



Introduction
Care-giving for older individuals has received considerable attention in Western societies due to individuals’ increased life expectancy, the ageing of baby boomers (Knickman and Snell, Reference Knickman and Snell2002) and the low fertility rate since the 1960s (Damiani et al., Reference Damiani, Farelli, Anselmi, Sicuro, Solipaca, Burgio, Iezzi and Ricciardi2011; Roser, Reference Roser2014). A European population projection for the period of 2016–2070 showed that in all cohorts aged 65 and older, the projected population size in 2070 will be higher than it was in 2016, and the median population age will increase by four years for men and women by 2070 (European Commission, 2018). This demographic trend, along with financial possibilities, gender roles, family relationships and organisational features, such as the availability of public and private health-care services, affect the type of care that the older population receives (Damiani et al., Reference Damiani, Farelli, Anselmi, Sicuro, Solipaca, Burgio, Iezzi and Ricciardi2011).
Healthy partners and adult children are first-line supporters who provide informal care to older relatives. Assisting in daily activities (e.g. meal preparation, giving medication, bathing and dressing, supporting an old person in preserving his or her social network) postpones admittance to an assisted living facility, nursing care facility or rehabilitation centre (Hequembourg and Brallier, Reference Hequembourg and Brallier2005). Given that baby boomers are growing older and that families are expected to have fewer children, the burden on children who take care of their parents is increasing (Tolkacheva et al., Reference Tolkacheva, Broese van Groenou and van Tilburg2010).
Most studies on intergenerational care for parents focus on the gender of adult children and on the informal care they provide. Although many of these studies show that daughters have a higher tendency than sons do to provide care for older parents (Dwyer and Coward, Reference Dwyer, Coward, Dwyer and Coward1992; Campbell and Martin-Matthews, Reference Campbell and Martin-Matthews2003; Shuey and Hardy, Reference Shuey and Hardy2003; Szinovacz and Davey, Reference Szinovacz and Davey2007; Brandt, Reference Brandt2013; Vergauwen and Mortelmans, Reference Vergauwen and Mortelmans2021), only a few have focused on the children's gender composition. Previous studies have furthermore neglected the entire parental care perspective (formal and informal) and the effect of children's gender composition on parents’ choices in allocating informal and formal care. By focusing mostly on the labour division among adult children with respect to informal care (Spitze and Logan, Reference Spitze and Logan1990; Campbell and Martin-Matthews, Reference Campbell and Martin-Matthews2003; Haberkern et al., Reference Haberkern, Schmid and Szydlik2015), researchers have paid little attention to the influence of children's gender composition on the variety of older parents’ care sources.
In our study, we address this gap in the literature by taking a multi-actor approach to care. We focus on the various types of care that parents receive and how their adult children's gender composition affects this. We distinguish between primary and secondary care-givers while highlighting the relative importance of the care source for parents.
We aim to examine whether children's gender composition influences the care type that parents use. To capture this, we distinguished four possibilities: only informal care, a combination of formal and informal care, only formal care and no care at all. Formal care is defined as receiving professional or paid services, such as Meals on Wheels, nursing home stays and professional home care providers, at least once a month from a professional care provider. Informal care, on the other hand, is defined as personal care or help with household chores at least once per month.
We also examine the reliance on the broader care network as a function of children's gender composition. To do so, we look into four types of possible informal care sources along with formal care. Partners, children, children-in-law and other (non-)relatives are considered to be the parents’ possible informal care network. Using this rich information about parents’ care sources gives us a more comprehensive understanding of the full range of care providers, the determination of the children's role in care-giving and the effect of children's gender composition on the larger care network. Therefore, we investigate the following research questions:
RQ1 Does the gender composition of adult children influence the informal and formal care type that parents receive?
RQ2 How does the gender composition of adult children affect the parental care network as a whole?
Answering these questions not only fills a gap in the literature but also gives us a better understanding of the gender dynamics within a group of adult children and their role in care provision for older parents.
The paper begins with a review of the gender composition of children and its effects on intergenerational solidarity, informal care and formal care. We then discuss the study's data and methodology. After the results, we focus on the discussion and finalise our study by drawing conclusions and proposing future research directions.
Background literature
In contemporary societies, traditional care-giving from adult children to parents has changed due to developments in family structures, demography, and societal and economical formations (Kohli, Reference Kohli1999; Giarrusso and Putney, Reference Giarrusso, Putney, Gu and Dupre2020), and these changes have made adult intergenerational solidarity more complex than in the past, which, in turn, has necessitated a more complex conceptualisation and measurement of intergenerational solidarity (Giarrusso and Putney, Reference Giarrusso, Putney, Gu and Dupre2020). Bengtson and Robert (Reference Bengtson and Robert1991) developed a model where they distinguished intergenerational solidarity into six dimensions: (a) affectual solidarity (positive feelings for each other); (b) normative solidarity (norms and expectations to support each other); (c) structural solidarity (opportunities for contact); (d) associational solidarity (contact between family members); (e) consensual solidarity (agreement on values and opinions); and, finally, (f) functional solidarity (support giving), which we mainly cover in the current paper.
During the past 30 years, a large number of articles on intergenerational solidarity have been published, with family scholars placing great emphasis on the determinants of receiving both formal and informal care. Despite the increased competition in the labour market, the greater number of women in the paid workforce and greater mobility for better job opportunities have reduced the amount of time that adult children dedicate to their parents (Bolin et al., Reference Bolin, Lindgren and Lundborg2008; Szydlik, Reference Szydlik2008; Kalmijn, Reference Kalmijn, Treas, Scott and Richards2014). Children remain the most important informal care-givers within a family network (Evandrou et al., Reference Evandrou, Falkingham, Gomez-Leon and Vlachantoni2018). On the other hand, improved care services have also enabled many people to access formal care (Da Roit, Reference Da Roit2007). Additionally, scholars have observed an increasing trend of parents wishing to be more independent from their adult children in terms of practical support and personal care (Kalmijn, Reference Kalmijn, Treas, Scott and Richards2014; Hortová and Souralová, Reference Hortová and Souralová2019). Hortová and Souralová's (Reference Hortová and Souralová2019) qualitative study showed that ageing parents stress the importance of having separate households as well as maintaining their lives without asking for help unless it is necessary.
