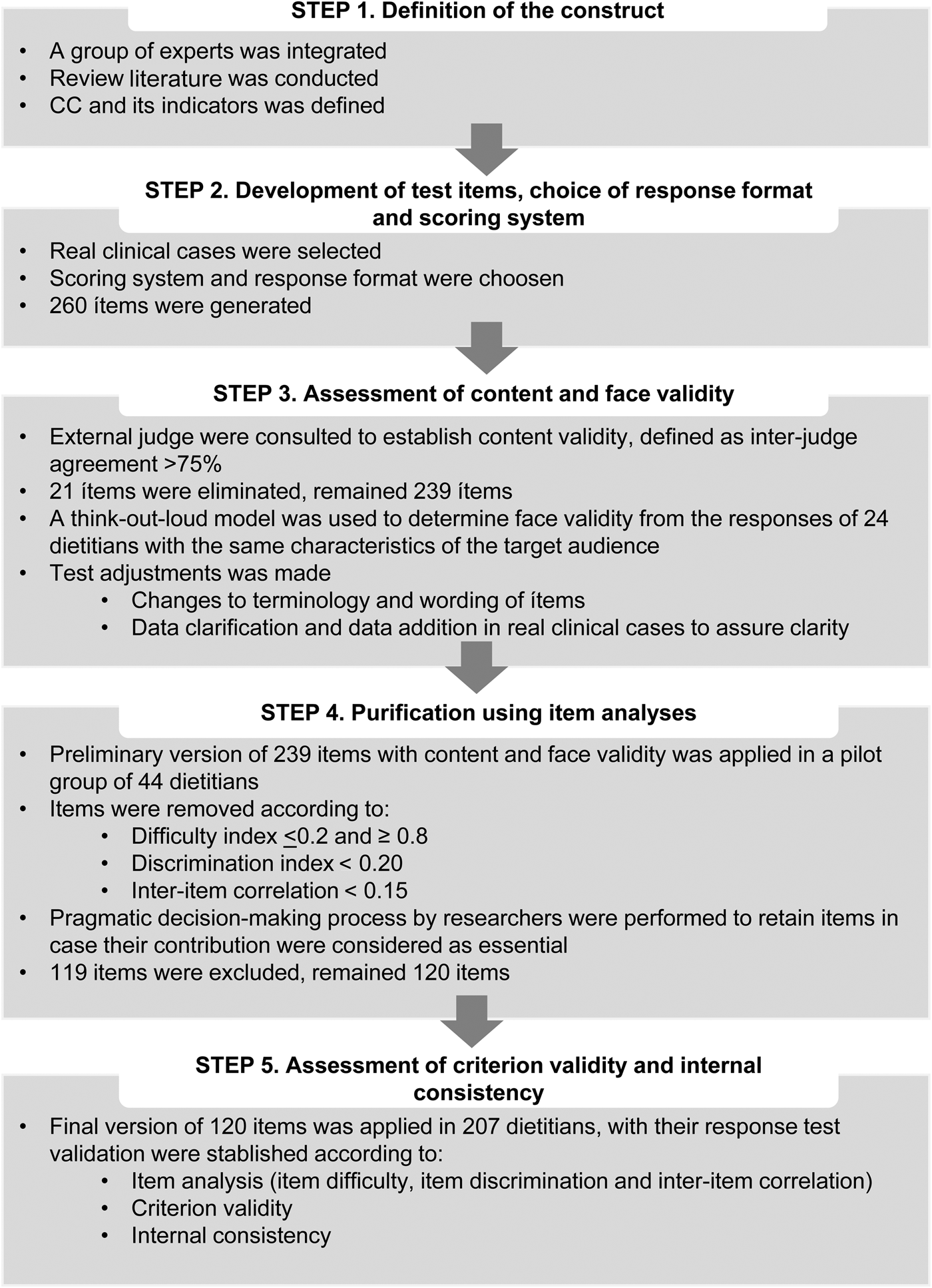
Fig. 1. Steps involved to develop and validate the test to evaluate dietitian's clinical competence about nutritional care of patients with early CKD.
