
8 results
S. aureus Surveillance and Decolonization Associated with Decreased MRSA, but not MSSA, Infections in the Neonatal ICU
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s117-s118
-
- Article
-
- You have access
- Open access
- Export citation
-
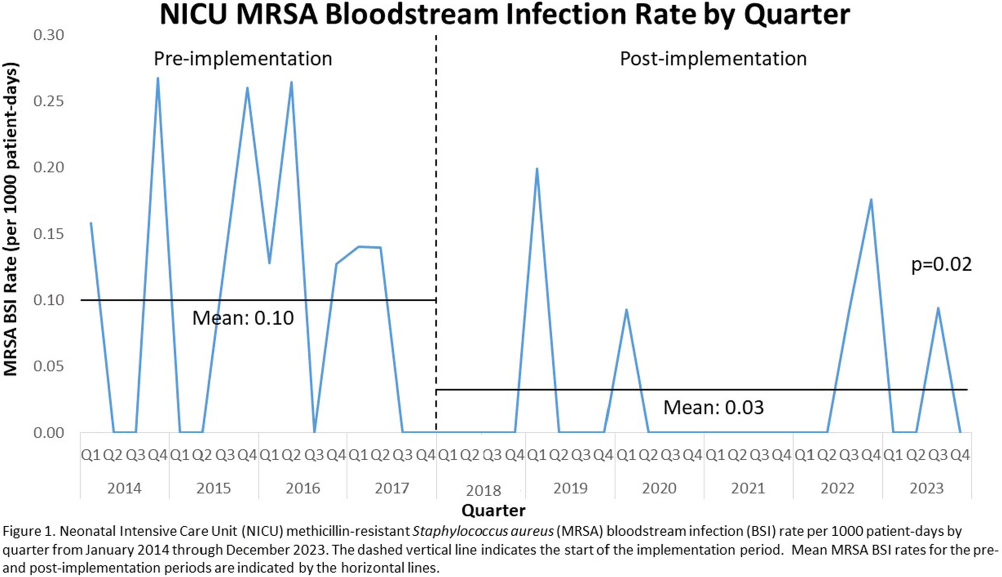
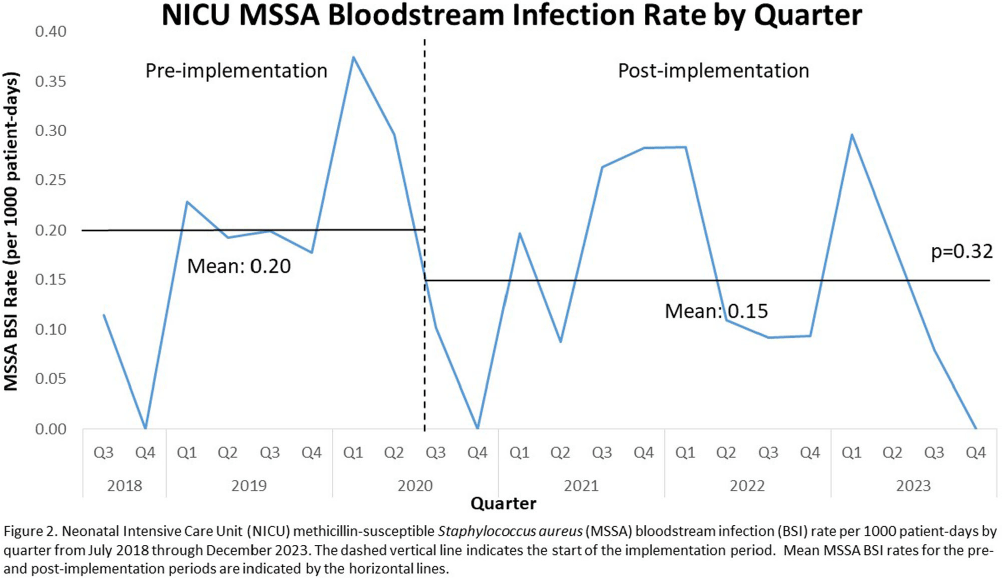
Background: Invasive Staphylococcus aureus infections cause significant morbidity and mortality in neonatal intensive care unit (NICU) infants.1 Colonization (asymptomatic carriage in the nose, skin, or gut) is a risk factor for subsequent invasive infection (e.g., pneumonia, bone infections, bloodstream infections, etc.). Active surveillance and decolonization measures for S. aureus-colonized infants have been associated with decreased invasive infection rates. 2-4 Methods: A methicillin-resistant S. aureus (MRSA) surveillance and decolonization program, consisting of admission and weekly MRSA nasal cultures followed by intranasal mupirocin plus chlorhexidine baths for colonized infants, was implemented in our level IV NICU with 150 beds in 2006.5 Due to poor compliance with decolonization protocols5, existing practices were reviewed and multiple interventions to increase compliance were implemented in 2018. These renewed efforts included revision of the existing MRSA decolonization protocol, updating the associated electronic medical record order set, re-education of unit staff, and weekly review by the Infection Prevention (IP) and NICU leadership teams to ensure the decolonization protocol was followed for newly colonized infants. Mean MRSA bloodstream infection (BSI) rates were calculated quarterly pre- (January 2014-December 2017) and post- (January 2018-December 2023) implementation of renewed efforts and compared via unpaired t-test. In July 2020 a similar methicillin-susceptible S. aureus (MSSA) surveillance and decolonization program was implemented with an associated revision of existing documents, education campaign, and weekly review of infants with new MSSA colonization. Mean MSSA BSI rates pre- (July 2018-June 2020) and post- (July 2020-December 2023) implementation were compared via unpaired t-test. Results: Renewed implementation of MRSA surveillance and decolonization was associated with a sustained decrease in the mean MRSA BSI rate (Figure 1): 0.10 per 1000 patient-days pre-implementation, 0.03 post-implementation (p=0.02). Following implementation of