A study on informal care provision by adult children and on the use of formal home care among ageing parents demonstrated that informal care is an important source of care and serves as an alternative to formal care as long as the needs of the ageing parents are ‘low and require unskilled type of care’ (Bonsang, Reference Bonsang2009). However, informal care can also have a complementary role vis-à-vis formal care depending on the accessibility of formal care and on existing family norms and societal structures (Bolin et al., Reference Bolin, Lindgren and Lundborg2008, Brandt et al., Reference Brandt, Haberkern and Szydlik2009; Haberkern and Szydlik, Reference Haberkern and Szydlik2010; Brandt, Reference Brandt2013). In the following subsections, we cover the various care sources for ageing parents.
Gender composition and care-giving to ageing parents
Informal care, in the context of parental care-giving, is seen as a way of preventing institutionalisation and enabling ageing parents to remain at home by providing them with the necessary support, such as meal preparation, housekeeping, financial management and the continuous supervision of parents (Horowitz, Reference Horowitz1985; European Commission et al., 2018).
A child's gender is a crucial determinant of informal care-giving to ageing parents. Continuous economic change and demographic change have occurred over the past few decades (Maume, Reference Maume2016), and progress has been made towards gender equality, which compels men to do more family care work. However, a significant amount of recent research has documented that daughters remain the primary parental care-givers compared with sons (Ingersoll-Dayton et al., Reference Ingersoll-Dayton, Neal, Ha and Hammer2003; Connidis and Kemp, Reference Connidis and Kemp2008; Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008; Ulmanen and Szebehely, Reference Ulmanen and Szebehely2015; Luppi and Nazio, Reference Luppi and Nazio2019; Vergauwen and Mortelmans, Reference Vergauwen and Mortelmans2021). They also spend more time on informal care-giving to their ageing parents than their brothers do (Gerstel and Gallagher, Reference Gerstel and Gallagher2001; Grigoryeva, Reference Grigoryeva2017).
A number of extensive studies on the effect of the gender composition of children on parent care by Matthews and colleagues documented that sibling groups that include only sisters are characterised by frequent contact and by a fairer sharing of filial responsibilities. Sisters support each other during the care-giving process (Matthews and Rosner, Reference Matthews and Rosner1988). On the other hand, examining sibling groups with only one sister revealed that daughters have more filial responsibilities related to parent care than sons do. It is also noted that brothers are more likely to ask for formal help compared with daughters (Matthews, Reference Matthews1995). Finally, Matthews and Heidorn (Reference Matthews and Heidorn1998) examined brother-only sibling groups and found that they expected their parents to contact them when they needed assistance, rather than offering help voluntarily. In these sibling groups, daughters-in-law provided hands-on care more often than sons did. In addition, brothers did not expect to meet all of their parents’ needs and combined informal care with formal care (Matthews and Heidorn, Reference Matthews and Heidorn1998). Similarly to Matthews and colleagues, Coward and Dwyer (Reference Coward and Dwyer1990) investigated three gender compositions of siblings – only children, one-gender-only siblings and mixed-gender siblings – and found that daughters tended to care more intensively in sibling groups, including in a mix of sisters and brothers. The intensity of care-giving was similar among only children compared to one-gender-only sibling groups.
More recent studies have continued to document the prominent care-giving role of daughters among children (Hequembourg and Brallier, Reference Hequembourg and Brallier2005; Connidis and Kemp, Reference Connidis and Kemp2008; Brandt, Reference Brandt2013; Grigoryeva, Reference Grigoryeva2017; Vergauwen and Mortelmans, Reference Vergauwen and Mortelmans2021). Attitudes and perceptions towards care-giving also differ between daughters and sons. Daughters not only provide more care than sons do but also their care-giving is more elastic than sons’ care-giving with regards to individual sources, limitations and parents’ characteristics (Grigoryeva, Reference Grigoryeva2017). Sons are more likely to view themselves as supervising parental care with the goal of maintaining their parents’ independence, and thus, they more often delegate the actual provision of care to someone else. Sons also tend to wait for their parents to request assistance, whereas daughters are more likely to monitor their parents consistently and to give them advice (Matthews, Reference Matthews2002; Hequembourg and Brallier, Reference Hequembourg and Brallier2005).
Social scientists have offered several explanations for the gender differences in adult children's care provisions. Among the most important explanations is women's historical caretaking role, gender identity formation and socialisation theory. The perceptions of and motivations for care-giving differ between men and women because women are taught to take on more care responsibilities, whereas men are expected to give less direct informal care (Kahn et al., Reference Kahn, McGill and Bianchi2011). As young children, women are often socialised to specialise in and to perform traditional ‘feminine’ tasks, which indicates socialisation theory. It is important to note that gender differences in care-giving do not necessarily occur due to a lack of filial responsibility among sons. Rather, they mostly arise from the cultural definition of gender-appropriate behaviour (Brody, Reference Brody1981; Allen, Reference Allen1994; Brewer, Reference Brewer2001). Kruijswijk et al. (Reference Kruijswijk, Da Roit and Hoogenboom2015) touched upon this topic from a different perspective and documented that care-giving has a multifaceted nature and that men contribute to the elasticity and stability of care arrangements by supporting female care-givers.