Step 1. Definition of the construct
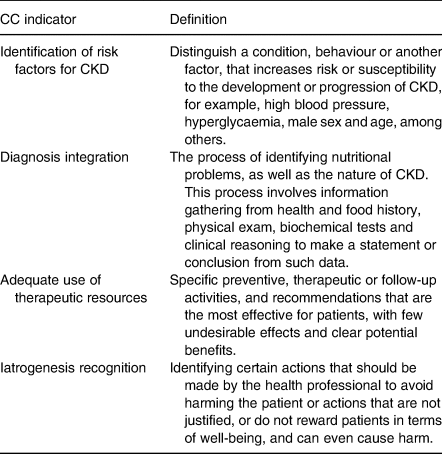
The first step was to define CC regarding nutrition in early CKD to ensure an appropriate conceptual framework. For this purpose, a workshop was held with a group of seven experts: three renal dietitians, three physicians (nephrology, internal medicine and family medicine) and one psychometrics expert. According to Miller(Reference Miller7), health professionals must know how to use the knowledge they have accumulated, and develop, among other things, the skill of acquiring information from a variety of sources, to analyse and interpret the data, and finally to translate such findings into a rational diagnostic or management plan. On the basis of this construct, CC was defined as the ‘ability to integrate and apply knowledge, skills and judgement to provide safe and effective nutritional care in CKD’. Competence was evaluated using the following indicators: identification of risk factors for CKD, diagnosis integration, adequate use of therapeutic resources and iatrogenesis recognition, as described in Table 1.
Table 1. Definition of clinical competence and its indicators
Step 2. Development of test items, choice of response format and scoring system
Once CC and its indicators were defined, in the same workshop, four clinical cases from patients at risk or with early CKD at the primary healthcare were selected. By using these real clinical cases, and considering the conceptual framework developed in Step 1, as well as relevant reviewed literature (including clinical practice guidelines and peer-reviewed journal articles), items (close-ended questions) were generated by the panel of experts. Two hundred sixty items were initially generated, following the suggestion to develop an item bank with at least double the amount that will appear in the final version(Reference Haladyna10) (about 100 final items were expected; twenty-five per each clinical case). Answer options were true, false and don't know. A balance between true and false statements (50 % of each option) was achieved. The scoring system was as follows: each correct answer adds one point (+1), incorrect answer subtracts one point (−1) and don't know option did not affect the score. The balance between true and false statements, and the ‘don't know’ option, may reduce the probability of correctly guessing the correct option, as previously suggested(Reference Haladyna10).
Step 3. Assessment of content and face validity
Content validity relates to the ability of a questionnaire to adequately cover all relevant topics of the construct(Reference Mokkink, Terwee and Patrick11). To assure content validity, the initial test (260 items) was evaluated by external judges regarding relevance, a group of three to ten experts is required to meet this goal(Reference Polit, Tatano Beck and Owen12); in the present study, four dietitians specialised in nephrology (different from those of the group of experts constructing the test), and recognised as experts in our setting, were the external judges. Each external judge rated individual items for relevance on a 4-point Likert scale (1 = not relevant, 2 = somewhat relevant, 3 = relevant, 4 = very relevant). The content validity index was calculated by dividing the number of external judges who scored the item as 3 or 4 divided by the total number of judges; a score of >0⋅75 was considered as adequate to keep an item(Reference Polit, Tatano Beck and Owen12). After this evaluation, from the initial 260 items, twenty-one were eliminated, remaining 239 items.
Face validity refers to the appearance of reasonableness of the test from the perspective of the test-taker and could be considered an aspect of content validity(Reference Mokkink, Terwee and Patrick11). Consequently, the test was completed by twenty-four dietitians with the same characteristics of the target audience for whom it was created, in order to confirm that instructions were easy to follow, to determine how long the test requires to complete and to evaluate the appropriateness and formulation of the items. A think-out-loud model was used, in which the participants verbalise their thought process as they complete the test, and when finalised the whole test, they meet with the researcher to discuss his/her experience of completing it. After this process, the researcher made necessary changes to terminology, wording and adding specific data to ensure face validity.
Step 4. Purification using item analysis
Once results of content and face validity processes were incorporated into the test, a preliminary version of 239 items was applied to a pilot group of forty-four dietitians with similar characteristics of the target sample to perform item analysis. Item analysis refers to a range of classical test theory techniques based on mathematically correlations between items and the degree that a person's true score on a test reflects their observed score and measurement error(Reference Trakman, Forsyth and Hoye9). For this purpose, results of the pilot group item difficulty, item discrimination and inter-item correlation were analysed and used to eliminate those items with inadequate performance.
(a) Item difficulty (severity or facility) assesses the percentage of respondents correctly answering an individual item(Reference Haladyna10). For example, if 90 % of participants answer correctly a particular item, the difficulty index was calculated as 0⋅9. Items with difficulty indexes of <0⋅2 and >0⋅8 were considered as too difficult and too easy, respectively, and were excluded(Reference Haladyna10).