MSSA surveillance and decolonization, there was no statistically significant change in the mean MSSA BSI rate (Figure 2): 0.20 per 1000 patient-days pre-implementation, 0.15 post-implementation (p=0.32). Conclusions: Implementation of a robust MRSA surveillance and decolonization program in the NICU was associated with a sustained decrease in invasive MRSA infections. No change in invasive MSSA infection rates was observed following implementation of a similar protocol for MSSA. Additional research is needed to better understand the role of MSSA surveillance and decolonization in the NICU.
References: 1. Ericson, J.E., et al., JAMA Pediatr, 2015. 2. Popoola, V.O., et al., ICHE, 2016. 3. Kotloff, K.L., et al., Pediatrics, 2019. 4. Voskertchian, A., et al., ICHE, 2018. 5. Reich, P.J., et al. Clin Microbiol Infect, 2016.


Healthcare worker perceptions surrounding Staphylococcus aureus transmission and prevention practices in the neonatal intensive care unit
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 05 June 2023, pp. 1953-1958
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Pediatric research priorities in healthcare-associated infections and antimicrobial stewardship
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 5 / May 2021
- Published online by Cambridge University Press:
- 26 November 2020, pp. 519-522
- Print publication:
- May 2021
-
- Article
- Export citation
4054 Telemedicine Infectious Diseases Consultation in Rural Hospitals: Feasibility, Acceptability, Appropriateness, and Implementation
-
- Journal:
- Journal of Clinical and Translational Science / Volume 4 / Issue s1 / June 2020
- Published online by Cambridge University Press:
- 29 July 2020, p. 146
-
- Article
-
- You have access
- Open access
- Export citation
Reply to Herigon and Newland
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 33 / Issue 2 / February 2012
- Published online by Cambridge University Press:
- 02 January 2015, pp. 208-210
- Print publication:
- February 2012
-
- Article
-
- You have access
- Export citation
Effectiveness of Measures to Eradicate Staphylococcus aureus Carriage in Patients with Community-Associated Skin and Soft-Tissue Infections: A Randomized Trial
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 32 / Issue 9 / September 2011
- Published online by Cambridge University Press:
- 02 January 2015, pp. 872-880
- Print publication:
- September 2011
-
- Article
- Export citation