Some studies (Gerstel, Reference Gerstel2000; Rubinstein, Reference Rubinstein2001; Sarkisian and Gerstel, Reference Sarkisian and Gerstel2004), on the other hand, focused on Giddens’ (Reference Giddens1984) ‘structuration theory’, where he focused on the duality of the structures. Briefly, structuration theory acknowledges ‘the interaction of meaning, standards and values, and power and posits a dynamic relationship between these different facets of society’ (Gibbs, Reference Gibbs2017). Looking from the care-giving perspective, it is described that structural explanations for the gender gaps in family care often highlight the limitations and opportunities that the various employment experiences of women and men generate. Due to better job and career prospects, men often have more lucrative and time-consuming or satisfying jobs than women do. Hence, employment pulls or pushes men away from care responsibilities (Gerson, Reference Gerson1993; Sarkisian and Gerstel, Reference Sarkisian and Gerstel2004).
In addition to these theories, several researchers (Matthews, Reference Matthews, Kramer and Thompson2001; Pillemer and Suitor, Reference Pillemer and Suitor2006; Haberkern and Szydlik, Reference Haberkern and Szydlik2010; Pillemer and Suitor, Reference Pillemer and Suitor2013; Grigoryeva, Reference Grigoryeva2017) have focused on the attitudes and demands of parents and adult children. Matthews (Reference Matthews, Kramer and Thompson2001) demonstrated that parents are more likely to expect care from their daughters than from their sons. Research by Grigoryeva (Reference Grigoryeva2017: 136) documented that ‘caregiving to older parents varies not only by an adult child's own gender, but also by the gender of the siblings with whom caregiving is shared and by the gender of the parent to whom care is provided’. More specifically, she showed that daughters provide more care hours to mothers than to fathers, but they also provide more care hours than sons do regardless of the parent's gender. The number of care services is at its largest in daughter-to-mother dyads, followed by daughter-to-father dyads.
Taken together, the findings on siblings’ gender composition indicate that daughters are more involved in parental care compared with sons, although families and the labour division in families have evolved in a more egalitarian direction (Lachance-Grzela and Bouchard, Reference Lachance-Grzela and Bouchard2010). In the next section, we address the literature on the determinants of receiving informal and formal care, as well as alternative informal care networks that ageing parents can have.
Effects of children's characteristics on informal care provision
Siblings’ characteristics affect the amount of informal care that children give to their parents. The number of children is one of these characteristics. A higher number of siblings tends to increase the total amount of help provided to older parents (Wolf et al., Reference Wolf, Freedman and Soldo1997; Szinovacz and Davey, Reference Szinovacz and Davey2007). Consequently, these children each spend fewer hours caring for their parents than children with fewer or no siblings do (Igel et al., Reference Igel, Brandt, Haberkern and Szydlik2009; Szinovacz and Davey, Reference Szinovacz and Davey2013). Adult children adapt their care provision to the care that their siblings provide. Hence, the larger the sibling group, the greater the potential for informal care arrangements (Szinovacz and Davey, Reference Szinovacz and Davey2007).
The partner status of children is another important determinant of informal care-giving (Tolkacheva et al., Reference Tolkacheva, Broese van Groenou and van Tilburg2010; Leopold et al., Reference Leopold, Raab and Engelhardt2014). Although some studies have found no effect between having a partner and providing care (Wolf et al., Reference Wolf, Freedman and Soldo1997), many studies have demonstrated that children with partners devote less of their time as care-givers, whereas non-partnered children are more often involved in care-giving (Dautzenberg et al., Reference Dautzenberg, Diederiks, Philipsen, Stevens, Tan and Vernooij-Dassen2000; Pezzin et al., Reference Pezzin, Pollak and Schone2008; Haberkern and Szydlik, Reference Haberkern and Szydlik2010; Tolkacheva et al., Reference Tolkacheva, Broese van Groenou and van Tilburg2010; Leopold et al., Reference Leopold, Raab and Engelhardt2014). Looking from the gender perspective, Wiemers and Bianchi (Reference Wiemers and Bianchi2015) reported that because married daughters have more family to take care of due to the inclusion of in-laws, unmarried daughters are the ones who most likely take care of their parents.
Contact frequency and proximity are other crucial determinants that influence the informal care that adult children provide. Having frequent contact and living close to parents increase the opportunity to help them with their daily activities (Haberkern and Szydlik, Reference Haberkern and Szydlik2010). Regarding gender differences and proximity, many studies have demonstrated that when sons and daughters live at equal distance, daughters have more contact with their parents than sons do (Matthews and Heidorn, Reference Matthews and Heidorn1998; Campbell and Martin-Matthews, Reference Campbell and Martin-Matthews2003; Bolin et al., Reference Bolin, Lindgren and Lundborg2008; Szinovacz and Davey, Reference Szinovacz and Davey2007). Spitze and Logan (Reference Spitze and Logan1990) demonstrated that parents with two sons have less contact with their children than parents with one son and one daughter do. They also found that parents with two daughters have more contact compared with parents who have one daughter and one son. One reason for this trend is that daughters develop closer emotional bonds with their parents, especially with mothers, than sons do, leading to greater levels of contact and helping behaviour from daughters (Spitze and Logan, Reference Spitze and Logan1990; Grigoryeva, Reference Grigoryeva2017).
Adult children's employment status also affects the informal care they provide to their parents. Children who have competing demands from their job environments in terms of working hours have less time to enter the care-giving role (Leopold et al., Reference Leopold, Raab and Engelhardt2014). With respect to gender differences in the relationship between work and care-giving, women are more likely than men are to make accommodations in their work schedules (e.g. reducing work hours, taking time off), and they might work part-time to facilitate care-giving for their ageing parents (Starrels et al., Reference Starrels, Ingersoll-Dayton, Neal and Yamada1995; Plantenga, Reference Plantenga2002).
Depending on the need and intensity of formal care, informal care can be complementary or can serve as an alternative to formal care. Although mostly adult children provide the majority of the informal care that their parents receive, other informal care sources also exist. They are briefly covered in the next subsection.