(b) Item discrimination is calculated based on the general notion that high-scoring students tend to choose the right answer and low-scoring students tend to choose the wrong answer(Reference Haladyna10). If a person does well overall but poorly on a particular item (and vice versa), the item is said to be a poor judge (or discriminator) of knowledge(Reference Trakman, Forsyth and Hoye9). To estimate the discrimination index, cut-off 25th and 75th percentiles of the total score were used, then the percentage of individuals in each group who endorsed correct/incorrect statements was evaluated(Reference Cappeleri, Lundy and Hays13). For example, if 70 % of the high-scoring group and 20 % of the low-scoring group endorse a particular item in the scale, the discrimination index for that item was calculated as 0⋅75−0⋅20 = 0⋅55. Items with a discrimination index of <0⋅20 were removed(Reference Haladyna10).
(c) Inter-item correlation exposes that items with very high correlations may be assessing the same idea, whereas items with low correlations may suggest items that are too assorted to be assessing an isolated concept(Reference Trakman, Forsyth and Hoye9). For example, an item with inter-item correlation of 0⋅95 can be considered redundancy among the items, whereas an item with inter-item correlation of 0⋅1 is assessing a very different idea from the rest of the items. From this analysis, those items with inter-item correlation coefficient of <0⋅15 were eliminated(Reference Streiner14).
In spite of results of item analysis, some individual items were useful beyond their contribution to the total score and provided key information about gaps in CC about early CKD among dietitians. Therefore, a pragmatic decision-making process before removing items was employed, as previously suggested(Reference DeVellis15). At the end of this step, 119 items out of 239 of the preliminary test were excluded. The final test contained 120 items (available as supplementary material).
Step 5. Assessment of criterion validity and internal consistency
The final test (120 items) was applied to 207 dietitians for the assessment of internal reliability and criterion validity and compute the final item analysis on a large sample.
Criterion validity refers to the degree to which scores of the test are an adequate reflection of a ‘gold standard’; in the present study, it was expected that dietitians with previous training had the highest mean score, which differs significantly to demonstrate criterion validity.
Internal consistency assesses the degree to which items within a test are interrelated and measures the same construct(Reference Mokkink, Terwee and Patrick11). Cronbach's α was used to determine internal consistency.
Recruitment and study sample
The recruitment of dietitians was done by means of the ‘snowball technique’, in which one interviewee gives the researcher the name of at least one more potential interviewee that met the inclusion criteria for the study(Reference Kirchherr and Charles16), meaning professional with a bachelor's degree in nutrition complete, graduates from the University of Guadalajara, the largest university in our setting (Jalisco, México), or from a university incorporated (same academic curricula) to the last. Invitations were sent, and for those who agreed to participate, the test application was individual or in an organised meeting with small groups. The recruitment and data collection period was January 2018–January 2019.
Ethical considerations
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Ethics Committee of the University of Guadalajara, under protocol number 01917. Written informed consent was obtained from all subjects/patients.
Statistical analysis
Data are shown as mean ± standard deviation or median and 25th–75th percentiles, when dimensional variables had parametric or non-parametric distribution, respectively, or as percentage in the case of nominal variables.
For test validation (step 5), the following analyses and cut-offs were used.
For internal consistency, a Cronbach's α of ≥0⋅70 was considered adequate(Reference Trakman, Forsyth and Hoye9). To establish criterion validity, the Mann–Whitney U test was applied to compare dietitians with and without previous CKD training. The latter test and χ 2 were used to compare general characteristics between both groups of dietitians. A P value of <0⋅05 was considered as significant.
Items with difficulty index in the range of 0⋅2–0⋅8, discrimination index >0⋅2, inter-item correlation >0⋅15 and balance of 50 and 50 % of true and false statements were considered as ‘ideal’, as previously reported(Reference Trakman, Forsyth and Hoye9,Reference Haladyna10,Reference Streiner14,Reference Hingorjo and Jaleel17) . Tests with missing data were not included in the analysis.
Results
Two hundred and seven dietitians participated in test validation of the final version containing 120 items (Table 2). Most participants were women (91 %), aged 26 (24–29) years. A majority had a bachelor's degree, only 9 % had a master's degree or PhD and the median time after graduation was 4 (1–6) years. Participants had 2 (0⋅5–3) years of practice in nutrition counselling, and 38 % treated patients with CKD. Forty-eight percent reported had previous training in non-communicable diseases (i.e., diabetes, hypertension, dyslipidaemia and obesity), and 20 % had previous CKD training; the latter subjects were considered as the ‘gold standard’ group to establish criterion validity. Table 2 also shows comparisons of characteristics of dietitians with and without CKD training. Participants with previous CKD training had significantly more years of laboral experience, treated more patients with CKD and had training in other non-communicable diseases more frequently than those without previous CKD training.
