



 Open access
Open access
Crossref Citations
This article has been cited by the following publications. This list is generated based on data provided by Crossref.
Sansom, Sarah E.
Gussin, Gabrielle M.
Singh, Raveena D
Bell, Pamela B
Benson, Ellen
Makhija, Jinal
Froilan, Mary Carl
Saavedra, Raheeb
Pedroza, Robert
Thotapalli, Christine
Fukuda, Christine
Gough, Ellen
Marron, Stefania
Villanueva Guzman, Maria Del Mar
Shimabukuro, Julie A.
Mikhail, Lydia
Black, Stephanie
Pacilli, Massimo
Adil, Hira
Bittencourt, Cassiana E.
Zahn, Matthew
Moore, Nicholas
Sexton, D.
Noble-Wang, Judith
Lyman, Meghan
Lin, Michael
Huang, Susan
and
Hayden, Mary K.
2022.
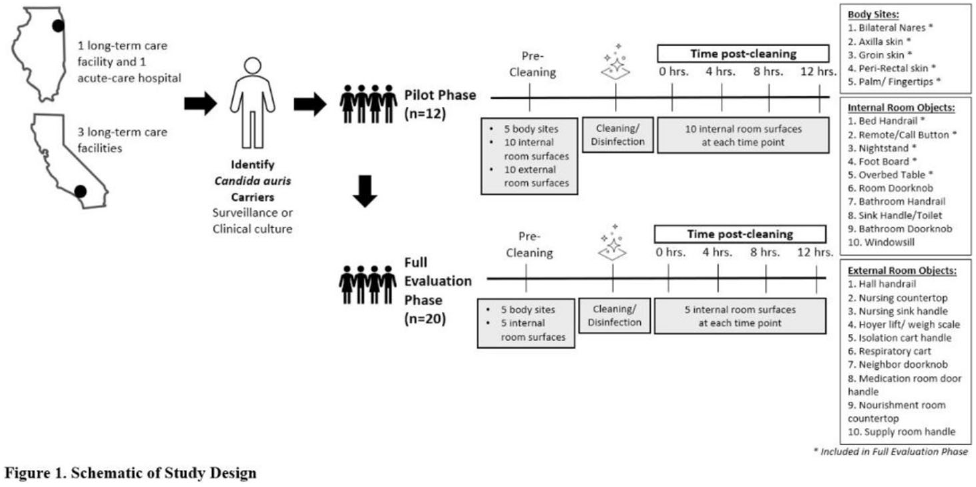
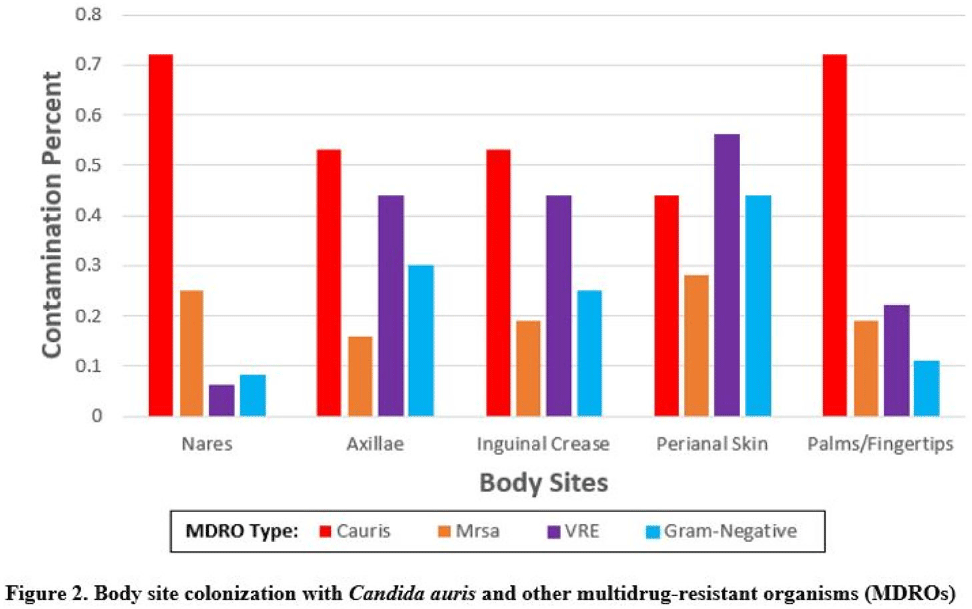
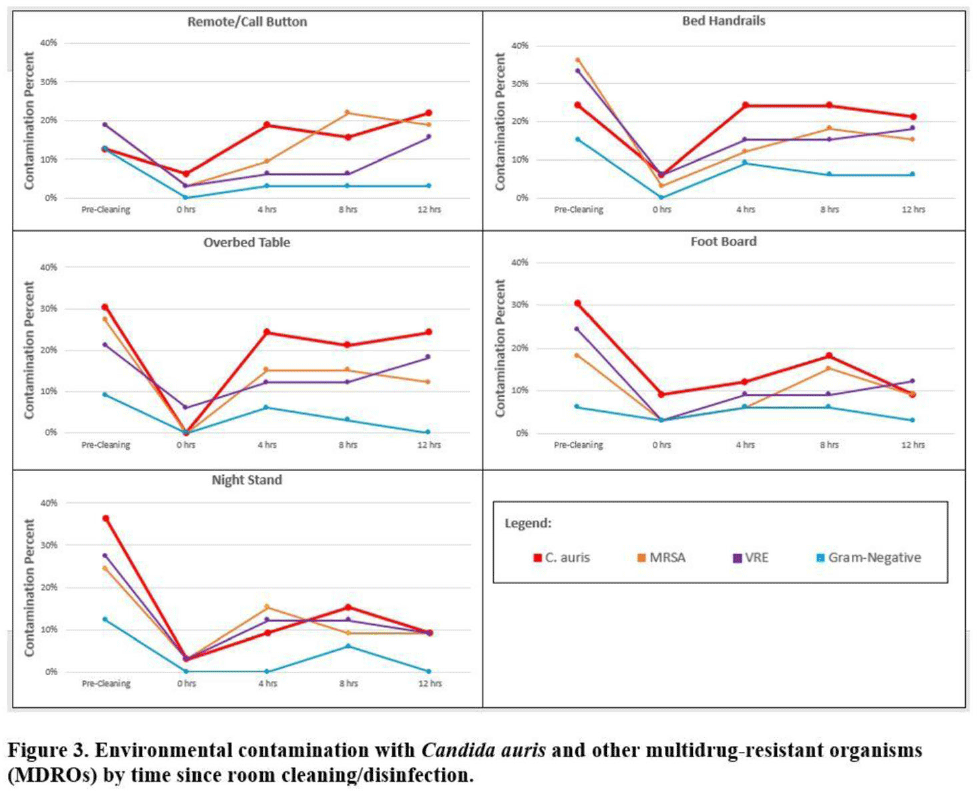
Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization – ERRATUM.
Antimicrobial Stewardship & Healthcare Epidemiology,
Vol. 2,
Issue. 1,
Didik, T.
Yau, A.P-Y.
Cheung, H.L.
Lee, S-Y.
Chan, N-H.
Wah, Y-T.
Luk, H.K-H.
Choi, G.K-Y.
Cheng, N.H-Y.
Tse, H.
Li, Y.
Wong, S.C.Y
and
Lung, D.C.
2023.
Long-range air dispersion of Candida auris in a cardiothoracic unit outbreak in Hong Kong.
Journal of Hospital Infection,
Vol. 142,
Issue. ,
p.
105.