Alternative informal care networks
Besides the care that adult children provide, partner care and the care that in-laws provide are the other most important sources of care for the ageing parents. Partners are often the first to take on care-giving responsibilities, especially in couple-only households (Pinquart and Sörensen, Reference Pinquart and Sörensen2011; Sundström et al., Reference Sundström, Jegermalm, Abellán, Ayala, Pérez, Pujol and Souto2018). Although a few studies indicate that the hours dedicated to partner care differ between women and men only when the level of partner care need increases (Glauber, Reference Glauber2017; Langner and Furstenberg, Reference Langner and Furstenberg2018), most studies that cover partner care suggest that male partners receive help from alternative care sources (Allen, Reference Allen1994) as well as formal care sources (Bertogg and Strauss, Reference Bertogg and Strauss2020) when giving aid to their partners. Meanwhile, female partners provide most of the care that partners require. Some other researchers highlighted that the demography, household structure and availability of different social services in countries are important determinants when explaining the care-giving behaviour of men and women (Abellan et al., Reference Abellan, Perez, Pujol, Sundstrom, Jegermalm and Malmberg2017; Sundström et al., Reference Sundström, Jegermalm, Abellán, Ayala, Pérez, Pujol and Souto2018).
Children-in-law, in co-operation with children, might play an important role in informal care-giving if a parent does not have a healthy partner who can look after him or her. Qualitative research by Matthews and Rosner (Reference Matthews and Rosner1988) divided in-law care into three postures: antagonism, indifference and active support. Antagonism results in no help from in-laws and even limits or stops help from adult children. In the indifference posture, in-laws show no intention to provide any informal care to their parents-in-law. However, they also do not influence the help that their partners give. Finally, active support can be seen as a form of direct support in which the daughter-in-law or son-in-law provides informal care and functions as a source of indirect support by facilitating the partner's involvement in providing parent care.
During times of active support, sons-in-law are willing to substitute for their wives, although this is rare. In contrast, daughters-in-law participate in care-giving activities more often compared with sons-in-law (Johnson and Wiener, Reference Johnson and Wiener2006; Henz, Reference Henz2009; Grundy and Read, Reference Grundy and Read2012). For example, daughters-in-law provide more hands-on care, such as meal preparation and shopping (Matthews and Heidorn, Reference Matthews and Heidorn1998), and they even perceive themselves as good assistants for daughters and as one of their parents-in-law's primary care-givers, although daughters take on more responsibility (Merrill, Reference Merrill1993).
Although family is presumed to be the most appropriate source of care, some old people might receive care from a variety of other informal care sources, such as relatives, friends, neighbours and other non-kin people (LaPierre and Keating, Reference LaPierre and Keating2013; Kalwij et al., Reference Kalwij, Pasini and Wu2014). These (non-)relatives can play a key preventative role in reducing the need for formal care (Nocon and Pearson, Reference Nocon and Pearson2000), and care-giving from these sources may occur in various ways (Croog et al., Reference Croog, Lipson and Levine1972; Himes and Reidy, Reference Himes and Reidy2000; Nocon and Pearson, Reference Nocon and Pearson2000; Barker, Reference Barker2002), such as sharing a meal and picking up groceries (Barker, Reference Barker2002). Additionally, other (non-)relatives are usually similar-age peers, not married, and unemployed or retired (Himes and Reidy, Reference Himes and Reidy2000). LaPierre and Keating (Reference LaPierre and Keating2013) differentiated friends and neighbours as alternative care sources. According to their study, friends have a higher tendency than neighbours to assist in various care tasks, such as personal care, bills and banking, and transportation. Meanwhile, neighbours were more likely to assist in tasks such as home maintenance, and their assistance encompassed only a limited number of tasks compared with friends.
Together, these studies support the notion that spousal care and care from adult children, followed by care from in-laws and other (non-)relatives, constitute the most important sources of informal care for ageing people. The most obvious pattern in the literature is that gender plays an important role in informal care and in the need for formal care.
Determinants of receiving formal care
Demographic transitions not only resulted in longer lifespans of individuals but also increased the need for long-term care for the older population. Previous research on why and the extent to which an ageing parent receives formal care services demonstrated that various reasons exist for why a parent receives more formal care than informal care. The first one is a country's cultural norms and welfare state provisions. Studies have mostly demonstrated that a family member often takes on necessary care tasks in Mediterranean and Eastern European countries, whereas outsourcing care for the older parents mostly takes place in Western Europe and Scandinavia (Damiani et al., Reference Damiani, Farelli, Anselmi, Sicuro, Solipaca, Burgio, Iezzi and Ricciardi2011; Bertogg and Strauss, Reference Bertogg and Strauss2020). The provisions of the welfare state also have an effect on the care composition given to the old people. Motel-Klingebiel et al. (Reference Motel-Klingebiel, Tesch-Roemer and Von Kondratowitz2005) showed that the ageing populations in countries where welfare state provisions are more comprehensive and accessible often receive a combination of informal and formal care. The second determinant is the level of care need of older parents. Parents who have serious functional limitations or experience degenerative conditions tend to receive more professional help (Broese van Groenou et al., Reference Broese van Groenou, Glaser, Tomassini and Jacobs2006; Kjær and Siren, Reference Kjær and Siren2020). The third explanation highlights well-documented individual predictors of the intergenerational solidarity of both parents and children. Parents who do not receive informal care tend to substitute informal care with formal care, or they use a combination of the two. For example, research demonstrates that parents with a high socio-economic status have less contact with their children and are better able to purchase private help. They therefore receive formal care more often than they do informal care (Broese van Groenou et al., Reference Broese van Groenou, Glaser, Tomassini and Jacobs2006; Kalmijn, Reference Kalmijn, Treas, Scott and Richards2014; Ulmanen and Szebehely, Reference Ulmanen and Szebehely2015; Kjær and Siren, Reference Kjær and Siren2020). In addition, the aforementioned predictors, such as employment, proximity, gender and family sizes, are indicated as formal care determinants of ageing parents.
Hypotheses
The gendered nature of the care-giving that adult children provide to their parents has been studied extensively. We take this a step further and examine whether gender composition influences parental care, as well as the various care networks utilised. To answer our research questions, we established the following hypotheses:
H1 Parents who have more sons tend to receive more formal care.