Table 2. Characteristics of dietitians in the final test (120 items), according to the previous CKD training
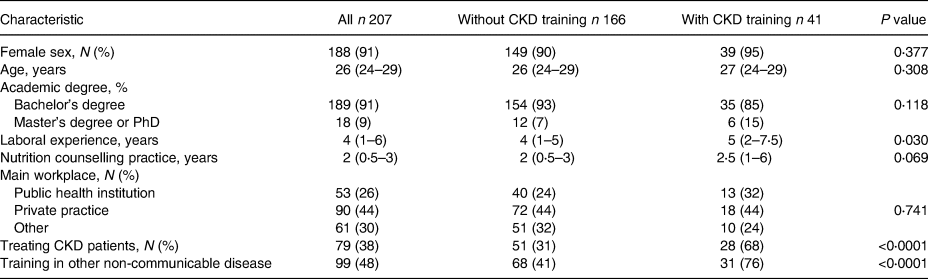
PhD, philosophy degree; CKD, chronic kidney disease; CC, clinical competence.
Data are shown as percentage or median (25th–75th percentiles).
From responses of the 207 dietitians subjected to the final test, the item analysis was as follows: 73 % had a difficulty index between the average (0⋅2–0⋅8), 2⋅5 % was classified as difficult and 24 % as easy. In addition, 62 % of the items had an adequate discrimination index (above 0⋅20), and 67 % had an adequate inter-item correlation (above 0⋅15). Table 3 shows the item analysis and internal consistency grouped according to CC indicators. The items belonging to each CC indicator had a balance near to 50 % between true and false statements. Mean values of difficulty index, discrimination index and inter-item correlation were as recommended in all groups of items, except for the discrimination index of identification of risk factors for CKD. Regarding Cronbach's α coefficient, the value of the complete test was 0⋅85, considered as an appropriate internal consistency to evaluate global CC, whereas the α values of the individual CC indicators scored lower.
Table 3. Item analysis of the final test (120 items)
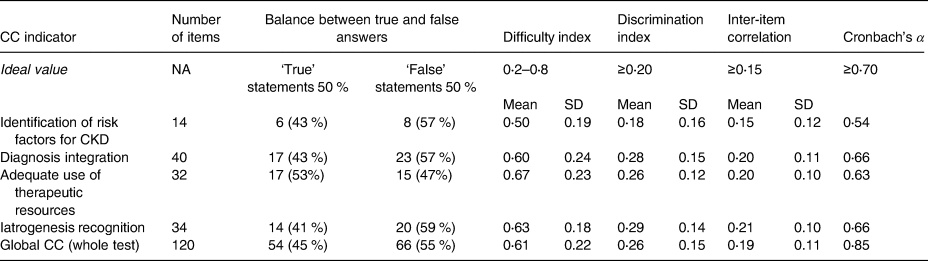
NA, not applicable; CC, clinical competence; CKD, chronic kidney disease; SD, standard deviation.
Data are shown as mean ± standard deviation.
Table 4 displays the results of assessment of criterion validity according to the previous CKD training status. As expected, the mean score of the global CC as well as the individual CC indicators were significantly higher for dietitians with CKD training in comparison with dietitians without previous training, supporting the criterion validity.
Table 4. Assessment of criterion validity by mean score comparison according to the previous CKD training status
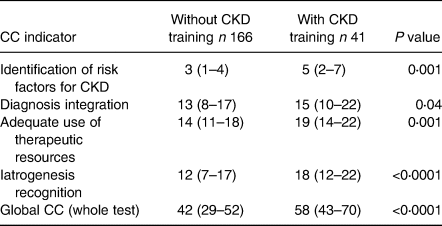
CC, clinical competence; CKD, chronic kidney disease.
Data are shown as median (25th–75th percentiles).
Discussion
The present study was performed to develop and validate a test evaluating dietitian CC about nutritional care in patients with early CKD. Nutrition intervention is effective in the control of risk factors for CKD but demands specialised training(Reference Anderson and Nguyen6,Reference Kent, McCarthy and Burrowes18) ; noteworthy, there is a scarcity of tools in this area.
Validation was achieved in several aspects. First, the availability of some experienced dietitians made it possible to ensure content and face validity (items covered the concepts they intend to measure and have clear instructions and adequate vocabulary). Additionally, purification of items, eliminating those redundant or inappropriate, reduced size of the test at the time that improved performance. Secondly, the analysis of the final test results shows that most of the items had satisfactory difficulty, discrimination capacity and inter-item correlation while maintaining the balance of true/false statements. Thirdly, the complete test shows adequate internal consistency according to Cronbach's α coefficient; however, isolated CC indicators (test subsections) should be used cautiously as its α values decreased when analysed individually, previous reports suggest that a higher number of items is associated to greater internal consistency(Reference Streiner14,Reference Steyn, Labadarios and Nel19) . Finally, when test responses were compared between two groups of people who a priori were expected to have different results, results confirmed the criterion validity. Dietitians who had previous CKD training (selected as the ‘gold standard’ group) also had more training in other chronic diseases, more interaction with CKD patients and longer time after graduation compared to the group of dietitians who were expected to score worse on the test; these differences also contribute to ensure criterion validity.
The present study does have limitations and strengths. The sample size was not calculated a priori by probabilistic methods (methods for sample size calculation in validation studies are limited); however, some authors recognise that a sample size of ‘200’ is fair(Reference DeVellis15) or satisfactory if include a greater number of respondents than the number of questions(Reference Parmenter and Wardle20), as done in the present study. Our sample was mainly composed of women; however, in our country (as in some others), women largely predominate as nutrition professionals(Reference King21). On the other hand, conditions to evaluate the scale's factor structure using exploratory factor analysis were not met, nor the evaluation of temporal stability using test–retest. The latter would be related to the length of the test (more than 2 h to complete) that could limit the recruitment of health workers. Notwithstanding, except for the latter analyses, the validation in the present study included all other steps of the methodology for a nutrition knowledge questionnaire(Reference Trakman, Forsyth and Hoye9): definition of the construct by a panel of experts, generation of the item pool, choice of an appropriate scoring system and response format, assessment of content and face validity, purification of the scale and gathering of data to re-examine the questionnaire's properties considering item difficulty, item discrimination, inter-item correlation, internal consistency and criterion validity. Adherence to this rigorous test development and validation process is one of the strengths of the present study, but the main merit might be to have evaluated CC, because this involves assessing not only knowledge, but also its application, and the capability of dietitians to identify risk factors for CKD, integrate a diagnosis, use appropriately therapeutic resources and recognise iatrogenic behaviour. In clinical setting, all those aspects are relevant since lack of training can negatively affect the nutritional therapy of patients on risk to progress to end stages of CKD. A previous test assessing CC in early CKD was validated for primary care physicians(Reference Cortés-Sanabria, Cabrera-Pivaral and Cueto-Manzano8), but not for dietitians. To the best of our knowledge, the present is the first test developed in this regard.
Practical implications
CKD is a growing epidemic worldwide, and dietitians have an essential role in its prevention and management; however, it is first necessary that dietitians display adequate knowledge and CC in this regard. It is recognised that the use of poor-quality nutrition knowledge questionnaires with unknown validity and/or reliability limits the conclusions that can be drawn from research in the nutrition education field(Reference Parmenter and Wardle20). The present questionnaire describes step by step, in a detailed manner, the process of development and validation to assess dietitians’ CC, and it is a suitable and easy tool to differentiate professionals with adequate competence from those who require further training. Moreover, the use of this test could reliably identify the effect of educational interventions to improve CC and catalyse investigation on dietitian education.
Conclusions
In conclusion, the present study encompassed the development and validation of a test to determine dietitian's CC about nutritional care of patients with early CKD. The final test has face, content and criterion validities, as well as satisfactory internal consistency.
The developed test is a reliable and valid tool to assess dietitian CC about nutritional care of patients with early CKD. It is a promising test in the development and guidance of public health actions related to the prevention and early management of CKD patients. Research is warranted to determine the CC of early CKD among dietitians.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2022.4.
Acknowledgements
This research did not receive financial assistance.
R.M.M.-H., L.C.-S., A.M.C.-M. and H.R.M.-R. designed research; R.M.M.-H. and C.N.O.-G. conducted research; R.M.M.-H., E.R.-C., A.G-P. and H.R.M.-R. analysed data or performed statistical analysis; R.M.M.-H., A.M.C.-M., L.C.-S., C.N.O.-G. wrote the paper; R.M.M.-H., A.M.C.-M. and L.C.-S. had primary responsibility for the final content. All authors have read and approved the final manuscript.
There are no conflicts of interest.







 Open access
Open access