H2 Parents who have daughters are more likely to receive informal care from children than parents with sons do.
H3 Parents who have more sons are more likely to use their children-in-law as an informal care source.
H4 Parents who have sons have a higher tendency to use more other (non-)relatives as care sources.
Data and methodology
We use data from the Survey of Health, Ageing and Retirement in Europe (SHARE). SHARE is a multi-disciplinary and cross-national panel database providing microdata on the health, socio-economic status, and social and family networks of individuals aged 50 and older (Börsch-Supan et al., Reference Börsch-Supan, Brandt, Hunkler, Kneip, Korbmacher, Malter, Schaan, Stuck and Zuber2013). So far, the SHARE panel design covers the period between 2004 and 2020. To answer the research questions, we used Wave 6, which was conducted in 2015 in Austria, Germany, Sweden, Spain, Italy, France, Denmark, Greece, Switzerland, Belgium, Israel, Czech Republic, Poland, Luxembourg, Portugal, Slovenia, Estonia and Croatia. Our data focused on the household level, and we retained data only from respondents who answered the questionnaire on behalf of their households (family respondents) and had at least one child. We omitted children below the age of 16. After these adjustments, the sample includes 40,312 respondents.
For the analyses, we applied multinomial logistic regression to examine the effect of children's gender composition on the care type (informal versus formal) that the parents used, as well as to observe the effect of gender composition on the parents’ informal care network (children, in-laws, friends, etc.). Apart from the two outcome variables and the variable of interest, the models included control variables at the child and parent levels. At the child level, we controlled for characteristics such as contact with parents, residential proximity to parents, employment status and marital status. At the parent level, we controlled for socio-demographic background and health status.
Dependent variable
We established four hypotheses to answer our research questions. To test these hypotheses, we constructed two outcome variables: care type and care network. We used the care type variable for examining H1; it indicates whether respondents received only informal care, a combination of formal and informal care, only formal care or no care at all. Respondents received informal care if they indicated getting personal care or help with household chores at least once per month during the 12 months preceding the Wave 6 interviews. Respondents received formal care if they indicated getting professional or paid services from a professional care provider at least once per month in the same period.
To construct our second outcome variable, care network, addressing H2, H3 and H4, we first identified the particular sources of informal care (e.g. partners, children, other family members, friends, colleagues, etc.) that parents received (for personal care or help with household chores) from inside or outside the household. In addition, we considered parents’ use of formal care (professional personal care, paid help with household chores and stays at a nursing home). Subsequently, we sorted the informal care sources based on the frequency of care-giving to distinguish primary and secondary care-givers. Using a latent class analysis (LCA), we found five prominent care sources that parents use: ‘partner care’, ‘children’, ‘children-in-law’, ‘other (non-)relatives’ and ‘only formal care’. The LCA yielded a best-fitting model of five of the presented classes for those receiving informal or formal care. Although the LCA suggests a separate class comprising formal care only, combinations between informal care sources and formal care render a great deal of infrequent categories (about 25% of each informal care source is combined with formal care). For the simplicity and feasibility of the multivariate analysis, this level of detail is not reflected in the dependent variable. In addition, from the analysis, it is clear that the categories of secondary care-givers are mostly the same as those for the primary care-givers, leading to no substantial patterns of a different primary and secondary care source. To cover all respondents, we added a separate category consisting of those receiving ‘no care at all’ in addition to the five care sources identified using LCA, leading to a dependent variable of six categories.
Independent variables
We present the independent variables in three groups: variable of interest, children characteristics and parental characteristics.
Since the main focus of this study is to understand how the gender composition of siblings influences the care type and care network of parents, this article's variable of interest is gender composition of children. This variable has seven categories: (1) daughter as only child, (2) son as only child, (3) as many daughters as sons, (4) more than half of the siblings are daughters, (5) more than half of the siblings are sons, (6) only daughters, and (7) only sons. With the help of this categorical variable, we could observe whether having more or less daughters or sons has an influence on the care type and care network of parents.
Before introducing children characteristics, it is crucial to highlight that all individual characteristics are averaged over the total number of children. Numeric characteristics yield an average score (e.g. contact frequency and proximity), whereas dichotomous information (e.g. employed or not) translates into proportions. The children characteristics Footnote 1 covered in this article are education (proportion highly educated), partnership status (proportion having a partner), employment status (proportion employed) and parental status (proportion having a child).Footnote 2 Further, we averaged contact frequency per year between children and parents, starting from the following categorisation: (1) 365 days, (2) 156 days, (3) 52 days, (4) 24 days, (5) 12 days, (6) 6 days, and (7) 0 days. The averaged geographic parent–child proximity was calculated from the individual categorisation encompassing (1) 0 kilometres (km) (which corresponds to child(ren) living in the same building or less than 1 km away from their parents), (2) 3 km, (3) 15 km, (4) 63 km, (5) 300 km, and (6) 750 km. Financial helpFootnote 3 is introduced by dichotomies expressing whether children received gifts from or gave gifts to parents of at least €250 in the 12 months before the interview.
We included several parental characteristics in the analyses. Age, gender, education, partnership status, number of children and employment status provided the basic background information about the respondents. The number of limitations with activities of daily living (ADL), such as getting out of bed, buying groceries, bathing, and so on, is used as a measure of parental health. The ADL scale ranges from 0 (no limitations) to 6 (limited with respect to all activities). In addition, a binary variable reflects whether the parents were hospitalised in the 12 months preceding the interview or not: 1 indicates that the respondent stayed overnight in a hospital in the last 12 months and 0 indicates no hospitalisation. Another binary variable reflecting whether the parents were born in the country where the interview was held or not is also added. The proportion of biological children indicates what share of children are biological or not.
Results
Descriptive results
To understand the whole perspective and the effects of siblings’ gender composition on parental care, we constructed two categorical outcome variables. The first outcome variable is care type. To capture all possible care types, we constructed a variable including four categories: no care at all, only formal care, a combination of formal and informal care, and only informal care. As shown in Table 1, 76 per cent of the respondents use no care at all, whereas the rest use only formal care, a mixture or only informal care (i.e. 5, 5 and 14%, respectively). The second outcome variable is care network, where we used six categories to identify parents’ care network. Five per cent of the sample receive formal care, whereas 10 per cent are looked after by their children, and the rest get care either from their partners, children-in-law or other (non-)relatives (i.e. 3, 1 and 5%, respectively).
Table 1. Descriptive statistics

Notes: Observations are based on respondents with at least one child. SD: standard deviation. ADL: activities of daily living.
Source: Survey of Health, Ageing and Retirement in Europe (Wave 6, release 7.00), calculation by the authors.
The gender composition of children demonstrates that around 21 per cent of the parents have either a daughter as an only child (10.5%) or a son as an only child (10.4%). Also, 27 per cent have as many daughters as sons, whereas 11 per cent have more daughters than sons and 12 per cent have more sons than daughters. The percentages of parents having only daughters and only sons as children are 14 and 15 per cent, respectively.
Looking at respondent characteristics, 62 per cent of our respondents are female. More than half of the respondents are partnered (standard deviation (SD) = 0.48). Overall, the average number of children is 2 (SD = 1.20). Most respondents do not have any restrictions, such as dressing, bathing, preparing a meal and shopping for groceries, in their daily activities (ADL mean = 0.28, SD = 0.93), and they consequently reported a low degree of hospitalisation, with 15 per cent being hospitalised in the last 12 months. One-quarter of the respondents are employed, and almost 90 per cent were born in the country where the interviews were held. A vast majority have biological children. Moving on to children characteristics, most children live far away from their parents (mean = 94.3 km, SD = 159.3), with a relatively high parent–child yearly contact rate (mean = 198.2, SD = 121.8). More than half of the children are married, employed and have at least one child. Very few of them receive or give financial means to/from their parents.
Results of the care type model
In our first model, we tested the first hypothesis using multinomial logistic regression (cf. Table 2). The multivariate analysis draws on the non-missing information of 33,984 parents. The model considers ‘only informal care’ as the reference category for the dependent variable care type and ‘only daughters’ are chosen to be the reference category for the gender composition of children. When interpreting the results, we will be comparing each category with the reference category.
Table 2. Multinomial logit regression results (dependent variable: care type)
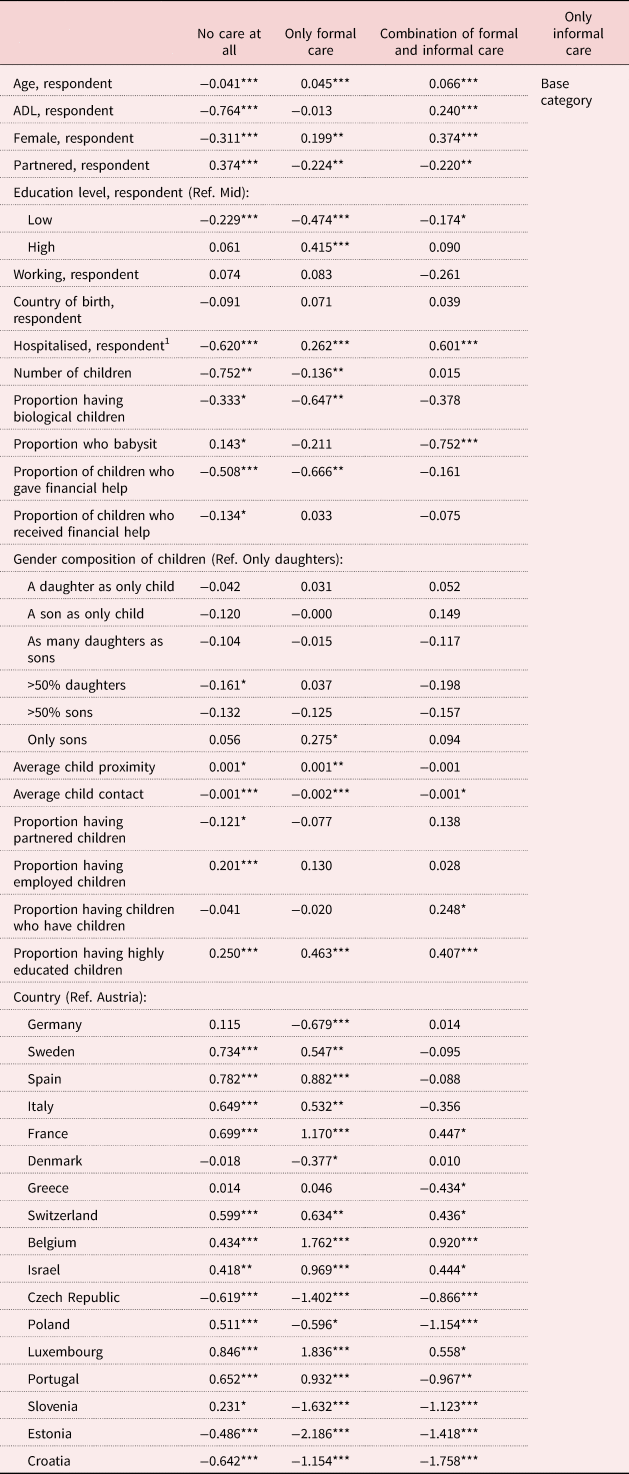
Notes: N = 33,984. 1. During the last 12 months. ADL: activities of daily living. Ref.: reference category.
Source: Survey of Health, Ageing and Retirement in Europe (Wave 6, release 7.00), calculation by the authors.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
We expected that parents with more sons tend to receive more formal care (H1). However, the results demonstrated that the gender composition of children has very little effect on the care type that parents receive. We found that, compared to parents with only daughters, parents tend to have more informal care rather than no care if they have more daughters than sons (b = −0.161, p < 0.05). Furthermore, parents with only sons have a higher likelihood of receiving only formal care (b = 0.275, p < 0.05). Although this is an effect that we expected, the significance level is moderate.
Looking at the direction of the effects, we observe that parents with only children and any composition, including daughters, tend to receive informal care more instead of no care at all. Additionally, instead of receiving only informal care, a combination of formal and informal care is more common among parents with only children and parents with only sons. It is important to stress that these are only the direction of effects and are not statistically significant.
Moving on to the other factors that affect care type, we saw that in comparison to only informal care, parents have a higher tendency to receive only formal care or a combination of care when they are older, female, single and hospitalised during the last 12 months. The number of children is also key to informal care for parents. Although the effect is small, results showed that children with their own children tend to use more of a combination of formal and informal care. Parents’ and children's educational attainment has a strong and positive effect, meaning that the likelihood of receiving only formal care is higher when both the parents and children are highly educated. Looking at other children characteristics, we found that if the proportion of employed children is high, parents have a higher likelihood of receiving no care at all as compared to informal care. While having a partner and having less contact with children lower their chances of receiving informal care, receiving financial help from children increases parents’ chances of getting informal care instead of no care at all or only formal care.
In summary, regarding the care type model, we examined the effect of children's gender composition on parents’ care type and expected to find that parents receive more formal care if they have more sons. Although the direction of the effects implied what we expected, we observed limited evidence for their statistical significance, suggesting only weak relationships. Therefore, hypothesis H1 is not confirmed.
Results of the care network model
Table 3 presents the results of the multinomial logistic regression models through which we tested the last three hypotheses. The model considers ‘care by children’ as the reference category of the care network. For gender composition of the children, ‘only daughters’ is assigned as the reference category.
Table 3. Multinomial logit regression results (dependent variable: care network)

Notes: N = 33,984. 1. During the last 12 months. ADL: activities of daily living. Ref.: reference category.
Source: Survey of Health, Ageing and Retirement in Europe (Wave 6, release 7.00), calculation by the authors.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Based on the existing literature, we expected that parents with daughters are more likely to receive informal care by children than parents with sons (H2). Comparing parents with only daughters to sons as only children shows that parents are more likely to receive partner care (b = 0.477, p < 0.05), children-in-law care (b = 1.066, p < 0.001) or care from other (non-)relatives (b = 0.628, p < 0.001) than children care. These parents not only have a higher tendency to get informal care from other sources than their son but also get more formal care (b = 0.391, p < 0.01). If more than half of the children are daughters, the parents have a higher likelihood of receiving care from their children than from partner care or no care at all (b = −0.405, p < 0.05 and b = −0.245, p < 0.01, respectively). Further comparison between parents with only daughters and parents with only sons revealed that the latter tend to receive more children-in-law (b = 0.750, p < 0.01) and partner care (b = 0.330, p < 0.05). Parents with only sons are also more prone to receive formal care (b = 0.387, p < 0.01). Based on these results, hypothesis H2 is confirmed.
Examining further the relationship between gender composition and the care network, we address the effect of having sons on making daughters-in-law involved in the provision of informal care to parents (H3). The results revealed that parents with sons as only children receive care from their daughters-in-law (b = 1.066, p < 0.001). Turning now to children with more than 50 per cent sons, parents also receive more help from their children-in-law (b = 0.585, p < 0.05). Comparing only daughters with only sons shows that parents with only sons are more likely to receive more care by their children-in-law than parents with only daughters (b = 0.750, p < 0.001). In short, daughters-in-law play a very important role in care for parents when there are fewer daughters in the family, particularly in families with sons only. Hence, we confirmed hypothesis H3.
Next, we examine whether having sons leads parents to receive more other (non-)relatives care, and we found that it is more likely for parents to have either care from their friends, colleagues or neighbours (b = 0.628, p < 0.001) when parents have sons as their only child. However, if parents have more sons than daughters (>50% sons), it is less likely that the parents receive other (non-)relatives care (b = −0.310, p < 0.05). Taken all together, hypothesis H4 is confirmed as well.
There are other factors affecting parents’ care network. The results suggest that parents with a higher number of children tend to receive care from their children. Parents who got financial help from their children received less formal or partner care and more children care. Further, if the proportion of biological children is high, the likelihood of using any other care network than children is low. An increased chance of receiving formal care prevails if parents have children with high educational attainments and children who live far away from them. If children are partnered, getting care from children-in-law is more likely.
Lastly, parent–child contact and proximity are most important for care by children and children-in-law. All other care options are more likely if contact is lower or children live farther away.
Discussion
As the European population ages, the need for care for the ageing parents is expected to increase. Longer life expectancy (Knickman and Snell, Reference Knickman and Snell2002), reductions in family size (Lo Sasso and Johnson, Reference Lo Sasso and Johnson2002) and change in family structures (Connidis and Barnett, Reference Connidis and Barnett2018) have led researchers to question how informal care-giving is organised for older parents. There is substantial evidence that daughters are more involved in providing care for their parents than their sons (Hequembourg and Brallier, Reference Hequembourg and Brallier2005; Luppi and Nazio, Reference Luppi and Nazio2019; Vergauwen and Mortelmans, Reference Vergauwen and Mortelmans2021). Adding to this existing knowledge, the current study examined the entire care perspective for older people with children. Specifically, we tested whether the gender composition of adult children influences the care types that parents use and whether this composition also affects the parental care network. Using detailed care types and care networks, as well as including a detailed categorisation of gender compositions, we were able to distinguish the importance of having daughters in parental care-giving.
To study how adult children's gender composition influences the balance between informal and formal care use, we hypothesised the effect of having more sons than daughters on parents’ tendency to get informal care. Our results suggest that parents with only sons have a higher likelihood of receiving only formal care than parents with only daughters. We also found that parents with more daughters than sons tend to have more informal care rather than no care. Contrary to our expectations (H1), the results on the effect of gender composition of children on care types show only weak statistical significance for the above-mentioned families. We could not find any significant results for the other types of gender compositions.
A possible explanation for this might lie in respondents’ characteristics. Looking at the respondents’ profile (cf. Table 1), it is apparent that most of the parents are in good health, mostly partnered, educated and not very old. They are not in a position where they need care in general. In the literature, many studies demonstrated that these characteristics indicate more independence in parents’ lives and, therefore, might cause less or no care needs (Rossi and Rossi, Reference Rossi and Rossi1990; Kalmijn, Reference Kalmijn2006; Szinovacz and Davey, Reference Szinovacz and Davey2007; Bertogg and Strauss, Reference Bertogg and Strauss2020).
Further, we focused on finding the differences in the parental care network resulting from children's gender compositions. We expected that parents who have more daughters are more likely to lean on their children as an informal care source. The results show that the informal care network of parents strongly depends on the gender composition of their children. A comparison between parents with only daughters and parents with a son as the only child revealed that the latter tend to receive more formal care. Moreover, we found that parents with only sons receive more formal help compared to only daughters. Results also suggest that receiving partner care and no care at all is less likely when parents have more daughters than sons in their family. In accordance with the present results, previous studies have demonstrated the association between having daughters and receiving more informal care from children (Matthews and Heidorn, Reference Matthews and Heidorn1998; Shuey and Hardy, Reference Shuey and Hardy2003; Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008; Vergauwen and Mortelmans, Reference Vergauwen and Mortelmans2021). One of the most accepted explanations for this by many researchers is that the involvement of having daughters and sons in informal care is divided through the socialisation theory of gender, which emphasises deeply entrenched, distinctive roles for men and women (Matthews and Heidorn, Reference Matthews and Heidorn1998; Hequembourg and Brallier, Reference Hequembourg and Brallier2005; Da Roit, Reference Da Roit2007; Davis and Greenstein, Reference Davis and Greenstein2009).
Moreover, we put emphasis on having sons and its effect on involving daughters-in-law as a care-giver to parents. Previous studies (Matthews and Heidorn, Reference Matthews and Heidorn1998; Henz, Reference Henz2009; Wiemers and Bianchi, Reference Wiemers and Bianchi2015; Evandrou et al., Reference Evandrou, Falkingham, Gomez-Leon and Vlachantoni2018) have emphasised the contribution of daughters-in-law in parental informal care-giving. Our results are similar to those previous observations and show that sons as only children use help from their wives to give paternal care. The same holds for families with more sons than daughters and families with only sons. Merrill (Reference Merrill1993) explained that daughters-in-law are often perceived and perceive themselves as a part of the family; hence, their involvement in parental care-giving is natural. Daughters-in-law substitute for daughters in male-dominated children groups.
Lastly, we examine the connection between having sons and receiving more other (non-)relatives care. As expected, we found that parents with sons as only children receive more other (non-)relatives care. However, for families with more sons than daughters, it is not likely for parents to get care from other (non-)relatives. Matthews and colleagues provided several possible explanations for this. First, sisters are usually viewed as family care-givers by brothers. Second, daughters are seen by themselves and by sons (brothers) as being in charge when they make an attempt to divide informal care-giving responsibilities among themselves and sons (Matthews, Reference Matthews1995, Reference Matthews2002). Therefore, having at least one daughter in the sibling group is often the key to receiving informal care from children.
Conclusion
The present study was designed to determine the effect of adult children's gender composition on parental care. First, we examined the effect of gender composition on the care types (informal care, formal care, combination of both and having no care) and found very few and weak statistically significant results. Thereafter, we focused on testing the same effect on care networks (care given by a partner, children, in-laws, other (non-)relatives, and receiving only formal or no care) of parents. A comparison of different gender compositions has shown that parents with more daughters are more often observed to count on children as an informal care source. It was also revealed that if parents have no daughters, the daughters-in-law are strongly involved in parental informal care. In other words, daughters-in-law substitute for daughters. Further analysis suggests that parents have a higher tendency to rely on care by other (non-)relatives if they have a son as their only child.
This work has been the first to examine thoroughly the effect of adult children's gender composition on parental care by focusing on various types of care and care networks at the same time. By doing so, we took a step further towards explaining why and how daughters play a crucial role in care for older parents and shed new light by looking into more care sources rather than only focusing on children.
The generalisability of the results is subject to certain limitations. First, capturing formal care is limited to what is offered in SHARE data. Formal care in our study only includes professional personal care, paid help with household chores and stays at a nursing home. However, in some European countries a substantial share of the older people receives state allowances (i.e. cash-for-care) to financially compensate informal care, which can also be perceived as formal care. Capturing detailed information on parents’ formal care use could help us to obtain a better understanding of the complementary and substitutionary role of informal help. A second limitation concerns the temporal aspect of our results. By adopting a longitudinal research setting, future research will not only explore a snapshot of the gender effect on parental care, but also how care potentially changes over the lifecourse of parents. Second, examining quantitative data did not enable us to observe detailed information on the process behind care-giving decisions within families.
Further research could assess the long-term effects of the gender composition of parental care. This will allow us to observe the impact of adult children's gender on the care changes of parents. The field of research on care sources would also gain from deeper insights into country differences. However, in the present study, we only controlled for the country of living. One of the reasons for this is that the current analysis gives us more data to look into care regimes and gender compositions in detail, which is not possible with country-specific analyses. Lastly, we could not find a strong significant effect of various types of adult children's gender compositions on the care types that parents receive. More work is needed to fully understand the reasons behind this result.
Despite the limitations, the current study demonstrates that daughters and daughters-in-law play a crucial role in parental care. While parents with sons are receiving help from different formal and informal sources, parents with daughters tend to receive care from their children more often. In the absence of daughters, it is often the daughters-in-law who take up the care-giving responsibility for parents.
Financial support
This work was supported by the Flemish Science Fund (FWO) (grant number G017319N).
Conflict of interest
The authors declare no conflicts of interest.




 Open access
Open access